(Editor’s Note: In this regular column, JCO provides an overview of a clinical topic of interest to orthodontists. Contributions and suggestions for future subjects are welcome.)
Can upper molars really be distalized? This elusive query comes up whenever the topic of Class II correction is raised, yet no conclusion seemingly achieves a consensus. At least, we periodically pretend not to comprehend how correction occurs (despite the substantial number of clinical and research reports on the subject) so as to promote methods that may be in current favor.
The idea that the maxilla or the maxillary dentition can be moved posteriorly to resolve a Class II malocclusion is perhaps one of the oldest and least understood concepts in orthodontics. The application of some type of pushing force against the upper arch and teeth to correct a Class II has obviously worked well enough during the past 100 years of orthodontics to perpetuate the "orthopedic" side of the specialty. The term distalization is a neologism, made up in recent years for our convenience. But while it may be an example of "bad" English, it might still be good orthodontic practice. To address whether upper molars can really be distalized, we need to address how contemporary distalization methods do what they do.
Similar articles from the archive:
Headgears and so-called Baker anchorage (Class II intermaxillary elastics) are highly successful methods of Class II correction that have stood the test of time, and whose effects have been rigorously evaluated.1 Interestingly, it has been variously claimed that neither or both can produce molar distalization.2 Fixed and removable functional appliances3 and intramaxillary appliances featuring finger4 or helical springs,5 jackscrews,6 or coil springs7-9 have all found a place in the armamentarium of so-called "distalizers". Adjuncts to full fixed orthodontic appliances, including the bulbous loops of the Tweed technique, repelling magnets,10,11 compressed superelastic wires,12 and jigs dependent on intermaxillary elastics13 or coil springs14,15 have also garnered a modicum of interest. These methods and gadgets have all produced demonstrable distal molar movement.
What Are Our Intentions?
When asked the purpose of molar distalization, we often stumble over the means rather than focus on the ends. It must be understood that the intent of molar distalization is the same as that of any other method of Class II correction: fix the malocclusion. Pushing molars posteriorly is simply a technique devised to deal with the teeth that are most problematic to move. The ability to reduce our reliance on patient cooperation - as required by such adjuncts as elastics, headgear, and functional appliances - is the primary reason for the increasing popularity of molar distalizers.
All six upper molars have been pushed posteriorly using any of the previously mentioned methods, with varying degrees of success. The following questions and answers about how distalization works, what effects it produces, what problems it creates, and how it compares to other methods of Class II correction are intended to provide an evidence base for the technique and, consequently, improve our quality of patient care.
Are We Just Tipping Molars?
Early detractors of molar distalization with headgear or elastics claimed that pushing molars only served to tip them backward, even though Class II malocclusions were being corrected by these methods.16 Cephalometric analyses of such cases frequently indicated minimal distal movement of the molars. Studies of appliances designed specifically to push molars distally (for example, the Jones Jig*, the Pendulum**, the Greenfield molar distalizer,17 and sagittal appliances18) did demonstrate more distal molar movement, but also found dramatically increased molar tipping.3,14,19-32
Unfortunately, most distalization methods apply force at the crown level, occlusal to the center of resistance of the molar, resulting in molar tipping. A reassessment of the point of force application led Carano and Testa to design the unique Distal Jet* appliance, which applies force through a mechanical couple closer to the center of resistance of the tooth, substantially reducing the degree of tipping8,33-37 (Fig. 1).
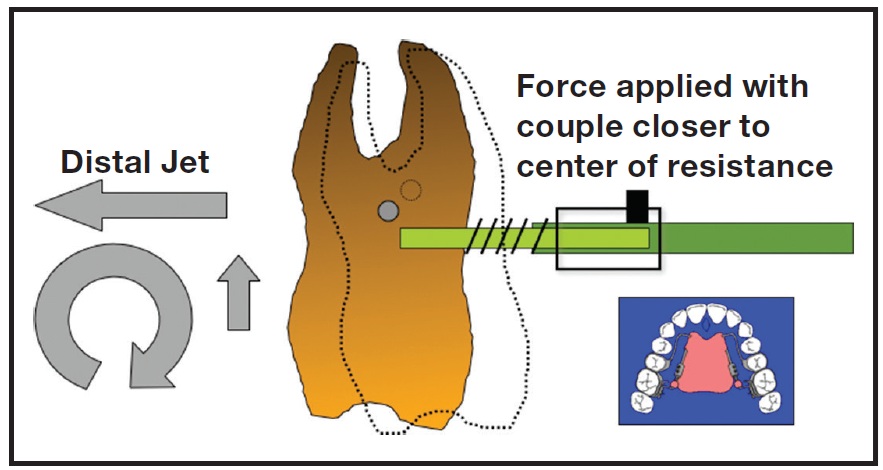
Fig. 1 Distal Jet* molar-distalization appliance produces less tipping of upper molars, since force is applied with couple closer to center of resistance. Device serves two purposes: uppermolar distalization without patient compliance and support for retraction of remaining maxillary dentition, once locked down to hold Class I molar positions.
Are We Simply Losing Anchorage?
Headgear uses the back of the head as "temporary skeletal anchorage", thereby preventing anchorage loss from mesial movement of the other maxillary teeth. If reciprocal forces are used to push the molars distally, however, the other end of that mechanism must dissipate its force in the opposite direction. For example, fixed-functional appliances and Class II elastics push the lower teeth forward, causing a loss of mandibular dental anchorage38-42 (although miniscrew anchorage can mitigate that loss43,44). In the maxilla, intramaxillary appliances are usually anchored by some combination of premolars, anterior teeth, a metal framework, and an acrylic Nance button in the anterior palate,45 all of which permit some degree of anchorage loss.16,29-33,46-52 In other words, when upper molars are moved posteriorly (when anchored on either the upper or lower teeth), those anchor teeth are likely to move anteriorly, honoring Newton's third law. Because anchorage is inevitably lost, the critical question becomes: Can we afford anchorage loss in a particular case? If not, an alternative method of Class II correction, such as extractions or surgery, may need to be considered, or better anchorage developed.
