Nonsurgical Correction of Severe Skeletal Class III Malocclusion
Optimal treatment of a Class III malocclusion with skeletal disharmony requires orthognathic surgery complemented by orthodontics.1 Treating such cases becomes much more challenging when the patient rejects surgery due to fear, cost, or esthetic concerns, but continues to expect a good result.
Several treatment options have been proposed for these types of cases,2,3 including extraction (usually premolars in the lower or both arches),1,4,5 extraoral traction (horizontal traction of the mandibular arch, or vertical traction in an open-bite case), and distalization of lower molars with devices such as lip bumpers.6-8 The use of an expansion device following a midline maxillary osteotomy has been advocated for treatment of the crossbite that is commonly found in non-growing Class III patients.9,10
This article describes two cases, one with a deep bite and one with an open bite, that were treated using an innovative nonsurgical treatment method for extreme skeletal Class III malocclusions. Surgical correction with orthodontic finishing was recommended in each case, but the patients and their families were vehemently opposed to surgery. The patients did want to resolve their dental malpositions and the esthetic impact of their prognathism, but they also expressed a desire to preserve the facial characteristics specific to their individual identities, referred to here as the "facial icon". Since skeletal and neuromuscular patterns are intrinsic traits of the facial icon, we agreed that only extrinsic traits - the dentition, alveolar bone, functional skeletal position, and soft-tissue and facial characteristics - would be modified by orthodontic treatment. With the possibility of adjusting the dentoalveolar interface11 to the skeletal disharmony, the overall objective in each case was to recover proper mastication and speech function, improve the prognathism, and balance the face and smile.
Similar articles from the archive:
Appliance Design
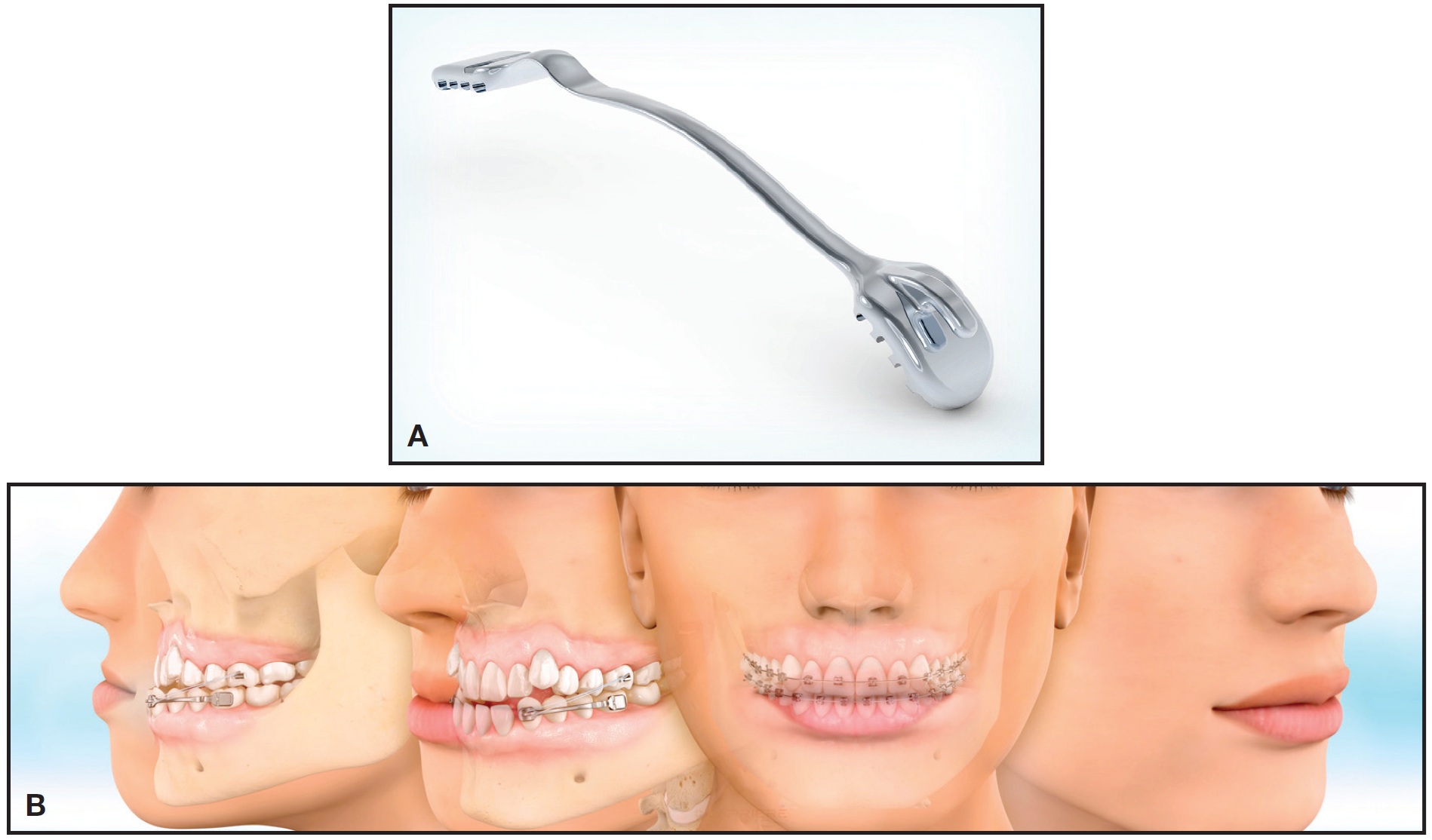
The design of the Carriere Class III Motion Appliance* was based on the same principles of respect for human biology and the concepts of simplicity,12 biomimetics,13,14 and biominimalism15 as the Carriere Class II Motion Appliance*.16 The anterior segment has a pad that bonds directly to the lower canine, with a hook for attachment of Class III elastics. An arm extends distally over the two lower premolars, with a slight curve following the contours of the dental arch, and is bonded to the lower first molar by means of a distal pad. This rigid, half-round arm controls the lower canines while directing movement longitudinally. Between the second premolar and first molar, it diminishes in size and forms an offset with a bayonet bend and toe-in angle, designed to produce a mild 10º distal rotation of the first molar. The bayonet bend has multilateral flexion to closely fit the patient's anatomical structure and facilitate the rotation; the posterior segment is flat to avoid interference with the maxillary teeth or brackets.
Class III intraoral elastics connect the appliance with maxillary anchorage (either bonded appliances or a vacuum-formed retainer) to activate the mandibular posterior segment, moving it bodily into what we call the "Class I platform" - a perfect intercuspation from the canines to the molars, in which centric relation coincides with centric occlusion. This movement is based on the histological condition of the lower posterior dentoalveolar corridors, composed of low-density, highly vascular trabecular bone surrounded on either side by compact, high-density bone.
It should be noted that the Carriere Class III Motion Appliances used in the cases presented here were prototypes fabricated from transparent polysulfone, free of bisphenol A. The appliance has since been produced in a metallic version and is now commercially available.
