Clinical Application of the PASS Technique
Molar anchorage loss has been shown to occur during the early stages of alignment with preadjusted appliances.1,2 The most commonly used archwires for initial alignment are made of nickel titanium, which has the elasticity to provide light, continuous forces but cannot accommodate the tipback bends needed to preserve molar anchorage. Among the methods developed to reinforce anchorage, headgear was once widely used but has not been entirely effective, even in compliant patients.3 Temporary anchorage devices (TADs) are more reliable but may be rejected by some patients and can only be placed in sites with optimal bone condition.
In recent years, self-ligating brackets have been advocated as a means of reducing wire-bracket friction, as well as allowing longer appointment intervals and fewer visits.4,5 Low friction is most advantageous during initial alignment, however, whereas friction is needed for control in finishing and torque expression. If the friction level of a bracket could be adjusted for different treatment stages, orthodontic tooth movement would be more efficient.
The Physiological Anchorage Spee-wire System (PASS)* was designed to optimize natural anchorage preservation while controlling friction and utilizing the elasticity of nickel titanium wires for initial alignment.6,7
Similar articles from the archive:
Appliance Design
The PASS appliance has two main components: a crossed buccal tube (XBT) consisting of a -7º main tube and a -25º tipback tube, crossing at the mesial end of the molar (Fig. 1A); and a multilevel low-friction (MLF) bracket (Fig. 1B).
In normal occlusion, the molars are tipped slightly forward, so that the mesiodistal angulation of the upper first molar is about 5º. Hence, the molar tube in the classic Straight-Wire Appliance, based on Andrews's six keys to normal occlusion,8 has a prescription of +5º. This prescription makes no allowance for molar anchorage preservation, however, and can be especially detrimental in extraction cases where the molars need to be maintained in an upright position or tipped back slightly before space closure. In a conventional preadjusted appliance, with the buccal tube positioned parallel to the line of buccal cusps, the passive archwire will lie below the anterior brackets because of the curve of Spee (Fig. 2A). When the anterior teeth are engaged, a counterclockwise tipforward moment will be created on the molar while the anterior teeth are extruded (Fig. 2B).
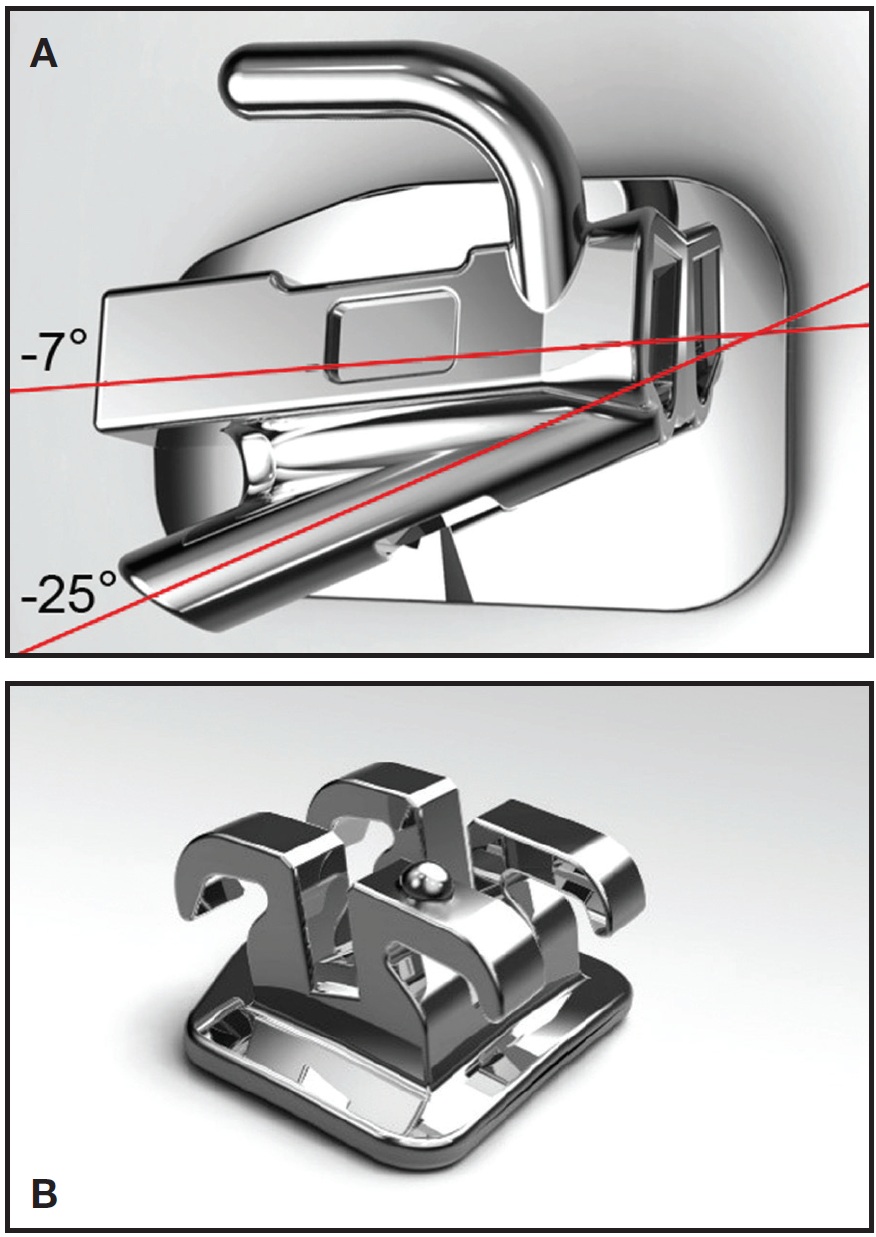
Fig. 1 Components of Physiological Anchorage Spee-wire System (PASS).* A. Crossed buccal tube (XBT). B. Multilevel low-friction (MLF) bracket.
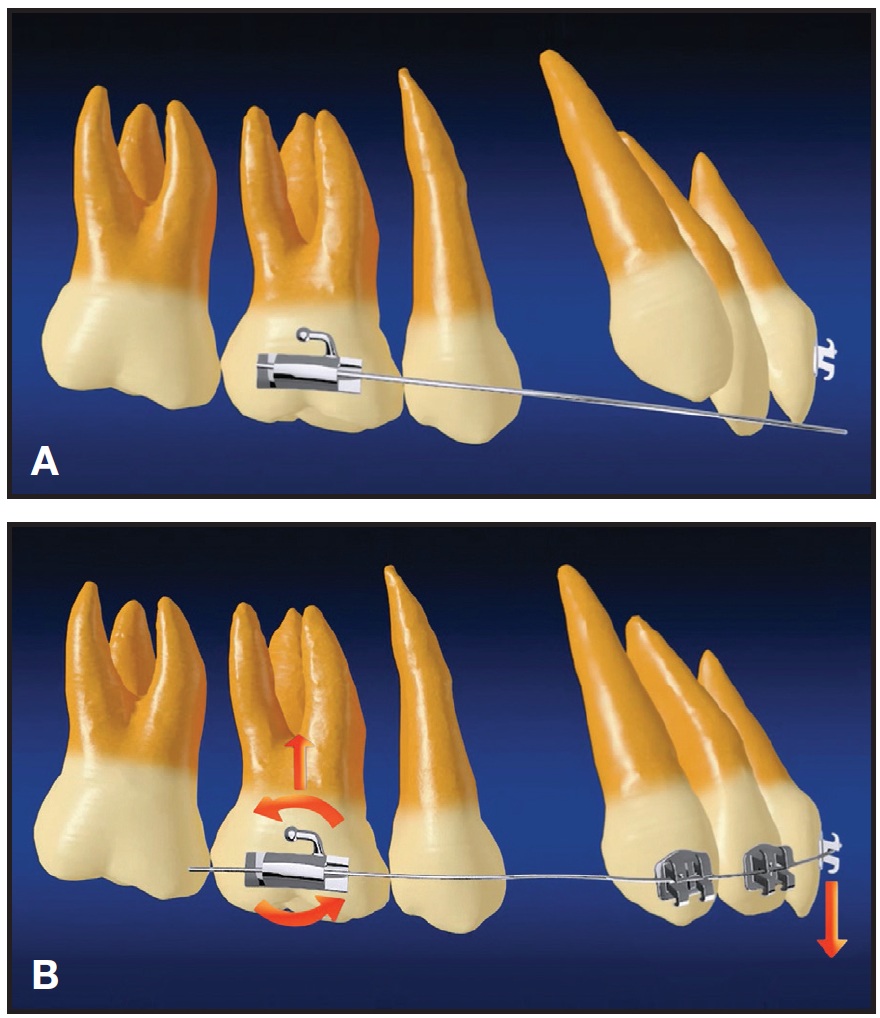
Fig. 2 Conventional preadjusted appliance. A. Passive archwire lies below anterior brackets. B. When archwire is engaged in anterior brackets, counterclockwise tip-forward moment is created on molar while incisors are extruded.