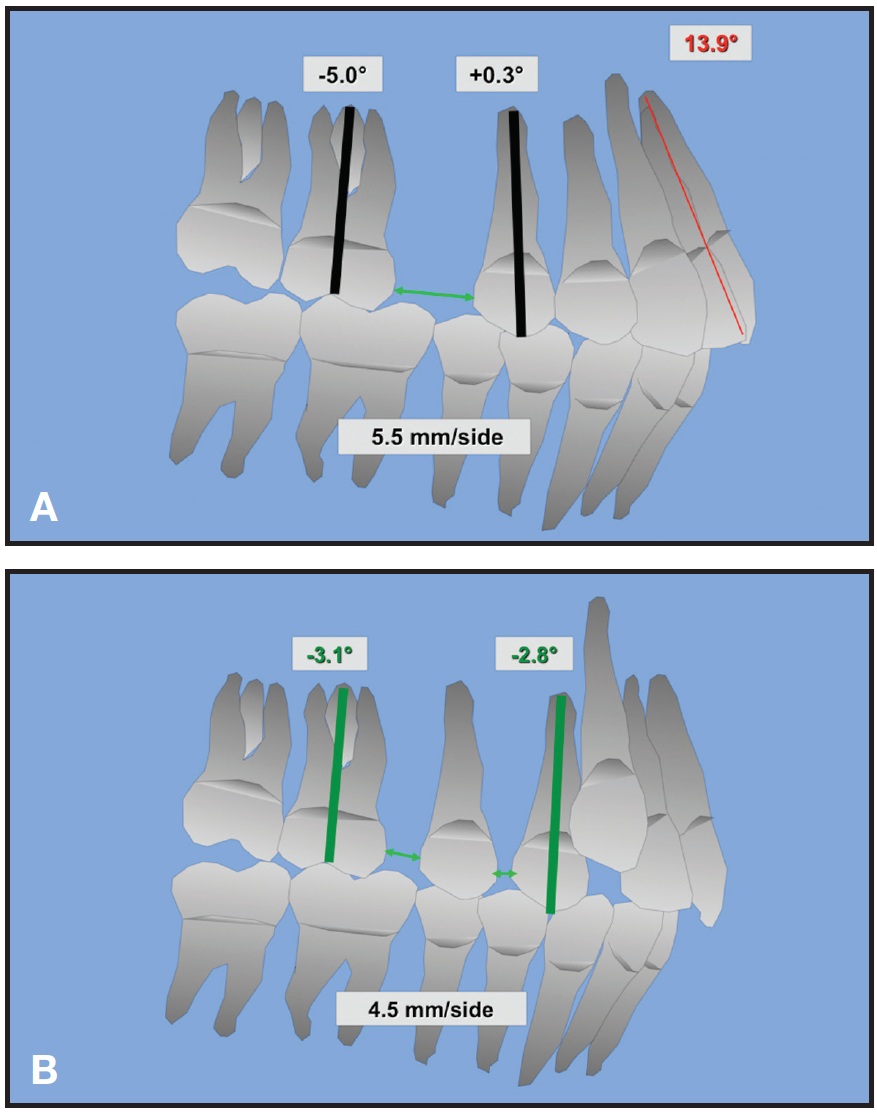
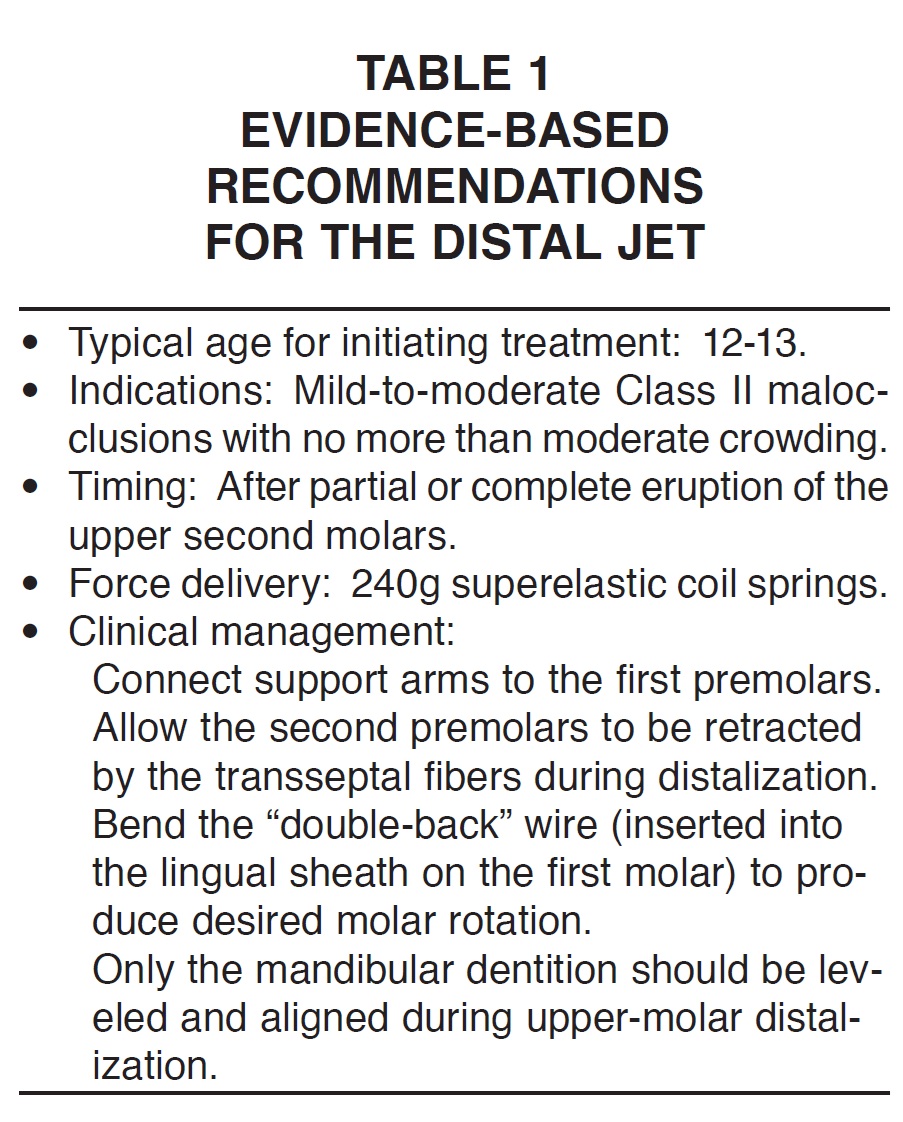
The brackets on all the maxillary teeth anterior to the molars can be tied together to create one large anchorage unit, but this approach has proven relatively unsuccessful in preventing anchorage loss.53-56 An upper preadjusted appliance will produce about 10º more labial flaring of the incisors than would occur if no brackets were placed (Fig. 2A).30,31,48 The effect is most readily apparent in a Class II, division 2 patient who suddenly develops unesthetic overjet during distalization. As Melsen and Bosch concluded, "There is little anchorage value to mobilized teeth."57 As a result, it has been suggested that molar distalization should be accomplished before bonding maxillary brackets (Fig. 2B).33,36 After all, what could be a more esthetic and hygienic appliance, during the first five to 10 months of Class II treatment, than no appliance? Meanwhile, the lower arch can be bracketed, leveled, and aligned up to rectangular "working" wires, often in time to support any intermaxillary elastics or fixed-functional appliances that may be needed36 (Table 1).