Treatment Sequence
Stage one with the Carriere Class III Motion Appliance involves treating the malocclusion to a Class I platform by distalizing each mandibular posterior segment, from canine to molar, as a unit. The mandible is simultaneously repositioned for an improved sagittal relationship by counterclockwise movement of the posterior occlusal plane. By the end of stage one, when the Class I platform is achieved, the lower canines will have been distalized enough to provide space for proper repositioning of the lower incisors, as determined by the diagnosis. The appliance will also have intruded the lower molars while extruding the canines - both necessary in Class III correction to change the mandibular occlusal plane and distally reposition the mandible for a better functional and esthetic relationship. To a certain degree, the appliance will alter the relationship between the maxilla and the mandible by bringing the posterior occlusal plane into a better functional position and thus balancing the face.
In stage two, treatment is finished using Carriere SLX** .022" preadjusted, passive self-ligating brackets in conjunction with thermally activated Cu Nitanium* wires.17 The use of small, round archwires at the start of treatment avoids binding, so that low forces can express themselves freely without the competing vectors that can arise with conventionally ligated brackets. Initial archwires are calibrated at a transformation temperature of 27ºC, and larger wires at 35ºC, each programmed at the appropriate time to limit force on the periodontium.
Any metabolic process in the human body requires the consumption of energy from nutrients and oxygen in the area where it is produced. The purpose of beginning with round, ultralight thermal archwires in large, passive self-ligating bracket lumens is to mildly stimulate a physiological effect in the metabolism of bone resorption and apposition. Low forces tend to promote efficient vascular dilation of the capillary network and thus stimulate an increase in the local blood supply in areas where tooth movement is needed. The intent is to avoid compromising oxygen delivery to the periodontal ligament, minimizing compressive forces that may reduce cellular turnover and promote undermining bone resorption.
Case 1
An 18-year-old male presented for treatment of mandibular prognathism (Fig. 2). His chief complaint was chewing difficulty, and he expressed a strong desire to improve his esthetic appearance.
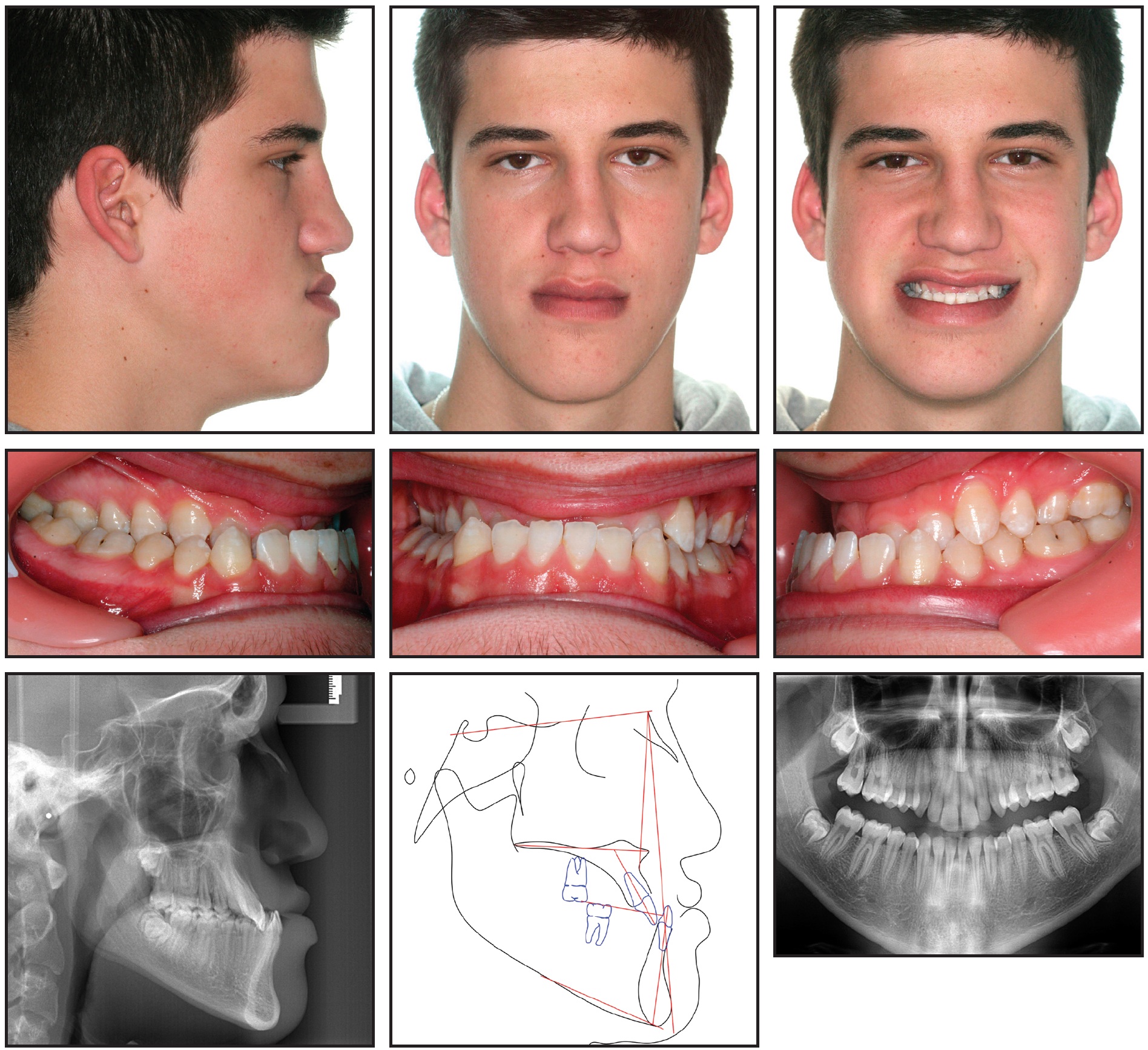
Fig. 2 Case 1. 18-year-old male with severe skeletal Class III malocclusion, full lateral and anterior crossbites, and midline shift to right before treatment.
Facial esthetics were dominated by the mandibular prognathism; the deviation to the right; and a crooked smile with a short, retrusive upper lip. The frontal view showed a mild facial hemiatrophy on the right side and a mild hemifacial hyperplasia on the left, with menton positioned slightly to the right. In terms of muscular balance and function, we observed hypertonicity in the transverse musculature of the upper lip, as well as macroglossia with tongue thrust at deglutition. At rest, the tongue posture was in the floor of the mouth, modeling the lower incisors into a forward position. The patient had extreme mastication difficulty, mainly due to the right lateral and anterior crossbites. Prior to orthodontic treatment, the patient underwent myofunctional therapy to correct his tongue function.
The maxillary arch was bonded with Carriere SLX .022" passive self-ligating brackets and .022" edgewise molar tubes. Leveling and alignment were initiated on a round .014" Cu Nitanium (27ºC) archwire with miniature stops crimped mesial to the second-molar tubes. To increase the length of the maxillary dental arch by adding wire length, each stop was activated 5mm (two-thirds the length of the tube). Composite bite ramps were bonded to the lingual aspects of the four lower incisors to prevent them from occluding with the upper-incisor brackets, simultaneously intruding the upper incisors to correct their extreme extrusion and extruding the upper molars to balance the lower third of the face.