In the PASS technique, the initial archwire is inserted into the tipback tube, generating a protective moment for the anchor molars from the beginning of treatment (Fig. 3A). Engaging the wire into the anterior brackets from the gingival direction will help maintain the anterior overbite, which is important in most extraction cases (Fig. 3B). Molar anchorage is reinforced even when a light nickel titanium wire is used, without any wire bending. The double-tube design also facilitates the early use of a piggyback wire to control the upper-incisor vertical position during alignment and to promote bite opening in deep-bite cases (Fig. 4).
The MLF bracket has a constricted cervical area that can hold the ligature and keep it from compressing the archwire. A lighter archwire therefore experiences low friction during the alignment stage (Fig. 5A). As the archwire progresses to a larger size, the ligature contacts the wire and generates a controlled force for better expression of the bracket prescription (Fig. 5B). In addition, the vertical slots are sized at .020" for the incisors, allowing better torque control, and .022" for the rest of the teeth, providing optimal sliding mechanics.
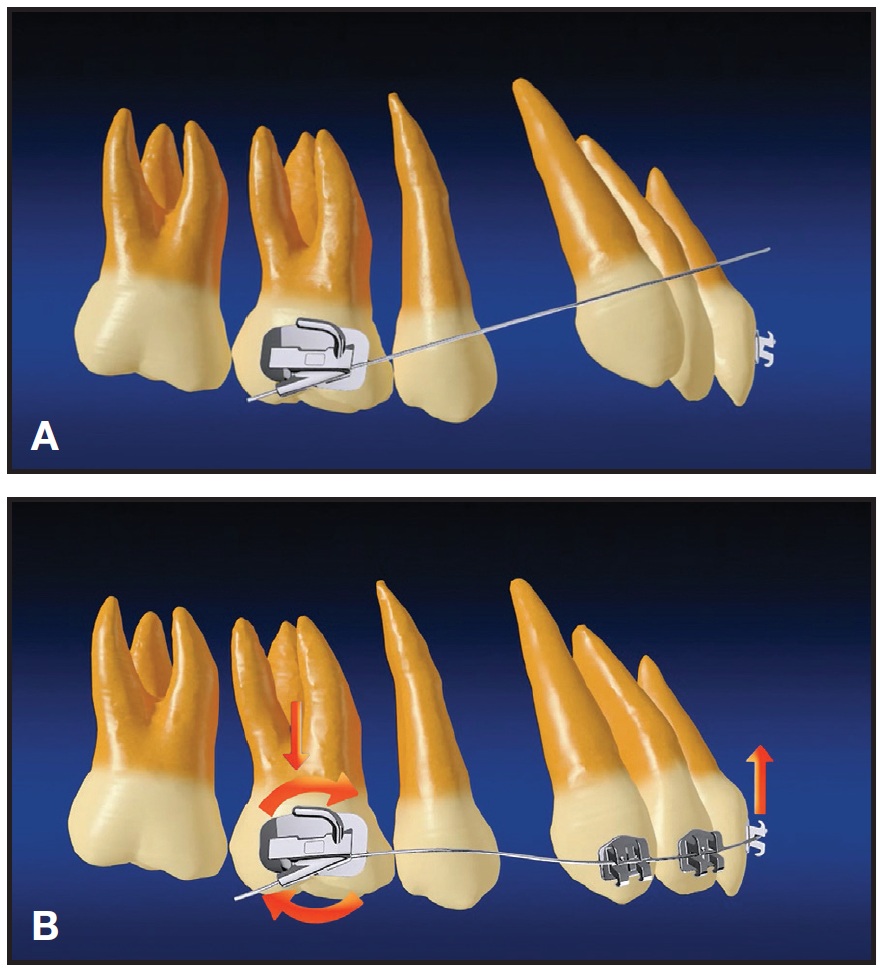
Fig. 3 PASS technique. A. Passive archwire inserted into tipback tube lies above anterior bracket. B. When archwire is engaged from gingival direction, protective moment for anchor molar is created and anterior overbite is maintained.