Is Space Opening Always Undesirable?
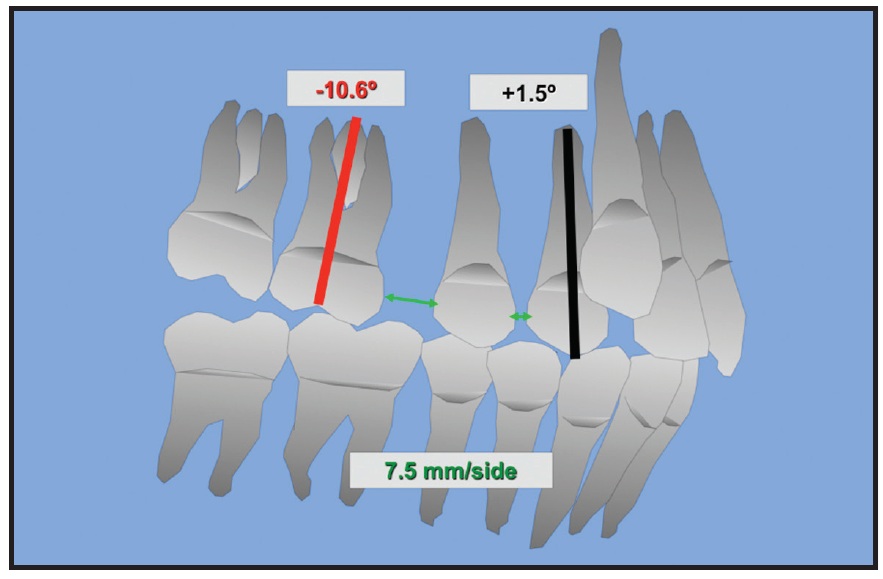
If reciprocal forces are used for molar distalization, interdental spaces are typically opened in the maxillary arch - either by the molars moving back or by other teeth moving forward, depending on which teeth have been used for support of the appliance33,36 (Fig. 3). These spaces are often substantial and can be disconcerting to the patient and general dentist.24 Still, there are instances in which spaces in the upper arch may be beneficial in creating arch length for blocked-out canines. Careful diagnosis is required, and the extraction of upper premolars should not be dismissed as a viable alternative.
Are We Propping Open the Bite?
Some critics have opined that molar distalization simply props open the bite, dislodging the condyles and potentially leading to TMD.58 It is true that if significant extrusion of the upper posterior teeth were produced during distalization, then the bite could be opened. If the molars are tipped back, then the mesial cusps and marginal ridges would be more likely to create some transient downward and backward (clockwise) rotation of the mandible. Reciprocal forces may extrude the molars and anchoring premolars, increasing lower anterior face height. Devices that produce more bodily movement, less molar tipping, and minimal extrusion (such as the Distal Jet) are unlikely to cause these issues.33,59
Must We Expand?
McNamara and Brudon60 and Hilgers5 have stated that maxillary expansion is a prerequisite to Class II correction. Certainly, the upper arch must be coordinated with the lower arch, and obvious transverse discrepancies have to be addressed, but is the use of a jackscrew expander a necessity?
The Pendulum appliance required the addition of a jackscrew due to the geometry of distolingual forces produced by its sweep springs. If there were no active transverse expansion, the molars would be swept into crossbite. In contrast, when distalizing forces are simply applied along the diverging maxillary alveolar trough, they are, in effect, expansive in nature. For example, the Distal Jet produces 3-5mm of intermolar expansion when the appliance is designed to apply forces parallel to the archform.33,36 Although it would be unreasonable to expect this device to resolve a substantial transverse discrepancy, the appliance can be further expanded during fabrication, or a jackscrew can be added if necessary.36
Why Not Rotate Molars?
Distal molar rotation61 in a case of mild Class II malocclusion (the so-called pseudo-Class I62) is certainly a simple and successful treatment method. Devices designed for this purpose - including Korn lip bumpers,63 the Jones Jig,7 and the Carriere*** appliance13 - rotate the upper molars posteriorly around their palatal cusps to seat the mesiobuccal cusps in the buccal grooves of the lower molars, thus producing Class I relationships.
Unfortunately, some of the popular distalizers may actually rotate the molars in the wrong direction. The Distal Jet, for example, applies forces against the lingual surfaces of the upper molars that will rotate the teeth mesially, requiring substantially more distalization to achieve the same result.33,46,64 The "double-back" portion of the bayonet wire inserted into the lingual first-molar sheath can easily be adjusted to produce appropriate distal molar rotation, simply by "toeing in" the wire with a utility plier prior to delivery of the appliance.35,36,65 The sweep springs of the Pendulum appliance may accentuate appropriate molar rotation, but because this family of devices is not self-limiting, the forces will continue unabated if the patient does not return as appointed.
What About the Second and Third Molars?
It has been posited that second or third molars must be extracted to permit any true distalization, but there appears to be no support from the literature for this hypothesis. If upper second and third molars are present when first-molar distalization is initiated, they will also be moved distally, despite the substantial combined surface area of the three molar roots. Such movement may also entail anchorage loss or tipping, as previously described.