Six weeks later, an upper .014" × .025" Cu Nitanium (27ºC) archwire was engaged, and a Carriere Class III Motion Appliance was bonded in the mandibular arch (Fig. 3).

Fig. 3 Case 1. After six weeks of initial leveling and alignment, upper .014" × .025" Cu Nitanium* (27°C) archwire engaged, Carriere Class III Motion Appliance bonded in mandibular arch, and Class III elastic traction initiated.
Class III elastics (6oz, 1/4") were worn full-time, except during meals, from the mesial hooks on the appliance to the second molars. Another 10 weeks later, an upper .017" × .025" Cu Nitanium (35ºC) archwire was engaged to complete leveling and alignment and start torque correction. After three and a half months of anteroposterior correction, a Class I platform was achieved in the posterior segment, completing stage one (Fig. 4).
Brackets and molar tubes were then bonded in the mandibular arch, with a round .014" Cu Nitanium (27ºC) wire used for leveling and alignment. To tie the posterior teeth together as a unit on each side, a figure-8 .012" stainless steel ligature wire was run under the archwire from the first molar to the canine. Six weeks later, an upper .019" x .025" Cu Nitanium (35ºC) archwire and a lower .014" x .025" Cu Nitanium (27ºC) archwire were engaged to complete leveling and start torque control (Fig. 5).
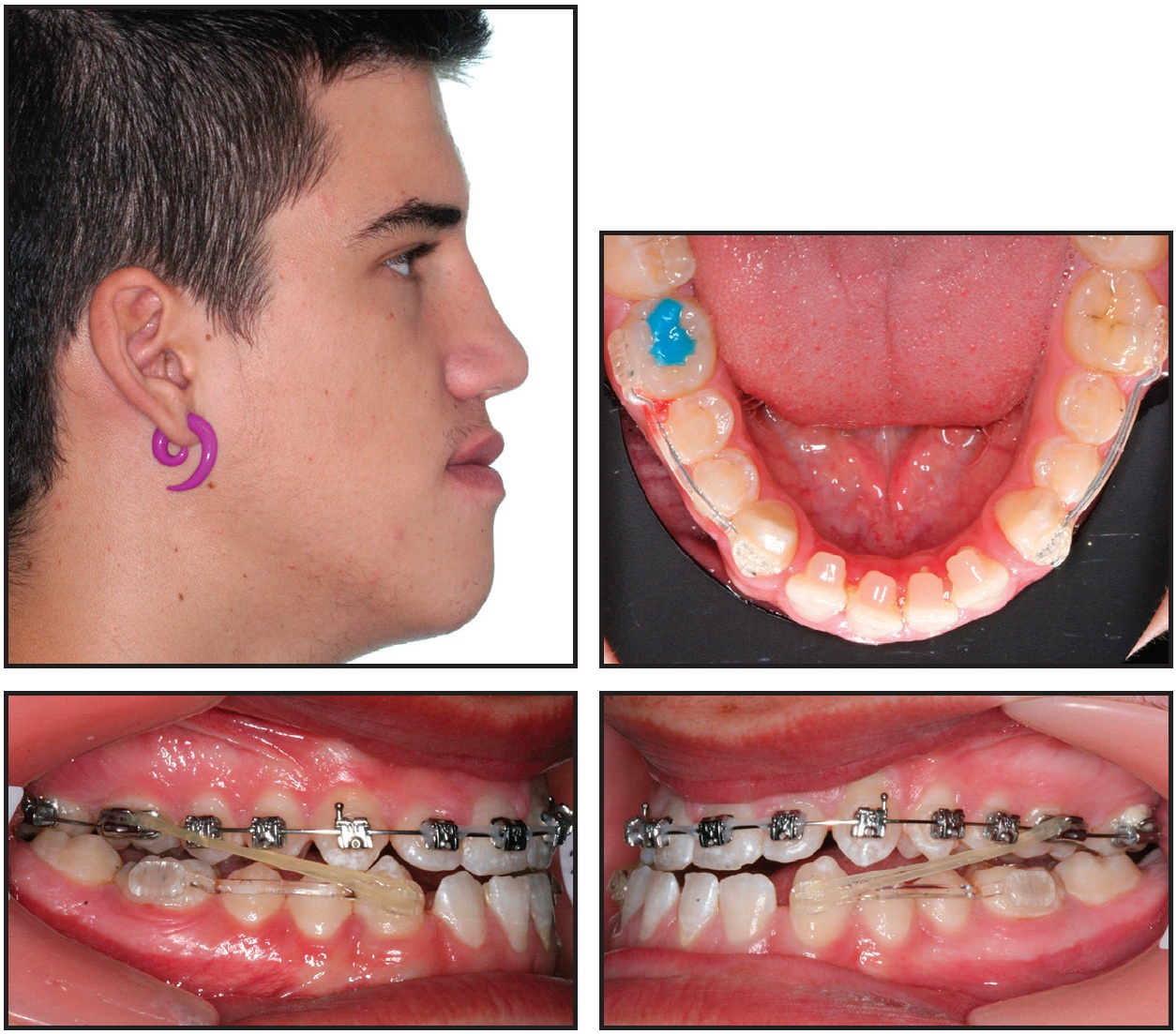
Fig. 4 Case 1. Class I platform achieved after three and a half months of Motion treatment.

Fig. 5 Case 1. Six weeks later, upper .019" × .025" Cu Nitanium (35°C) archwire and lower .014" × .025" Cu Nitanium (27°C) archwire placed to complete leveling and start torque control.
Light (2oz, 1/4") Class III elastics were worn at night only. To retract the lower incisors, elastic power chain was attached from the lower-second-premolar hooks to posts crimped on the mandibular archwire distal to each lateral incisor.
After eight and a half months of treatment, an upper .019" x .025" CNA** archwire was engaged for final torque adjustment, arch expansion, and detailing, and a TransForce2** palatal expander was placed to correct the buccal crossbite (Fig. 6).

Fig. 6 Case 1. After eight and a half months of treatment, upper .019" × .025" CNA** archwire and Trans-Force2** palatal expander placed, along with lower .017" × .025" Cu Nitanium (35°C) archwire.
An .017" x .025" Cu Nitanium (35ºC) wire was engaged in the mandibular arch, where the elastic power chain was maintained.
The TransForce2 appliance was in place for two and a half months of transverse development (Fig. 7).

Fig. 7 Case 1. After two and a half months of transverse development, TransForce2 expander debonded.
Triangular vertical elastics (2oz, 1/8") were prescribed for nighttime wear to settle the buccal occlusion, combined with oblique elastics (2oz, 1/4") worn from the lower right canine to the upper left canine for a final midline adjustment.
After 11 months of treatment, final settling and space closure were initiated by running power chain bilaterally from the second and first premolars to hooks crimped on the upper .019" × .025" CNA archwire and the lower .019" × .025" Cu Nitanium (35ºC) archwire (Fig. 8).