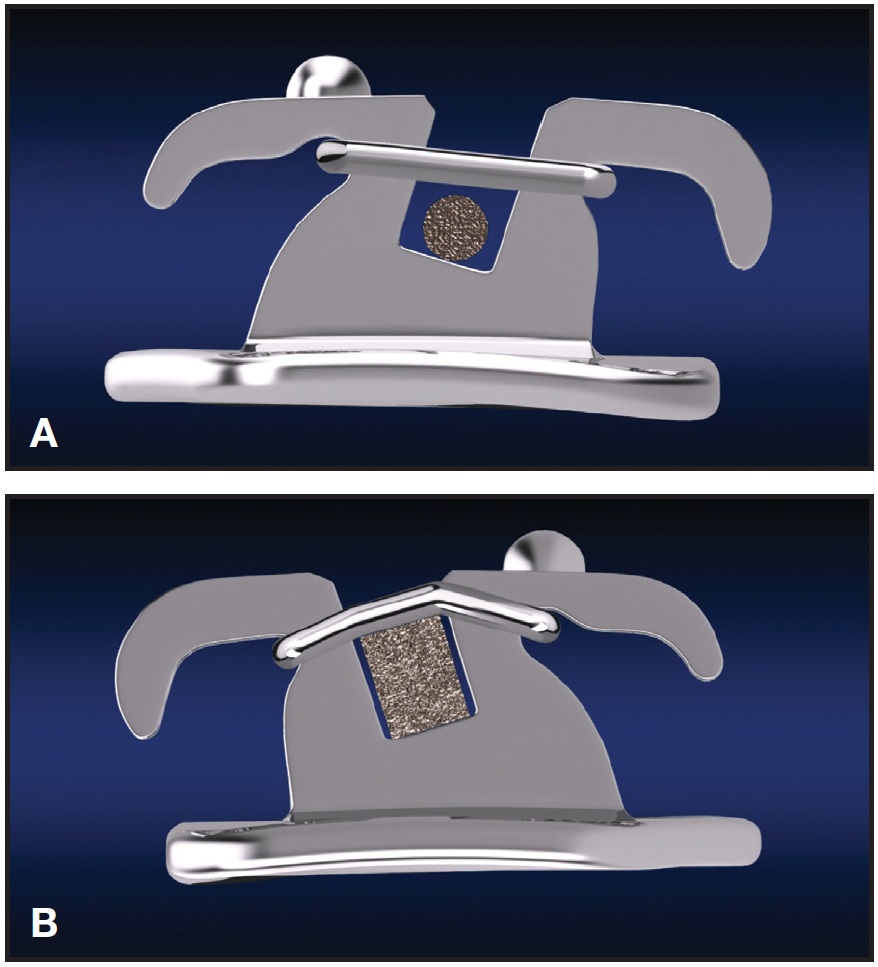
Fig. 5 A. With small initial archwire in MLF bracket, ligature is held in constricted cervical area, avoiding archwire compression and thus reducing friction. B. With larger finishing archwire, ligature exerts controlled force to express bracket prescription.

Fig. 4 .018" stainless steel piggyback wire can be inserted into main molar tube to control upper-incisor vertical position and promote bite opening in deep-bite case.
In a low-friction environment, gentle forces from lip pressure and tissue regeneration of extraction sites may be utilized to assist tooth movement.9 Because of the unique design of the XBT, the moment generated on a labially positioned canine - commonly seen in a patient with anterior crowding - will result in guided distal drift of the canine without the use of laceback ties (Fig. 6). Posterior anchorage is thus preserved while anterior crowding is relieved.10 The premolars are usually not bracketed for two to three months to allow a favorable molar-canine moment to be created. In the vertical dimension, the reaction force from molar tipback is diminished by the canine and balanced by lip pressure, similar to the effect of light-force self-ligating systems. Therefore, no J-hook headgear (as in the Tweed technique) or Class II elastics (as in the Begg technique) are needed to prevent the incisor flaring that would otherwise occur under the heavy tipback forces generated by stainless steel archwires.