Enucleation or early removal of the upper third molars in an adolescent patient in hopes of facilitating molar distalization may be overly aggressive, considering the cost and potential morbidity. Removal of the upper second molars (if they have even erupted by the start of treatment) involves some modicum of wishful thinking that the third molars will consistently erupt in an appropriate and timely manner to serve as second-molar surrogates. Gianelly recommended that distalization be accomplished prior to the eruption of second molars.15 Should treatment be started early in a patient with unerupted second molars, hoping for the best, or should we wait for eruption to decide whether to have second molars extracted?
Maginnis reported that the "second molar eruption status showed no significant effects with relation to first molar distalization, tipping, or anchorage loss for patients treated with the Distal Jet".49 Flores-Mir and colleagues reached a similar conclusion: that the effect of upper second and third molar eruption on molar distalization appears to be minimal.66 Bolla and colleagues found half as much first-molar tipping (2º), less anchorage loss (.8mm), less premolar extrusion (1.2mm), and the same amount of distalization when the second molars had erupted as when they had not erupted.33 It seems that the crown of the first molar tends to tip posteriorly as the roots are "tripped" by the erupting second molar crown and the first molar's center of resistance moves superiorly.36
Until the efficacy of second- or third-molar extraction is clearly demonstrated, perhaps we should consider waiting to begin molar distalization until the late mixed to early permanent dentition, when the second molars are erupting.33,49 At this stage, there is less potential for iatrogenic buccoversion of the second molars, and the mandibular growth response will be more favorable. In addition, the erupted premolars may drift distally along with the molars, due to the pull of the transseptal fibers36 (Fig. 4).
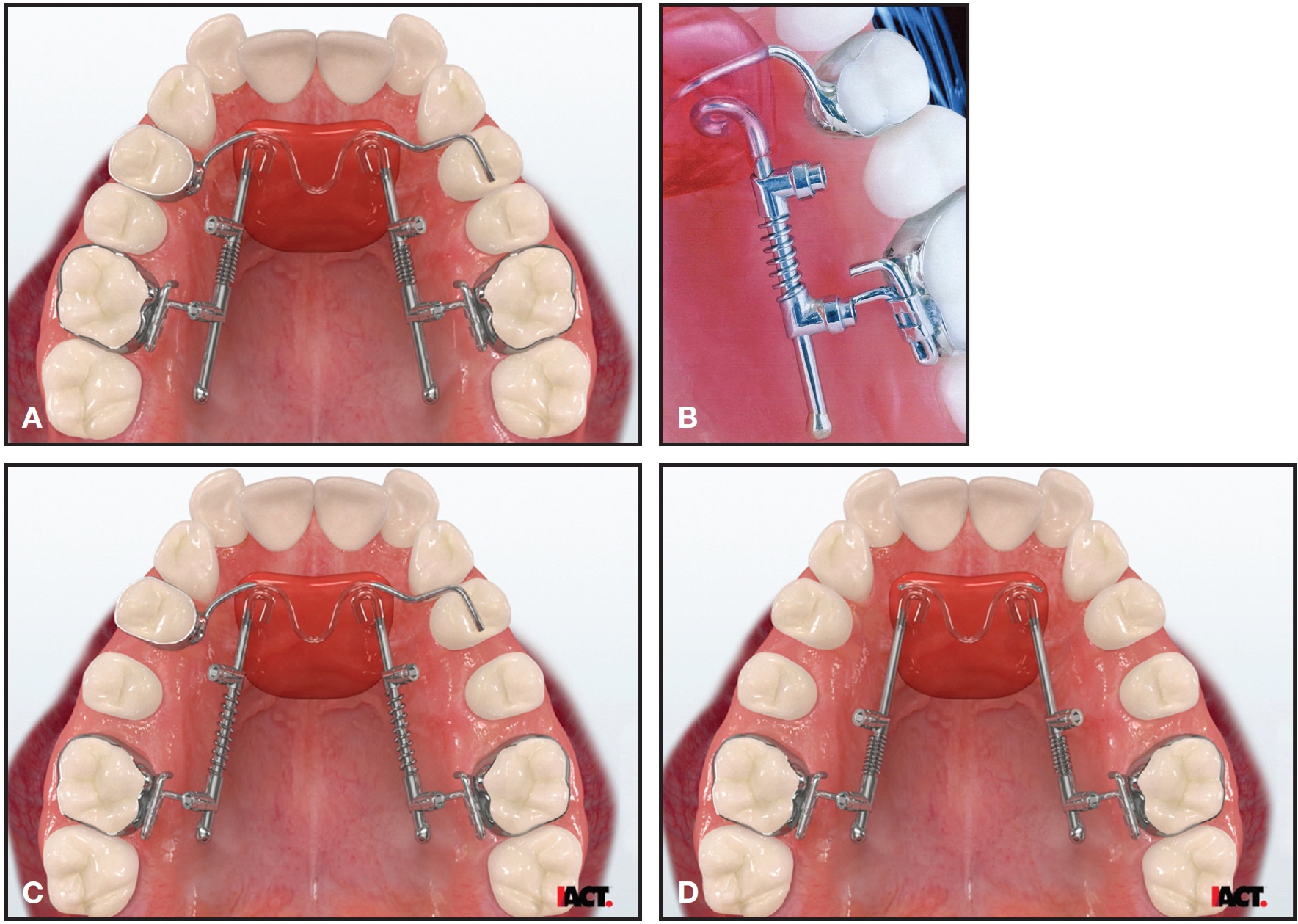
Fig. 4 Bowman modification of Distal Jet. A. Tube-and-piston construction replaced by simple tracking wires for better geometry and rigidity. Bands or bonded occlusal rests and Nance acrylic button provide anchorage. B. Mesial locks slid distally to compress 240g coil springs. Distalization is initiated by unlocking distal set screws only one-quarter turn; appliance is activated every four to six weeks for four to 10 months. C. Distal set screws locked down at completion of distalization. Premolars have followed molars as transseptal fibers stretched. D. Simple transition to modified Nance holding arch occurs when premolar support arms are sectioned at acrylic button (photos courtesy of IACT, Birmingham, AL).
These principles are illustrated by the case of a 12-year-old female who presented with a moderate Class II malocclusion, deep overbite, and minor crowding (Fig. 5).