Fig. 8 Case 1. Final settling initiated with bilateral power chain from second and first premolars to crimpable hooks on upper .019" × .025" CNA archwire and lower .019" × .025" Cu Nitanium (35°C) archwire.
After a total 18 months of treatment, the fixed appliances were removed, a 3-3 lower lingual retainer was bonded, and a vacuum-formed aligner was delivered to retain the upper arch (Fig. 9A).
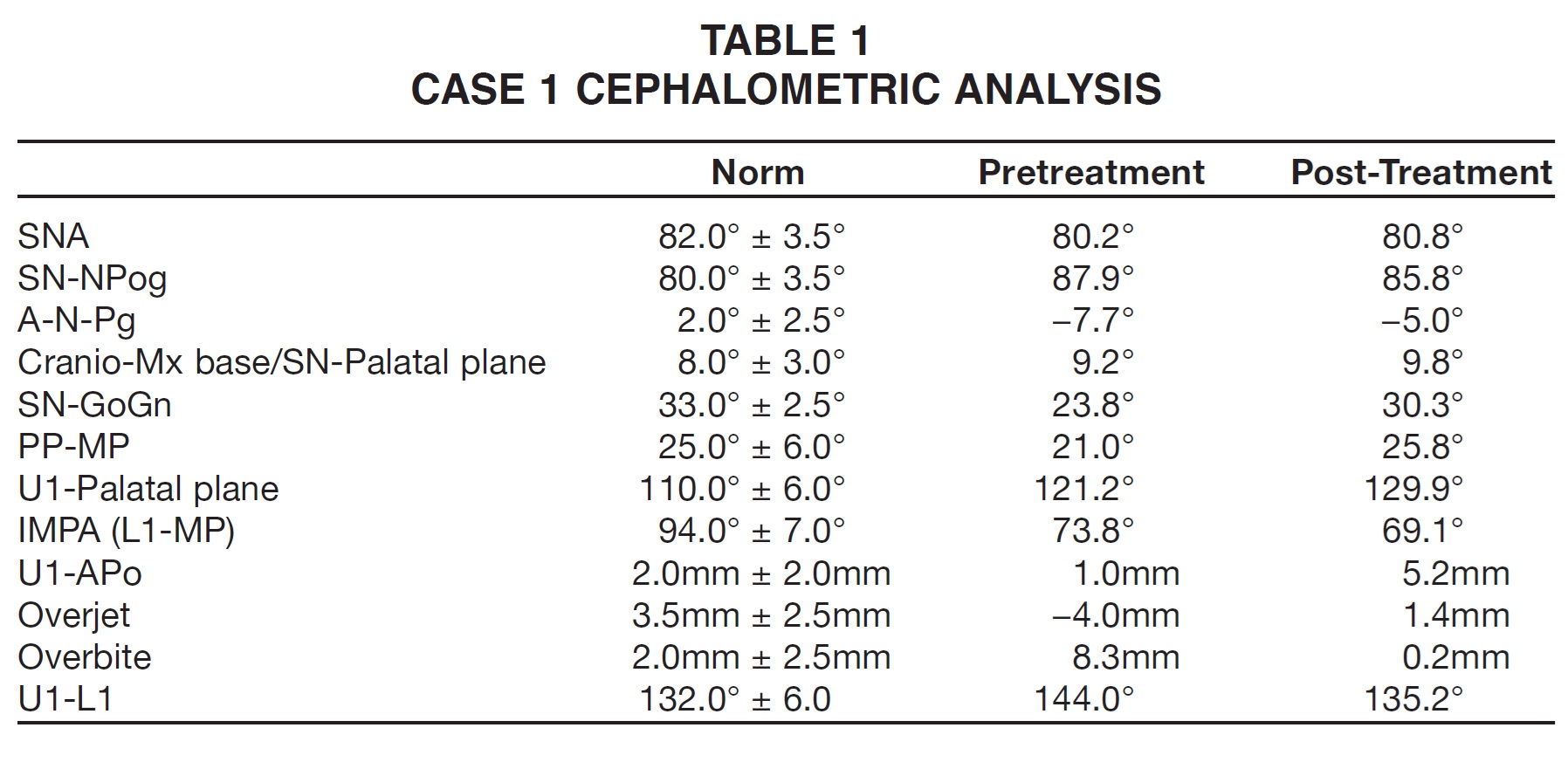
During treatment, as evidenced by a reduction in ANB, the mandible rotated clockwise, opening the maxillomandibular angle and reposturing the mandible in the temporomandibular space (Fig. 9B, Table 1).
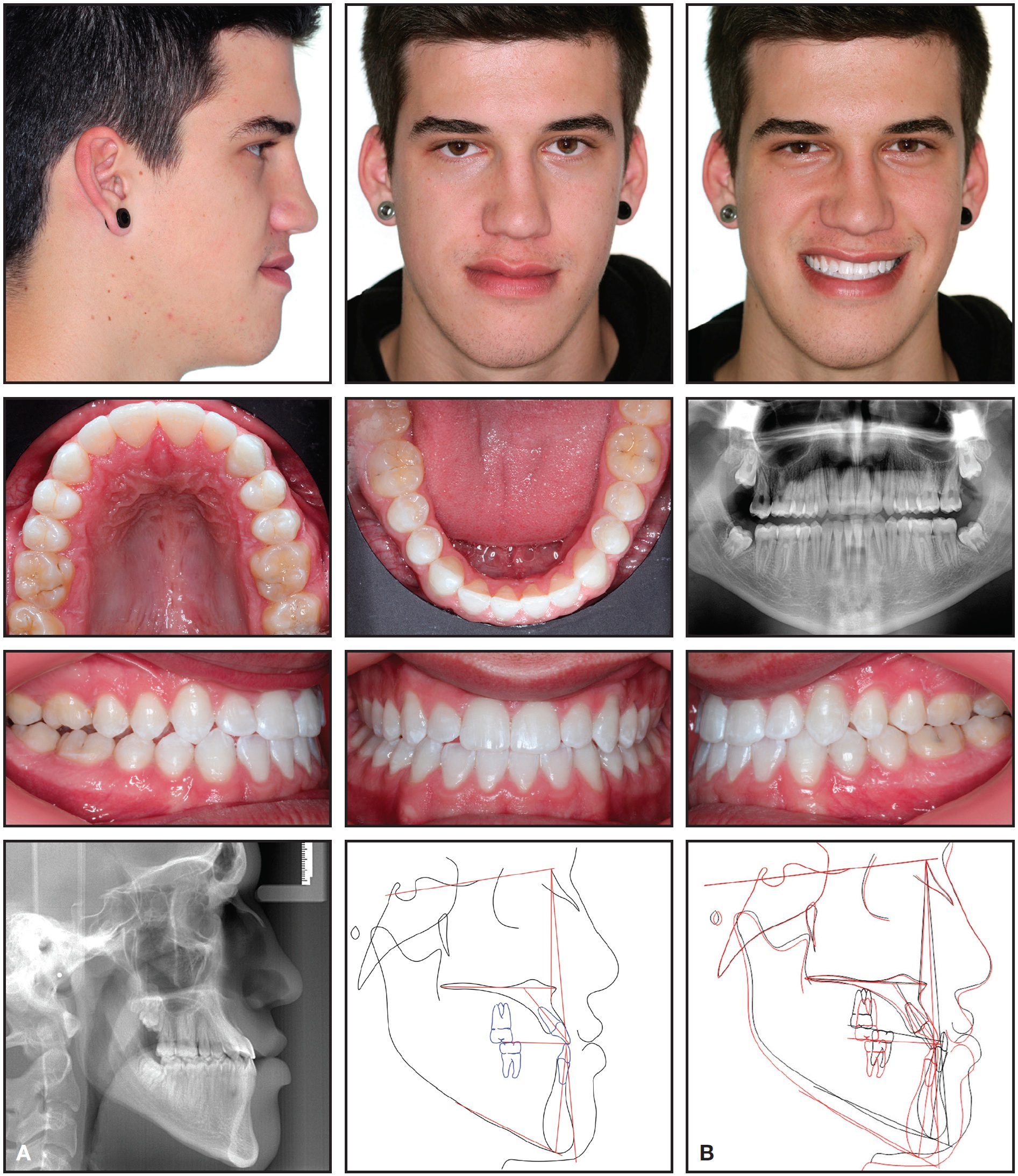
Fig. 9 Case 1. A. Patient after 18 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
The vertical dimension also increased. The upper molars were mesialized and extruded, and the upper incisors moderately protruded. The lower molars were intruded; each posterior segment was distalized as a unit from molar to canine, resulting in a Class I dental relationship. In addition, the lower incisors were retruded as the overjet and overbite were corrected. A counterclockwise rotation of the occlusal plane was noted, typical of the Carriere Class III Motion Appliance. Facially, the soft-tissue profile and smile line improved due to retrusion of the lower lip, better balance of the lower facial third, and protrusion of the upper lip to a more harmonious position. Retrusion of menton occurred as a consequence of the reposturing of the mandible and opening of the maxillomandibular angle.