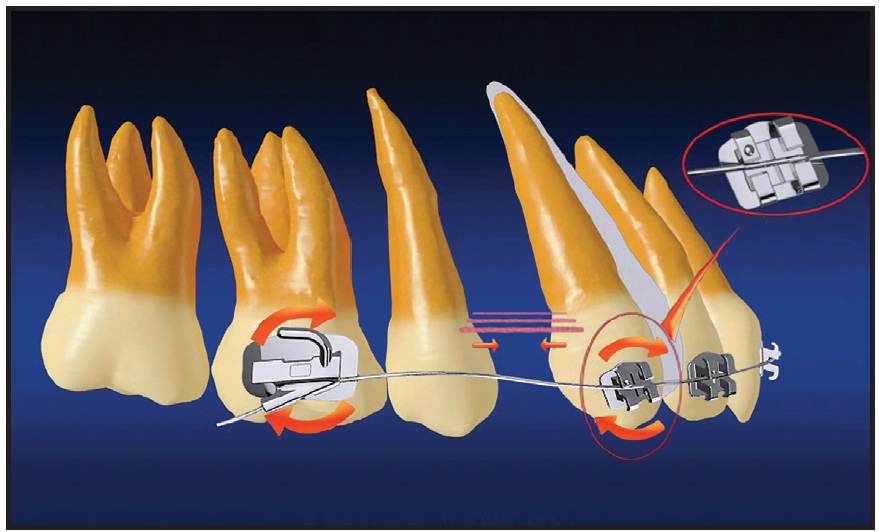
Fig. 6 Optimized molar-canine moment created by insertion of nickel titanium archwire into tipback tube; in low-friction environment, guided distal canine drift relieves anterior crowding without taxing molar anchorage.
Case Report
A 33-year-old female presented with the chief complaint of irregular teeth (Fig. 7).

Fig. 7 33-year-old female patient with anterior crowding and periodontally compromised condition before treatment.
She displayed a Class I malocclusion with severe anterior crowding - 10mm in the upper arch and 8mm in the lower - and the two upper lateral incisors in crossbite. Chronic periodontitis-related gingival recession was found, with the upper left canine the most affected: obvious bone loss had occurred on its buccal side, and the remaining attachment was fragile.
After routine periodontal treatment and observation for inflammation control, the four first premolars were extracted to provide space for orthodontic movement. To avoid placing a heavy load on the periodontally compromised teeth, we prescribed the PASS technique with its low-force mechanics and guided distal canine drift.
During initial alignment, .014" and .016" round nickel titanium archwires were inserted into the -25º tipback tubes (Fig. 8A). Distal canine movement occurred without laceback ties, and initial upper alignment was achieved in six months (Fig. 8B). Only minor upper-molar tipback was observed.

Fig. 8 A. .014" nickel titanium archwire inserted into XBT tipback tubes to facilitate distal canine drift. B. After six months of treatment, initial upper alignment achieved using .016" nickel titanium archwire, with minor upper-molar tipback but no periodontal deterioration.
In a total 23 months of treatment, the position of the upper molars was well maintained and the extraction space was efficiently used, not only for anterior alignment but also for retraction, thus improving the profile (Fig. 9A). Cephalometric superimpositions confirmed maximum molar anchorage control (Fig. 9B). The panoramic x-ray showed root parallelism without obvious root resorption. Further surgical and periodontal treatment was recommended to restore the upper-leftcanine defect and improve its attachment status.