Fig. 5 12-year-old female with moderate Class II malocclusion, deep overbite, and minor crowding before treatment.
Treatment was initiated with a Distal Jet and a lower preadjusted Butterfly System* appliance. A super-Class I molar relationship was achieved in six months, while the lower arch was leveled to an .019" x .025" stainless steel archwire (Fig. 6A). The Distal Jet was then converted to a modified Nance holding arch, and upper brackets were placed. Two months later, retraction of the anterior teeth was initiated with support from Class II elastics and the Nance holding arch (Fig. 6B).
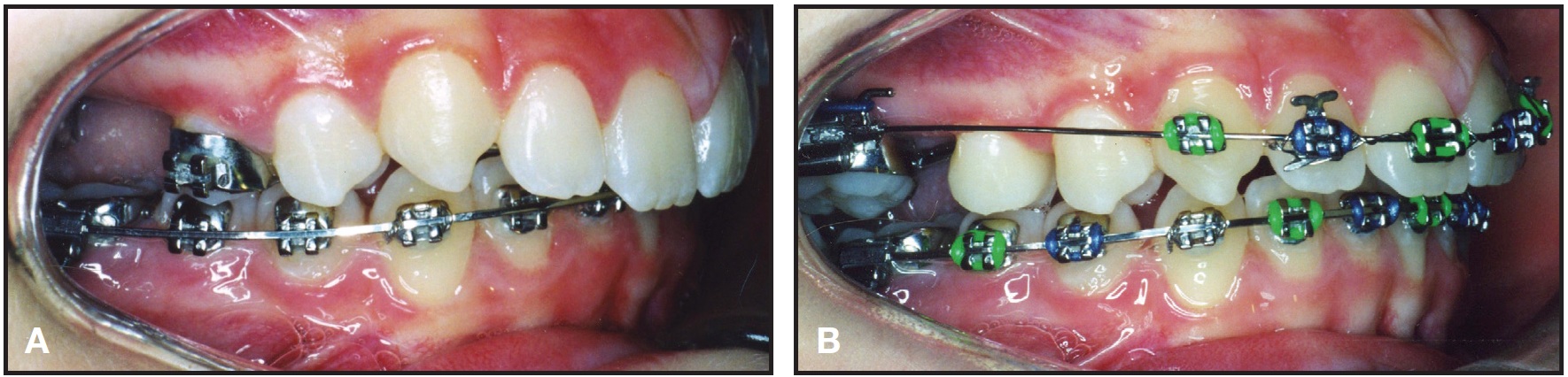
Fig. 6 A. Super-Class I molar relationship achieved after six months of distalization with Distal Jet; lower preadjusted Butterfly System* appliance used for leveling, up to .019" × .025" stainless steel archwire. B. Two months later, with Distal Jet converted into modified Nance holding arch, retraction of anterior teeth initiated using Class II elastics.
Total treatment time was 21 months (Fig. 7).

Fig. 7 Patient after 21 months of treatment.
Don't the Molars Just Move Forward Again?
It is quite disconcerting to superimpose pre- and post-treatment cephalometric tracings of a molar-distalization patient and find that both the upper and lower molars seem to have come forward substantially.46 Were the molars pushed back so carefully only to spring back forward? It may certainly appear that we had set out on a fool's errand - at least until we consider the effects of facial growth. Although the typical pattern of adolescent facial development includes slightly more mandibular than maxillary growth, both jaws are growing downward and forward. The jaws are also carrying teeth, which, in turn, are adjusting to maintain contact by erupting.36,59,67
In an untreated control group of Class II patients, the same growth pattern will be observed, but with the lower teeth "a step behind"(or the upper teeth a step ahead).68 Facial growth continues to carry both upper and lower molars downward and forward, but dentoalveolar compensation at the occlusal plane maintains the Class II relationship. When we interrupt the compensation mechanism with headgear, elastics, bite planes, expanders, functional appliances, or distalizers, the occlusal relationships change to Class I while the normal growth pattern continues on its course, carrying all the teeth (including the molars, now "locked" in Class I) mesially.69
What Happens After Distalization?
We can distalize molars into Class I relationships in five to 10 months, but the issue then becomes how to control subsequent tipping, rotation, extrusion, expansion, and reciprocal anchorage loss.30,33,49 As Watson astutely recognized, the key to Class II distalization is not how the molars are moved back, but what happens afterward in terms of biomechanics.70 In comparison, a functional appliance can "correct the Class II molar relationship instantaneously" on insertion, but it is what occurs later - dentoalveolar changes and growth - that actually achieves the correction.71
This is not the only similarity between distalizers and functional appliances. In fact, when samples of patients treated with either fixed-functional appliances or molar distalization were compared, the overall effects were quite similar, and the amount of mandibular growth contributing to the Class II correction was identical.72 Treatments addressing either jaw resulted in the same amount of mandibular growth. Clearly, the interruption of dentoalveolar compensation is the key to the resolution of Class II malocclusion for most growing patients, whether the mechanism is headgear, Class II elastics, distalizers, or functional appliances.69,73 As more research is conducted on these disparate methods, it should sharpen our focus on selecting the best tool for a particular patient. Until then, clinical choices appear to be more a matter of practice management than of biological advantage.
Once distalized, the molars must be held in position as the remaining maxillary teeth are retracted to reduce protrusion, resolve overbite, close spaces, and achieve a Class I canine relationship. Molars have been retained with a variety of devices, including modified plastic retainers, headgears, lip bumpers, stopped wires with Class II elastics, fixed-functional appliances (Class II combination therapy36,53), and modified Nance holding arches (acrylic palatal buttons).8,35 Whether the anterior retraction is achieved with sectional, sliding, or closing-loop mechanics, the anchorage requirements are the same.36,54,74-76 Would you risk relying on the distalized upper molars for this anchorage? Why distalize at all, if other devices and mechanics still have to be used to finish the correction?70 Of course, the same question can be raised about functional appliances, since full fixed appliances and elastics will likely be required to maintain the artificially advanced mandibular position while growth catches up.71
It would be an advantage if the same appliance that produced the distalization could also function as anchorage for retraction. That was the unique design of the Distal Jet, as a device that could be converted to a modified Nance holding arch while still seated in the mouth.8,34-37 Unfortunately, the Nance holding arch does not always provide enough anchorage support. If supplementation with elastics or headgear is required, it reintroduces issues of patient compliance.36,53,54,74 To date, the concept of a completely "non-compliant" orthodontic mechanism has been something of a pipe-dream.