Records taken 19 months after completion of active treatment confirmed the stability of the results (Fig. 10).
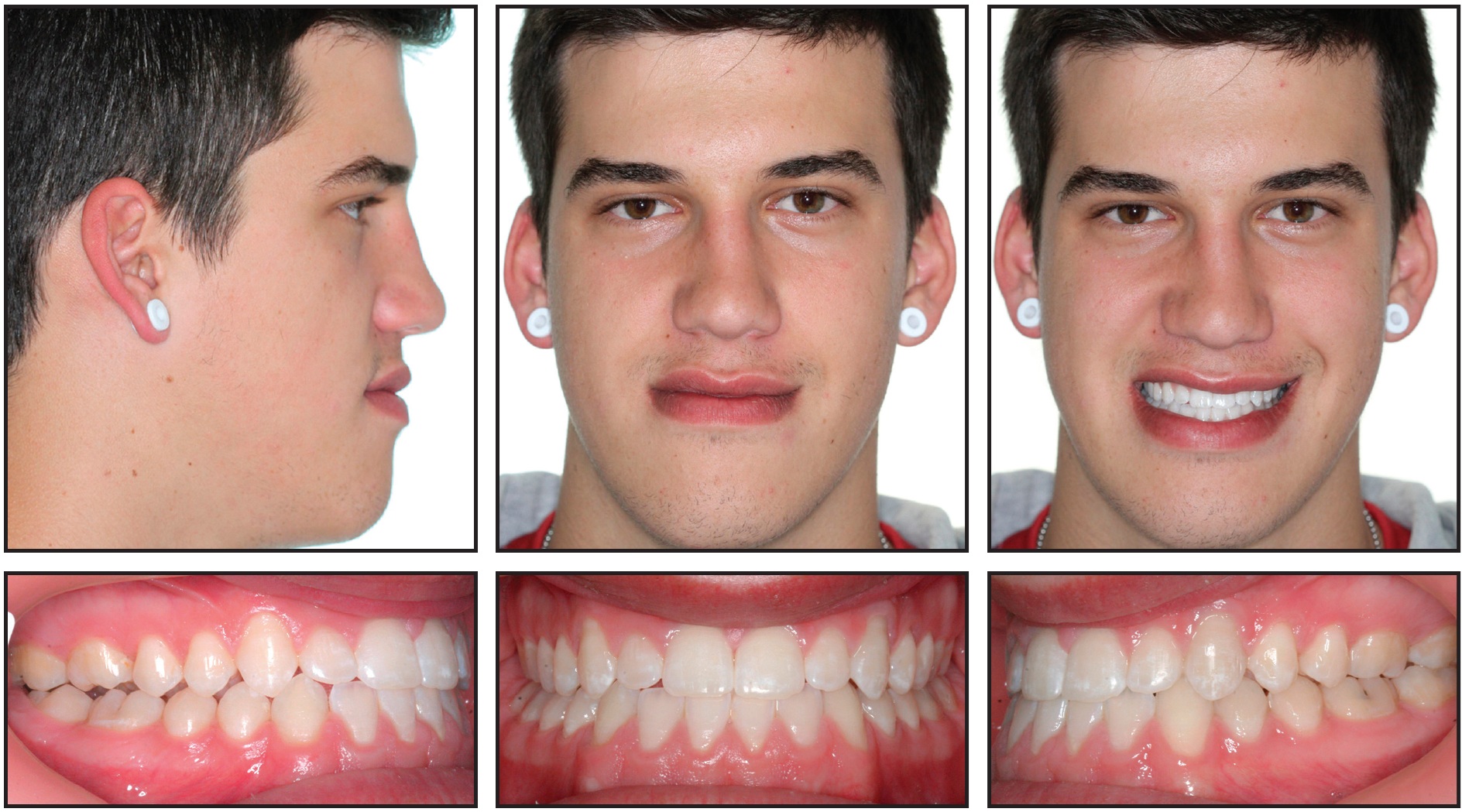
Fig. 10 Case 1. Patient 19 months after completion of active treatment.
Case 2
A 31-year-old female presented with the desire to correct her reverse overjet and the esthetics of her smile (Fig. 11). Her chief complaint was the functional incongruence between her dental arches, especially when chewing.

Fig. 11 Case 2. 31-year-old female patient with severe skeletal and dental Class III malocclusion and unilateral crossbite before treatment.