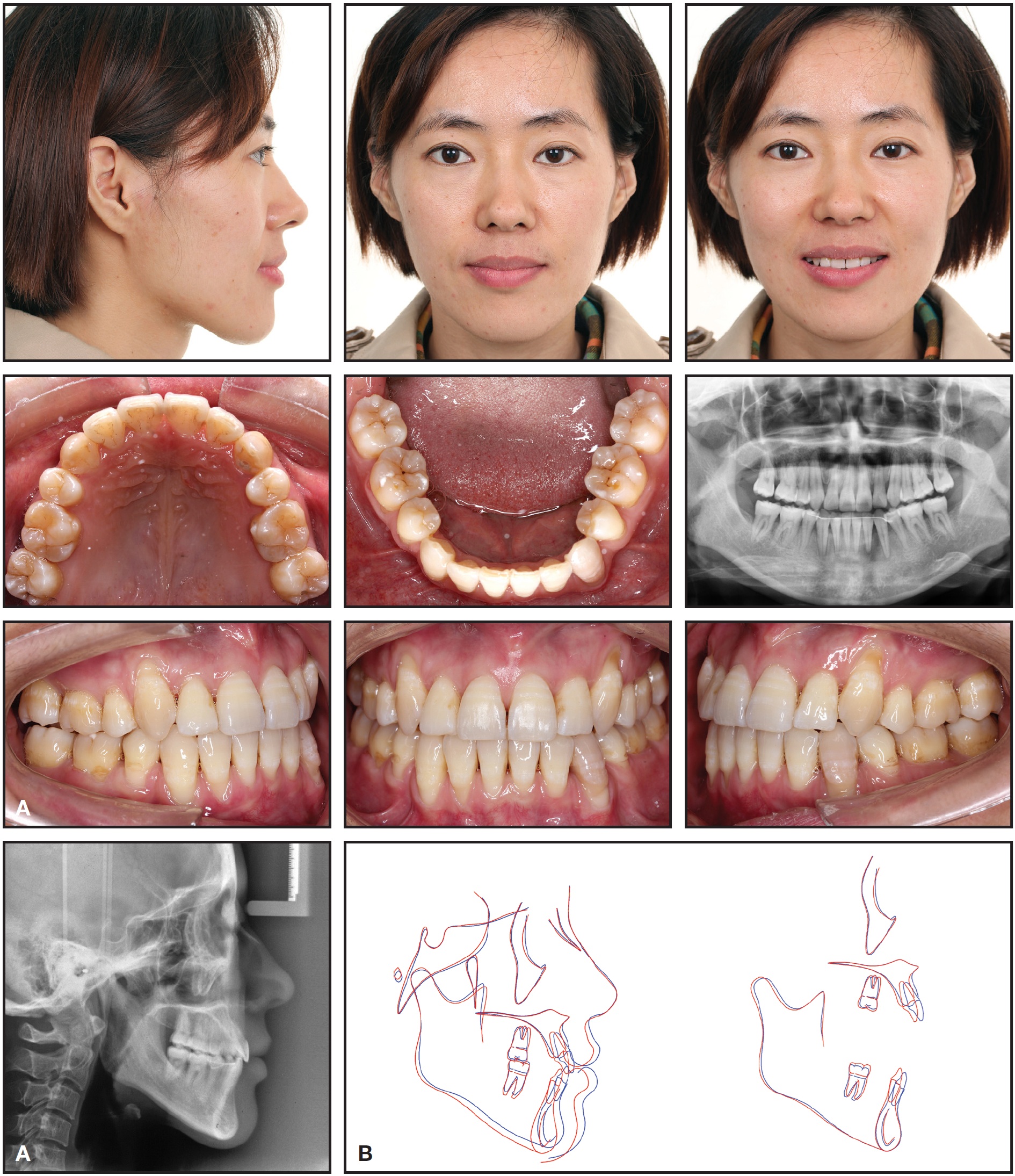
Fig. 9 A. Patient after 23 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Discussion
According to Su and colleagues, the upper first molars tend to be more distally tipped in younger patients, with more distally located lower molars and increased mandibular plane angles.6
In other words, high-angle Class II adolescent patients have the most desirable physiological conditions for natural anchorage preservation. Clinically, however, this kind of patient is most predisposed to anchorage loss. The PASS technique avoids the need for mechanical anchorage reinforcement by taking advantage of the patient's physiological anchorage, while the pretreatment molar positions are maintained during initial alignment with small nickel titanium archwires inserted in the XBT tipback tubes.2
Maintenance of the physiological curve of Spee during and after orthodontic treatment is emphasized in the PASS technique because this normal occlusal curvature is required for an efficient masticatory system. A geometrical curve of Spee that produces the most efficient pattern for maximizing tooth contacts during chewing has been considered an important goal of denture construction.11 It has been suggested that the curve of Spee performs a biomechanical function by increasing the crush-shear ratio between the posterior teeth, thus improving the efficiency of occlusal forces in food processing.12 From an anchorage-control perspective, an increased crush-shear ratio may enhance intermaxillary resistance to mesial molar movement, as in a lowangle case compared to a high-angle case. In a prospective clinical trial, the upper first molar tipped forward an average of 7.2º in the group treated with headgear3; therefore, keeping the upper first molar upright with the -7º XBT tube would save about 2mm of anchorage - nearly one-third of the premolar-extraction space in a maximum-anchorage case.