Conclusion
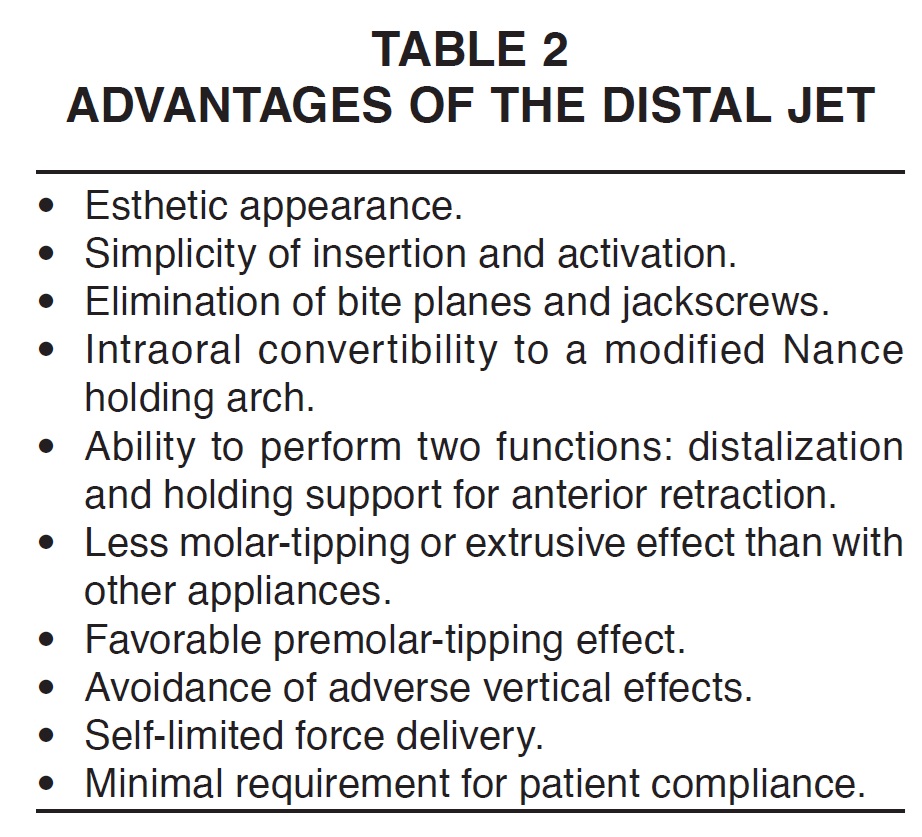
Whether the chosen distalization method requires patient compliance to achieve any progress (as with headgear, the Carriere device, bimetric maxillary arches, or the acrylic cervical occipital appliance) or reduces those cooperation requirements (as with the Jones Jig, the Pendulum, fixed-functional appliances, or the Distal Jet), the results appear to be similar. Once the molars have been distalized, the mechanics required to complete the rest of the correction are as important as the distalization method itself. It would therefore seem preferable to select a device that is simple, comfortable, versatile, esthetic, hygienic, easy to comply with, cost-effective, self-limiting, and yet predictable, effective, and efficient, with minimal undesirable side effects (Table 2). The next logical step in the evolution of upper-molar distalization will involve the application of skeletal anchorage.
FOOTNOTES
- *American Orthodontics, Sheboygan, WI; www.americanortho.com.
- **Ormco Corporation, Orange, CA; www.ormco.com.
- ***Henry Schein Orthodontics, Melville, NY; www.henryschein.com.
REFERENCES
- 1. Angle, E.H.: The Treatment of Malocclusion of the Teeth, 7th ed., S.S. White Dental Manufacturing Co., Philadelphia, 1907.
- 2. Graber, T.M.: Extraoral force - fact and fallacies, Am. J. Orthod. 41:490-505, 1955.
- 3. Lai, M.: Molar distalization with the Herbst appliance, Semin. Orthod. 6:119-128, 2000.
- 4. Cetlin, N.M. and Ten Hoeve, A.: Nonextraction treatment, J. Clin. Orthod. 17:396-413, 1996.
- 5. Hilgers, J.J.: The Pendulum appliance for Class II non-compliance therapy, J. Clin. Orthod. 26:706-714, 1992.
- 6. Walde, K.C.: The simplified molar distalizer, J. Clin. Orthod. 37:616-619, 2003.
- 7. Jones, R.D. and White, J.M.: Rapid Class II molar correction with an open-coil jig, J. Clin. Orthod. 26:661-664, 1992.
- 8. Carano, A. and Testa, M.: The Distal Jet for upper molar distalization, J. Clin. Orthod. 30:374-380, 1996.
- 9. Keles, A.; Erverdi, N.; and Sezen, S.: Bodily distalization of molars with absolute anchorage, Angle Orthod. 73:471-482, 2003.
- 10. Gianelly, A.A.; Vaitas, A.S.; and Thomas, W.M.: The use of magnets to move molars distally, Am. J. Orthod. 96:161-167, 1989.
- 11. Bondemark, L. and Kurol, J.: Distalization of maxillary first and second molars simultaneously with repelling magnets, Eur. J. Orthod. 14:264-272, 1992.
- 12. Locatelli, R.; Bednar, J.; Deitz, V.S.; and Gianelly, A.A.: Molar distalization with superelastic NiTi wire, J. Clin. Orthod. 26:277-279, 1992.
- 13. Carriere, L.: A new Class II distalizer, J. Clin. Orthod. 38:224-231, 2004.
- 14. Muse, D.S.; Fillman, M.J.; Emmerson, W.J.; and Mitchell, R.D.: Molar and incisor changes with Wilson rapid molar distalization, Am. J. Orthod. 104:556-565, 1993.
- 15. Gianelly, A.A.: Bidimensional Technique Theory and Practice, GAC International, Islandia, NY, 2000.