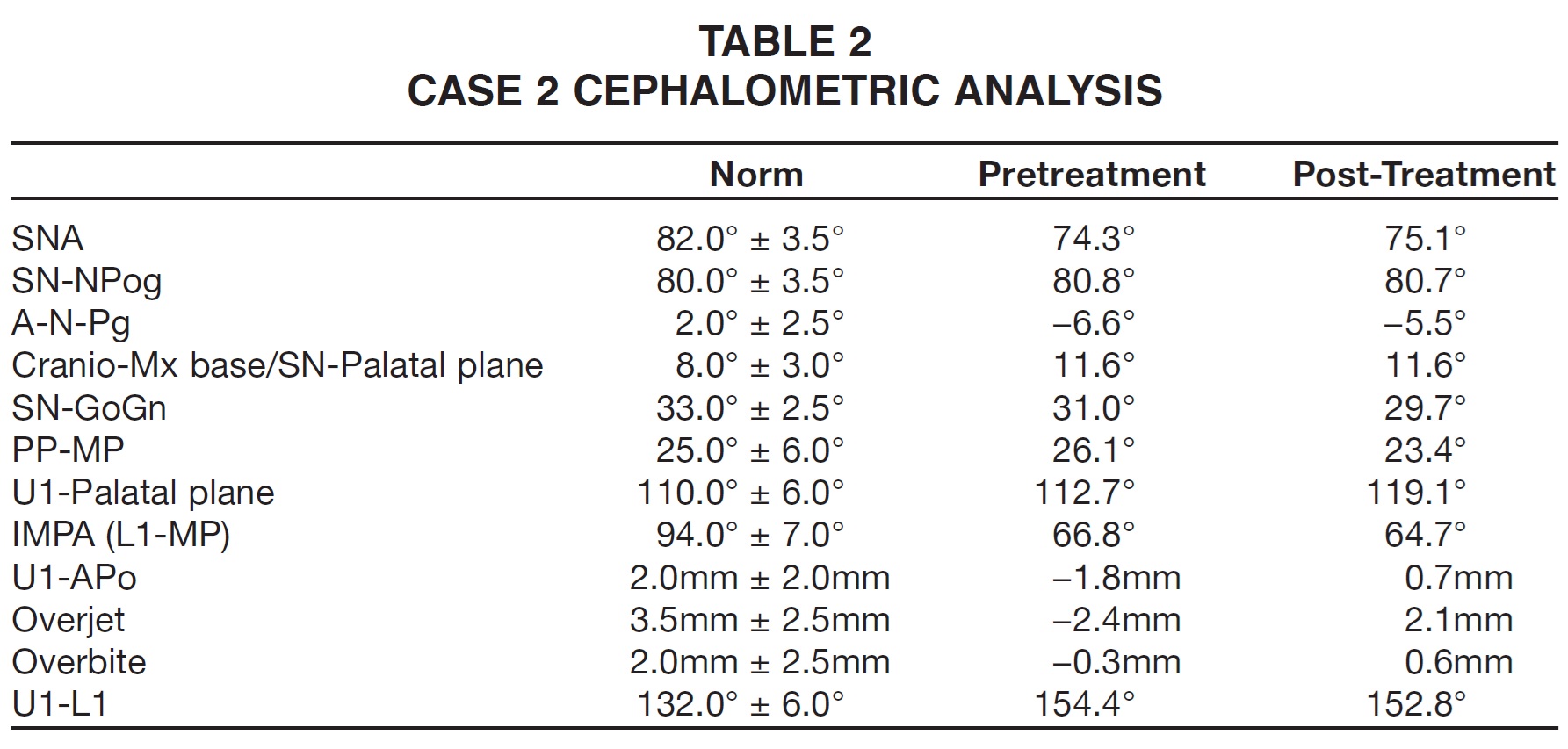
The patient displayed a full-step Class III relationship of the molars and canines, anterior and posterior crossbites on the right side, a 2.4mm negative overjet, a .3mm negative overbite, an open-bite tendency from canine to canine, and a slight shift of the lower midline to the right (Table 2). Her skeletal anomalies included a divergent facial type and a skeletal Class III with bilateral maxillary constriction.
The prominence of the patient's lower lip in relation to the upper lip increased the prognathic aspect of her face in profile. Although she was conscious of her facial appearance, she was not concerned about the mandibular prognathism, which was an accepted trait in her family. She did, however, want to diminish the concavity of her midface. Functionally, she exhibited macroglossia, with the tongue interposed between the dental arches at rest; perioral hypertonicity, with a thin, slightly short upper lip; and an obtuse nasolabial angle. Her periodontal condition was healthy, but she showed severe gingival recession and a thin periodontium due to vigorous, improper tooth-brushing.
The maxillary arch was bonded with Carriere SLX .022" passive self-ligating brackets and .022" edgewise molar tubes. The brackets were copolymer prototypes selected by the patient. Leveling and alignment were initiated on a round .014" Cu Nitanium (27ºC) archwire.
Six weeks later, an upper .014" × .025" Cu Nitanium (27ºC) archwire was engaged, and a Carriere Class III Motion Appliance was bonded in the mandibular arch (Fig. 12).

Fig. 12 Case 2. After six weeks of initial leveling and alignment, upper .014" × .025" Cu Nitanium (27°C) archwire engaged, Carriere Class III Motion Appliance bonded in mandibular arch, and Class III elastic traction initiated.
Class III elastics (6oz, 1/4") were worn full-time, except during meals. Ten weeks later, an upper .017" × .025" Cu Nitanium (35ºC) archwire was placed to complete leveling and alignment and start torque correction (Fig. 13).

Fig. 13 Case 2. After four months of treatment, upper .017" × .025" Cu Nitanium (35°C) archwire placed.
After five months of anteroposterior correction, a Class I platform was achieved in the posterior segment, completing stage one (Fig. 14).
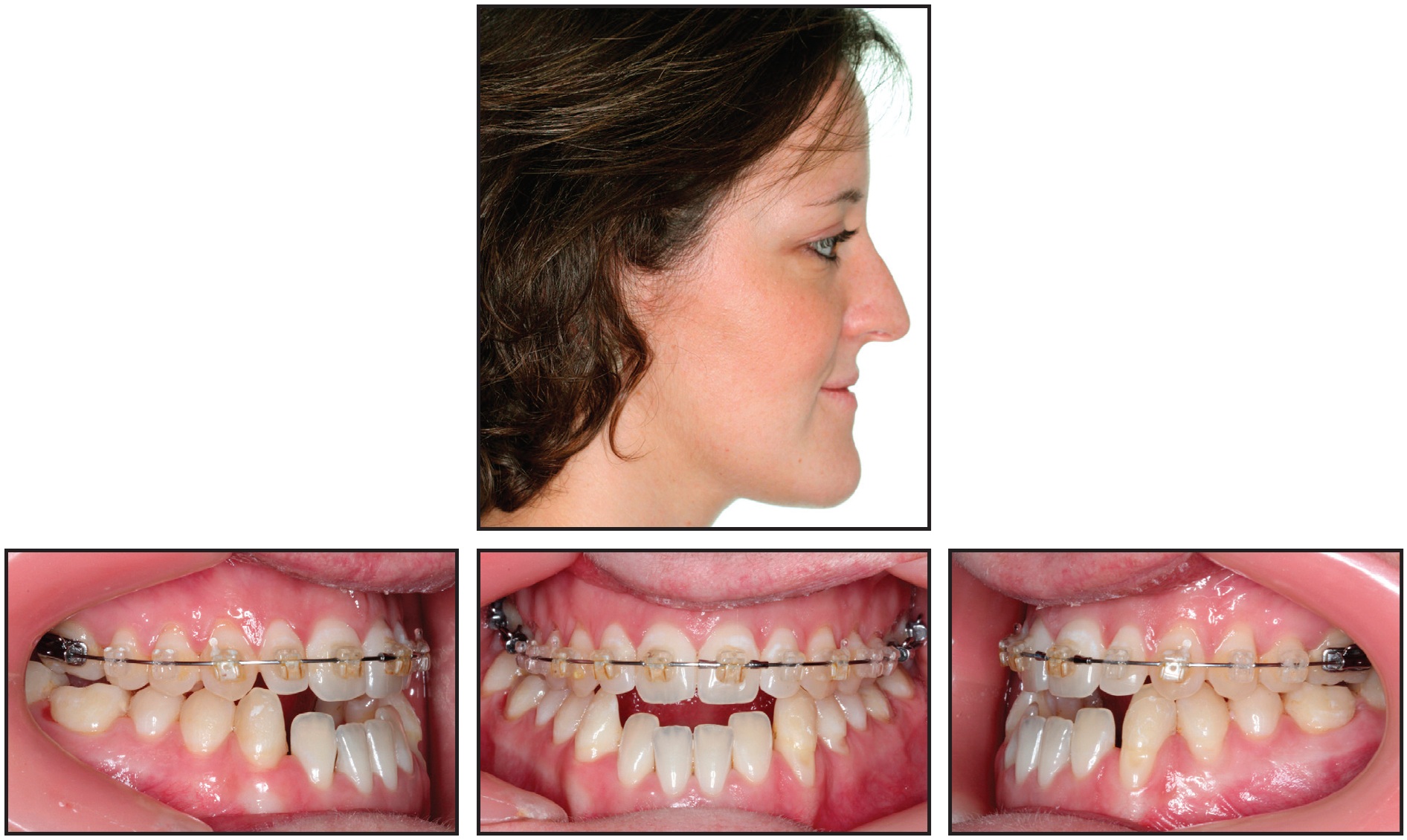
Fig. 14 Case 2. Class I platform achieved after five months of Motion treatment.