The main difference between the MLF bracket and conventional self-ligating brackets is that instead of using a clip, the MLF provides more clearance for the archwire inside the slot. According to Kusy and Whitley, adding more clearance increases the critical contact angle for binding and thus reduces sliding resistance.13 Although the situation may not be ideal for every tooth as orthodontic correction proceeds, overall friction will still be reduced. We have observed free sliding of the MLF bracket along an .014" archwire with an .008" ligature in vitro, but in vivo studies are still needed to substantiate these findings.
FOOTNOTES
- *Hangzhou Shinye Orthodontic Products Co., Zhengjiang, China; www.shinye-ortho.com.
REFERENCES
- 1. Rajesh, M.; Kishore, M.; and Shetty, K.S.: Comparison of anchorage loss following initial leveling and aligning using Roth and MBT prescription—A clinical prospective study, J. Int. Oral Health 6:16-21, 2014.
- 2. Su, H.; Han, B.; Li, S.; Na, B.; Ma, W.; and Xu, T.: Factors predisposing to maxillary anchorage loss: A retrospective study of 1403 cases, PLoS One 9:e10956, 2014.
- 3. Xu, T.; Zhang, X.; Oh, H.S.; Boyd, R.L.; Korn, E.L.; and Baumrind, S.: Randomized clinical trial comparing control of maxillary anchorage with 2 retraction techniques, Am. J. Orthod. 138:544.e1-544.e9, 2010.
- 4. Damon, D.H.: The rationale, evolution and clinical application of the self-ligating bracket, Clin. Orthod. Res. 1:52-61, 1998.
- 5. Shivapuja, P.K. and Berger, J.: A comparative study of conventional ligation and self-ligation bracket systems, Am. J. Orthod. 106:472-480, 1994.
- 6. Su, H.; Han, B.; Li, S.; Na, B.; Ma, W.; and Xu, T.M.: Compensation trends of the angulation of first molars: Retrospective study of 1403 malocclusion cases, Int. J. Oral Sci. 6:175-181, 2014.
- 7. Anchorage, in Fixed Orthodontic Appliances: Principles and Practice, ed. J.K. Williams, P.A. Cook, K.G. Isaacson, and A.R. Thom, Wright, Oxford, U.K., 1995, pp. 7-14.
- 8. Andrews, L.F.: The six keys to normal occlusion, Am. J. Orthod. 62:296-309, 1972.
- 9. Erikson, B.E.; Kaplan, H.; and Aisenberg, M.S.: A histological interpretation of repair phenomena following the removal of first premolars with retraction of the anterior segment, Am. J. Orthod. Oral Surg. 31:1-20, 1945.
- 10. Irvine, R.; Power S.; and McDonald F.: The effectiveness of laceback ligatures: A randomized controlled clinical trial, J. Orthod. 31:303-311, 2004.
- 11. Marshall, S.D.; Caspersen, M.; Hardinger R.R.; Franciscus, R.G.; Aquilino, S.A.; and Southard, T.E.: Development of the curve of Spee, Am. J. Orthod. 134:344-352, 2008.
- 12. Kumar, K.P. and Tamizharasi, S.: Significance of curve of Spee: An orthodontic review, J. Pharm. Bioallied Sci. 4:S323-S328, 2012.
- 13. Kusy, R.P. and Whitley J.Q.: Influence of archwire and bracket dimensions on sliding mechanics: Derivations and determinations of the critical contact angles for binding, Eur. J. Orthod. 21:199-208, 1999.
-
 DR. SI CHEN
DR. SI CHEN -
 DR. GUI CHEN
DR. GUI CHEN -
 DR. XU
DR. XU
Dr. Si Chen is a Clinical Associate Professor, Dr. Gui Chen is a Research Assistant, and Dr. Xu is a Professor, Department of Orthodontics, Peking University School and Hospital of Stomatology, 22 Zhongguancun South Avenue, Haidian District, Beijing 100081, China. Dr. Xu is the inventor of the PASS system; e-mail him at tmxuortho@163.com.