- 16. Patel, A.N.: Analysis of the Distal Jet appliance for maxillary molar distalization, thesis, University of Oklahoma, Oklahoma City, 1999.
- 17. Greenfield, R.L.: Fixed piston appliance for rapid Class II correction, J. Clin. Orthod. 29:174-183, 1995.
- 18. Owen, A.H. III: The maxillary sagittal appliance: A clinical study, Am. J. Orthod. 91:271-285, 1987.
- 19. Angelieri, F.; Almedia, R.R.; Almeida, M.R.; and Fuziy, A.: Dentoalveolar and skeletal changes associated with the Pendulum appliance followed by fixed orthodontic treatment, Am. J. Orthod. 129:520-527, 2006.
- 20. Mavropoulos, A.; Karamouzos, A.; Kiliaridis, S.; and Papadopoulos, M.A.: Efficiency of noncompliance simultaneous first and second molar distalization: A three dimensional tooth movement analysis, Angle Orthod. 75:532-539, 2005.
- 21. Papadopoulos, M.A.; Mavropoulos, A.; and Karamouzos, A.: Cephalometric changes following simultaneous first and second molar distalization using a non-compliance intraoral appliance, J. Orofac. Orthop. 65:123-136, 2004.
- 22. Kinzinger, G.S.; Fritz, U.B.; Sander, F.G.; and Diedrich, P.R.: Efficiency of a Pendulum appliance for molar distalization related to second and third molar eruption stage, Am. J. Orthod. 125:8-23, 2004.
- 23. Brickman, C.D.; Sinha, P.K.; and Nanda, R.S.: Evaluation of the Jones Jig appliance for distal molar movement, Am. J. Orthod. 118:526-534, 2000.
- 24. Runge, M.E.; Martin, J.T.; and Bukai, F.: Analysis of rapid maxillary molar distal movement without patient cooperation, Am. J. Orthod. 115:153-157, 1999.
- 25. Kinzinger, G.S.; Wehrbein, H.; and Diedrich, P.R.: Molar distalization with a modified Pendulum appliance - In vitro analysis of the force systems and an in vivo study in children and adolescents, Angle Orthod. 75:558-567, 2005.
- 26. Bussick, T.J. and McNamara, J.A. Jr.: Dentoalveolar and skeletal changes associated with the Pendulum appliance, Am. J. Orthod. 177:333-343, 2000.
- 27. Byloff, F.K. and Darendeliler, M.A.: Distal molar movement using the Pendulum appliance, Part 1: Clinical and radiological evaluation, Angle Orthod. 67:249-260, 1997.
- 28. Chaques-Asensi, J. and Kalra, V.: Effects of the Pendulum appliance on the dentofacial complex, J. Clin. Orthod. 35:254- 257, 2001.
- 29. Ghosh, J. and Nanda, R.S.: Evaluation of an intraoral maxillary molar distalization technique, Am. J. Orthod. 110:639- 646, 1996.
- 30. Chiu, P.P.; McNamara, J.A. Jr.; and Franchi, L.: A comparison of two intraoral molar distalization appliances: Distal Jet versus Pendulum, Am. J. Orthod. 128:353-365, 2005.
- 31. Ferguson, D.J.; Carano, A.; Bowman, S.J.; Davis, E.C.; Gutierrez Vega, M.E.; and Lee, S.H.: A comparison of two maxillary molar distalizing appliances with the Distal Jet, World J. Orthod. 6:382-390, 2005.
- 32. Byloff, F.K.; Darendeliler, M.A.; Clar, E.; and Darendeliler, A.: Distal molar movement using the Pendulum appliance, Part 2: The effects of maxillary molar root uprighting bends, Angle Orthod. 67:261-270, 1997.
- 33. Bolla, E.; Muratore, F.; Carano, A.; and Bowman, S.J.: Evaluation of maxillary molar distalization with the Distal Jet, Angle Orthod. 72:481-494, 2002.
- 34. Carano, A.; Testa, M.; and Bowman, S.J.: The Distal Jet: Simplified and updated, J. Clin. Orthod. 36:586-590, 2002.
- 35. Bowman, S.J.: Modifications of the Distal Jet, J. Clin. Orthod. 32:549-556, 1998.
- 36. Bowman, S.J.: Class II combination therapy: Molar distalization and fixed functional appliances, in Current Therapy in Orthodontics, ed. R. Nanda and S. Kapila, Mosby, St. Louis, 2009, pp. 115-136.
- 37. Bowman S.J.: Distal Jets refined: Bowman modification and Horseshoe Jet, AOAppliances, 11:1-5, 2008.
- 38. Hansen, K.; Koutsonas, T.G.; and Pancherz, H.: Long-term effects of Herbst treatment on the mandibular incisor segment: A cephalometric and biometric investigation, Am. J. Orthod. 112:92-103, 1997.
- 39. Nalbantgil, D.; Arun, T.; Sayinsu, K.; and Fulya, I.: Skeletal, dental and soft-tissue changes induced by the Jasper Jumper appliance in late adolescence, Angle Orthod. 75:426-436, 2005.
- 40. May, P.W.; Chada, J.; Ledoux, W.R.; Weinberg, P.; Block, M.S.; and McMinn, R.W.: Skeletal and dental changes using a Jasper Jumper appliance, J. Dent. Res. 71:1645, 1992.
- 41. Rothenberg, J.; Campbell, E.S.; and Nanda, R.: Class II correction with the Twin Force Bite Corrector, J. Clin. Orthod. 38:232-240, 2004.
- 42. Ruf, S.; Hansen, K.; and Pancherz, H.: Does orthodontic proclination of lower incisors in children and adolescents cause gingival recession? Am. J. Orthod. 114:100-106, 1998.
- 43. Aslan, B.I.; Kucukkaraca, E.; Turkoz, C.; and Dincer, M.: Treatment effects of the Forsus Fatigue Resistant Device used with miniscrew anchorage, Angle Orthod. 84:76-87, 2014.
- 44. Berkman, M.E.; Haerian, A.; and McNamara, J.A. Jr.: Interarch maxillary molar distalization appliances for Class II correction, J. Clin. Orthod. 42:35-42, 2008.
- 45. Nance, H.N.: The limitations of orthodontic treatment; mixed dentition diagnosis and treatment, Am. J. Orthod. 33:177-223, 1947.