Brackets and molar tubes were then bonded in the mandibular arch, and a round .014" Cu Nitanium (27ºC) wire was engaged for leveling and alignment (Fig. 15).

Fig. 15 Brackets and molar tubes bonded in mandibular arch, with round .014" Cu Nitanium (27°C) wire engaged for leveling and alignment.
Six weeks later, a lower .014" x .025" Cu Nitanium (27ºC) archwire was placed to complete leveling and alignment and start torque control. Light (2oz, 1/4") Class III elastics were worn at night only.
After 10 months of treatment, an upper .019" x .025" Cu Nitanium (35ºC) archwire and a lower .017" x .025" Cu Nitanium (35ºC) archwire were engaged, and retraction of the lower incisors was initiated with elastic chain from the second premolars to posts crimped on the mandibular archwire distal to the lower lateral incisors (Fig. 16).

Fig. 16 Case 2. After 10 months of treatment, upper .019" × .025" Cu Nitanium (35°C) archwire and lower .017" × .025" Cu Nitanium (35°C) archwire placed for retraction of lower incisors with elastic chain.
After 12 and a half months of treatment, an upper .019" x .025" CNA finishing wire and a lower .019" x .025" Cu Nitanium (35ºC) finishing wire were engaged for final torque adjustments, arch expansion, and detailing (Fig. 17).

Fig. 17 Case 2. After 12.5 months of treatment, upper .019" × .025" CNA finishing wire and lower .019" × .025" Cu Nitanium (35°C) finishing wire engaged for final torque adjustments, arch expansion, and detailing.
Triangular vertical elastics (2oz, 1/8") were prescribed for nighttime wear to settle the buccal occlusion, combined with oblique elastics (2oz, 1/4") worn from the lower right canine to the upper left canine for a final midline adjustment.
After a total 18 months of treatment, the fixed appliances were removed, and a 3-3 upper lingual retainer was bonded (Fig. 18A). For a final esthetic touch, minor labial recontouring was performed in the upper arch by injecting a hyaluronic acid dermal filler at the lip border.
Cephalometric superimpositions indicated a slight distal reposturing of the mandible at the level of the temporomandibular space, as shown by a slight reduction in ANB (Fig. 18B, Table 2). The upper molars were extruded and also migrated mesially, resulting in a Class I dental occlusion. The upper incisors were protruded, and the open bite was closed. The final profile reflected a retrusion of the lower lip and protrusion of the upper lip. As in Case 1, the occlusal plane suffered a counterclockwise rotation.
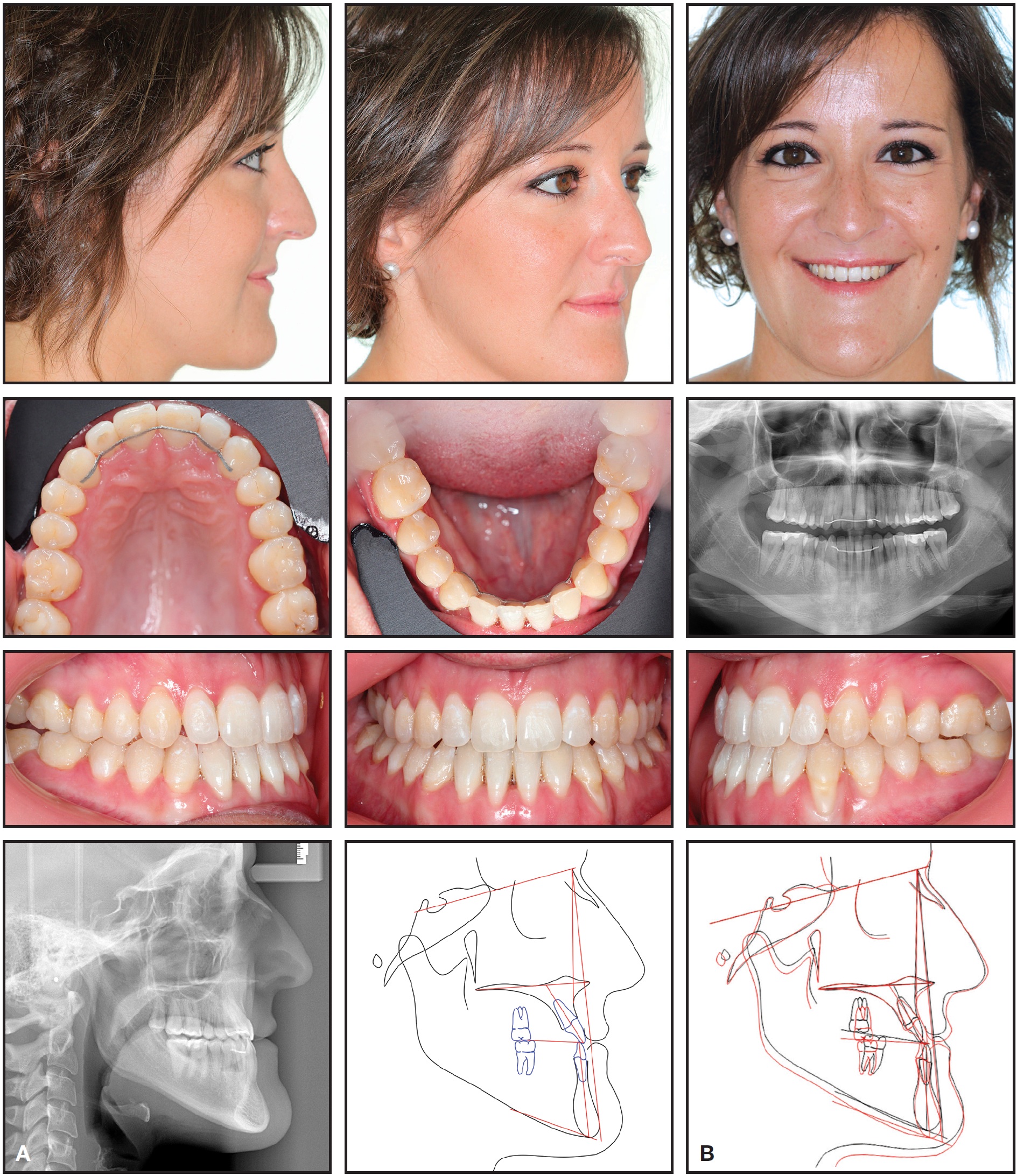
Fig. 18 Case 2. A. Patient after 18 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Discussion
Distalization is not the only effect of the Carriere Class III Motion Appliance, which is why it is not referred to as a distalizer. Clinical experience with the device has demonstrated skeletal and dental changes, alterations of the occlusal plane and the intermaxillary relationship, and improvement of soft-tissue prognathic conditions.