- 46. Ngantung, V.; Nanda, R.S.; and Bowman, S.J.: Posttreatment evaluation of the Distal Jet appliance, Am. J. Orthod. 120:178- 185, 2001.
- 47. Huerter, G.: A retrospective evaluation of maxillary molar distalization with the Distal Jet appliance, thesis, St. Louis University, St. Louis, 2000.
- 48. Gutierrez, V.M.E.: Treatment effects of the Distal Jet appliance with and without edgewise therapy, thesis, St. Louis University, St. Louis, 2001.
- 49. Maginnis, J.J.: Treatment effects of the Distal Jet with 180 gram and 240 gram springs, thesis, St. Louis University, St. Louis, 2002.
- 50. Lee, S.H.: Comparison of treatment effects of two molar distalization appliances, thesis, St. Louis University, St. Louis, 2001.
- 51. Davis, E.C.: A comparison of two maxillary molar distalization appliances, thesis, St. Louis University, St. Louis, 2001.
- 52. Cali, L.: Comparing two methods of non-compliance Class II therapy: The Distal Jet and the SMD (frog), thesis, St. Louis University, St. Louis, 2011.
- 53. Bowman, S.J.: Class II combination therapy, J. Clin. Orthod. 32:611-620, 1998.
- 54. Bowman, S.J.: Class II combination therapy (Distal Jet and Jasper Jumpers): A case report, J. Orthod. 27:213-218, 2000.
- 55. Bowman, S.J.: Class II correction and orthodontics for the non-compliant patient, Gutta Percha Clarion, Kalamazoo Valley District Dental Society Newsletter, Spring 1993, pp. 13-17.
- 56. Bowman, S.J.: The Distal Jet appliance: Class II correction by maxillary molar distalization, Belg. Tijds. Orthod. 3:65-72, 2002.
- 57. Melsen, B. and Bosch, C.: Different approaches to anchorage: A survey and an evaluation, Angle Orthod. 67:23-30, 1997.
- 58. Williams, R.E.: Letter to the editor: Distal Jet appliance, Am. J. Orthod. 121:9A, 2002.
- 59. Ngantung, V.; Nanda, R.S.; and Bowman, S.J.: Author's response, Am. J. Orthod. 120:14A-15A, 2001.
- 60. McNamara, J.A. Jr. and Brudon, W.L.: Orthodontic and Orthopedic Treatment in the Mixed Dentition, Needham Press, Ann Arbor, MI, 1993.
- 61. Lamons, F.F. and Holmes, C.W. III: The problem of the rotated maxillary first permanent molar, Am. J. Orthod. 47:246- 272, 1961.
- 62. De Baets, J. and Chiarini, M.: The pseudo-Class I: A newly defined type of malocclusion, J. Clin. Orthod. 29:73-88, 1995.
- 63. Korn, M. and Shapiro, E.: Flexible lip bumpers for arch development, J. Clin. Orthod. 28:43-49, 1994.
- 64. Nishii, Y.; Katada, H.; and Yamaguchi, H.: Threedimensional evaluation of the Distal Jet appliance, World J. Orthod. 3:321-327, 2002.
- 65. Kinzinger, G.S. and Diedrich, P.R.: Biomechanics of a Distal Jet appliance: Theoretical considerations and in vitro analysis of force systems, Angle Orthod. 78:676-681, 2008.
- 66. Flores-Mir, C.; McGrath, L.; Heo, G.; and Major, P.W.: Efficiency of molar distalization associated with second and third molar eruption stage, Angle Orthod. 83:735-742, 2013.
- 67. Liu, S.S. and Buschang, P.H.: How does tooth eruption relate to vertical mandibular growth? Am. J. Orthod. 139:745-751, 2011.
- 68. Donaghey, J.B.: A cephalometric evaluation of tooth movement and growth of the jaws in untreated individuals, ages 11- 15, thesis, St. Louis University, St. Louis, 1986.
- 69. Tsourakis, A.K. and Johnston, L.E. Jr.: Class II malocclusion: The aftermath of a "perfect storm", Semin. Orthod. 20:59-73, 2014.
- 70. Watson, W.G.: Letter to the editor: Distal Jet versus Pendulum appliance, Am. J. Orthod. 129:3, 2006.
- 71. Johnston, L.E. Jr.: Functional appliances: A mortgage on mandibular position, Aus. Orthod. J. 14:154-157, 1996.
- 72. Burkhardt, D.R.; McNamara, J.A. Jr.; and Baccetti, T.: Maxillary molar distalization or mandibular enhancement: A cephalometric comparison of comprehensive orthodontic treatment including the Pendulum and the Herbst appliances, Am. J. Orthod. 123:108-116, 2003.
- 73. Johnston, L.E. Jr.: A comparative analysis of Class II treatment methods, in Science and Clinical Judgment in Orthodontics, ed. J.A. McNamara Jr., D.S. Carlson, P.S. Vig, and K.A. Ribbens, Center for Human Growth and Development, University of Michigan, Ann Arbor, MI, 1986, pp. 103-148.
- 74. Bowman, S.J.: Alternatives after molar distalization, Am. Orthod. Good Pract. 1:2-3, 2000.
- 75. Carano, A. and Bowman, S.J.: Non-compliance Class II treatment with the Distal Jet, in Orthodontic Treatment of the Class II Noncompliant Patient: Current Principles and Techniques, ed. M.A. Papadopoulos, Elsevier-Mosby, Edinburgh, 2006, pp. 265-289.
- 76. Bolla, E.; Doldo, T.; and Giorgetti, R.: Distal movement of maxillary canines and premolars with sectional mechanics following Distal Jet application to molars, Prog. Orthod. 5:72- 89, 2004.
-
 DR. BOWMAN
DR. BOWMAN
Dr. Bowman is a Contributing Editor of the Journal of Clinical Orthodontics; an Adjunct Associate Professor, St. Louis University, St. Louis; a straight-wire instructor, University of Michigan, Ann Arbor, MI; an Assistant Clinical Professor, Case Western Reserve University, Cleveland; a Visiting Clinical Lecturer, Seton Hill University, Greensburg, PA; and in the private practice of orthodontics in Portage, MI; e-mail: drjwyred@aol.com.