Skeletally, the appliance fosters a functional repositioning of the condyle in the temporomandibular complex. As a consequence of lower-molar intrusion and lower-canine extrusion, the mandible repostures along the occlusal plane. This phenomenon has consistently resulted in a counterclockwise rotation of the posterior occlusal plane - a direct effect of the appliance. Combined with distalization of the posterior mandibular dental segments, retraction of the lower incisors, and a slight advancement of the upper incisors, it produces a marked improvement in a prognathic profile.
The retropositioning of the mandible and counterclockwise rotation of the mandibular plane result in a shortening of the musculature involved in the floor of the mouth, including the genioglossus, geniohyoid, mylohyoid, and digastric muscles. As these muscles become more relaxed, they create a larger space for the base of the tongue in the posterior third of the pharyngeal cavity, which is a naturally comfortable and more functional zone. The anterior pressure of the tip of the tongue against the lower incisors is thereby reduced, resulting in an improvement of the facial profile.
In treating Class III patients, our understanding has grown of the importance of facial features and the facial icon to a person's identity, as well as the potentially detrimental effects of orthognathic surgical transformation on the emotional, affective, and psychosocial aspects of certain patients. The purpose of the Carriere Class III Motion Appliance is to improve the face by correcting the extrinsic traits that patients most commonly object to, while respecting the intrinsic traits that are considered part of the patient's identity. When the appliance is offered as an orthodontic alternative to a patient who is unwilling to undergo surgery, the traits that differentiate the morphology of human faces - both intrinsic and extrinsic - and how they are affected by each treatment method should be explained to the patient during an in-depth interview. These considerations might not apply to some pathological cases.
Conclusion
Class III treatment requires decisions to be based not only on the morphological traits that present as orthodontic problems, but also on those that warrant consideration for their possible psychological and quality-of-life impact. Taking the latter into consideration when making treatment recommendations is a specialized service rendered by the orthodontist. Each individual should be treated based on his or her own personal expectations, combined with the orthodontist's professional advice and human understanding.
FOOTNOTES
- *Trademark of Henry Schein Orthodontics, Melville, NY; www.henryscheinortho.com.
- **Registered trademark of Henry Schein Orthodontics, Melville, NY; www.henryscheinortho.com.
REFERENCES
- 1. Proffit, W.R. and Ackerman, J.L.: A systematic approach to orthodontic diagnosis and treatment planning, in Current Orthodontic Concepts and Techniques, 3rd ed., ed. T.M. Graber and B.F. Swain, C.V. Mosby, St. Louis, 1985.
- 2. anson, G.; de Souza, J.E.; Alves, F.A.; Andrade, P. Jr.; Nakamura, A.; de Freitas, M.R.; and Henriques, J.F.: Extreme dentoalveolar compensation in the treatment of Class III malocclusions, Am. J. Orthod. 128:787-794, 2005
- 3. Moullas, A.T.; Palomo, J.M.; Gass, J.R.; Amberman, B.D.; White, J.; and Gustovich, D.: Nonsurgical treatment of a patient with a Class III malocclusion, Am. J. Orthod. 129:S111-S118, 2006.
- 4. Carrière, J.: Inverse Anchorage Technique in Fixed Orthodontic Treatment, Quintessence Publishing Co., Inc., Chicago, 1991.
- 5. Liu, X. and Yang, Z.: Orthodontic camouflage treatment of an adult skeletal Class III malocclusion, J. Clin. Orthod. 44:57- 63, 2010.
- 6. Locatelli, R.; Bednar, J.; Dietz, V.S.; and Gianelly, A.A.: Molar distalization with superelastic NiTi wires, J. Clin. Orthod. 26:277-279, 1992.
- 7. Miura, F.; Mogi, M.; Ohura, Y.; and Hamanaka, H.: The super-elastic property of the Japanese NiTi alloy wire for use in orthodontics, Am. J. Orthod. 90:1-10, 1986.
- 8. Cetlin, N.M. and Ten Hoeve, A.: Nonextraction treatment, J. Clin. Orthod. 17:396-413, 1983.
- 9. Bartzela, T. and Jonas, I.: Long-term stability of unilateral posterior crossbite correction, Angle Orthod. 77:237-243, 2007.
- 10. Haas, A.J.: Palatal expansion: Just the beginning of dentofacial orthopaedics, Am. J. Orthod. 57:219-255, 1970.
- 11. Garner, L.D.: Soft-tissue changes concurrent with orthodontic tooth movement, Am. J. Orthod. 66:367-377, 1974.
- 12. De Bono, E.: Simplicity, Penguin Putnam, Inc., New York, 1999.
- 13. Benius, J.M.: Biomimicry: Innovation Inspired by Nature, HarperCollins Publishers, Inc., New York, 2002.
- 14. Cussó Anglés, J.: Gaudi's Sagrada Familia: A Monument to Nature, Editorial Milenio, Lleida, Spain, 2013.
- 15. Carrière, L.: Hippocratic philosophy: Biominimalism and new technologies: Innovation in a new orthodontic treatment method and optimization of the facial icon, lecture, Induction Ceremony of Access as Numerary Member of Royal Academy of Doctors, Barcelona, 2015.
- 16. Carrière, L.: A new Class II distalizer, J. Clin. Orthod. 38:224-231, 2004.
- 17. Carrière, L.: Orthodontic positioning system with Carriere SLB and Carriere distalizer: A road map for the orthodontic trip, syllabus, 2006.
-
 DR. CARRIERE
DR. CARRIERE
Dr. Carrière is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at Clinica Carrière, Escoles Pies, 109, 08017 Barcelona, Spain; e-mail: luis@carriere.es. He the inventor of and has a financial interest in the Carriere Class II Motion Appliance, Class III Motion Appliance, and SLX Passive Self-Ligating Bracket.