MANAGEMENT & MARKETING
Establishing an Optimal Pricing Strategy for Your Practice
Can an orthodontist create a fee schedule that is fair to patients while still providing maximum profits for the practice? This article will look objectively at various practice models and identify the optimal fee structure for each type, based on statistics I have collected from my own practice and those of my colleagues in recent years. I trust the information presented here will make you more confident in setting your own fees.
ROBERT S. HAEGER, DDS, MS
Establishing an Optimal Pricing Strategy for Your Practice
We'll start by identifying seven different types of orthodontic practices. Although their characteristics are not mutually exclusive, we'll consider them separately to give you a better understanding of how fees should be established in your own practice. Determining your practice model is only half of the equation, however; we'll also take a detailed look at five different pricing strategies, each of which can be incorporated as a whole or selectively, depending on your chosen practice model.
Seven Practice Models
1. High percentage of capitation or reduced-fee insurance-reimbursement patients: Medicaid and many insurance plans require discounting off the practice's customary fee schedule.
2. High percentage of patients with fees capped by insurance companies such as Delta Dental: These insurance companies limit the amount that can be charged to patients, even though they don't pay more than a set fee of $1,500-2,000.
Similar articles from the archive:
- MANAGEMENT & MARKETING Statistical Analysis of Two-Phase Treatment Compared with Single-Stage Comprehensive Treatment March 2008
- MANAGEMENT & MARKETING Increasing New Patient Starts by Analyzing Referral Sources and Treatment Coordinators March 2009
- MANAGEMENT & MARKETING Communicating with "No Future Appointment" Patients November 2008
3. High percentage of child patients: More than 80% of the practice's initial exams are for patients age 18 or younger.
4. High percentage of Phase I patients: More than 20% of the practice's child starts are for Phase I treatment.
5. High percentage of adult patients: More than 25% of the practice's total starts are patients age 19 or older.
6. Operating well below capacity: The practice is operating at less than 85% of capacity and thus has room to start 15% more patients.
7. Operating at full or close to full capacity: The practice is operating at more than 90% of capacity and thus has room to start less than 10% more patients.
Five Pricing Strategies
1. Market Pricing
Under this strategy, you find out what other local practices are charging and set your own fees accordingly. This can be done by asking second-opinion seekers about your competitors or asking a friend to set up exams at various offices to learn their new-exam procedures and prices. Although the "secret shopper" approach is advocated by several consultants as an easy way to gain competitive information, I consider it rather underhanded and unethical, because it actually takes money out of the wallet of another orthodontist. We can calculate that lost profit as follows, based on the average practice:
• About 43% of initial exams start treatment immediately; after future recalls, about 65% eventually start treatment.
• If the fee is $5,200 and the overhead rate is 60%, the profit per start is $5,200 x .40 = $2,080.
• Thus, the immediate cost of a non-starter, based on a 43% start rate, is $2,080 x .43 = $894.
• Based on a 65% start rate including recalls, the eventual cost of a "secret shopper" visit is $2,080 x .65 = $1,352.
Thus, by using your competitor's office for your fact-finding mission, you are not only taking insight from his or her practice, but actually taking almost $900 in short-term profit or more than $1,350 in ultimate profit. In that case, I maintain that you should be prepared to reimburse the other orthodontist for the lost income.
2. Two-Phase Pricing
The best way to assess two-phase pricing is to determine the number of visits required to treat patients in two phases compared to full treatment. You can then calculate the revenue generated per visit, which can be used to set your pricing strategy. Let's look at the results of a study of my own practice, published in the March 2008 issue of JCO1:
• 60 consecutively finished two-phase patients were compared to 394 single-stage patients finished with full treatment during the same period.
• 31 of the two-phase patients were Class I; 25 were Class II.
• 203 of the full-treatment patients were Class I; 180 were Class II.
• On average, the two-phase patients needed almost nine more months of total treatment and 10 more visits to finish.
• The combined fee for two-phase treatment was 23.9% higher, but the revenue per visit was 23.1% less (Fig. 1).
• Findings were similar when Class I and Class II subgroups were compared separately (Figs. 2,3).
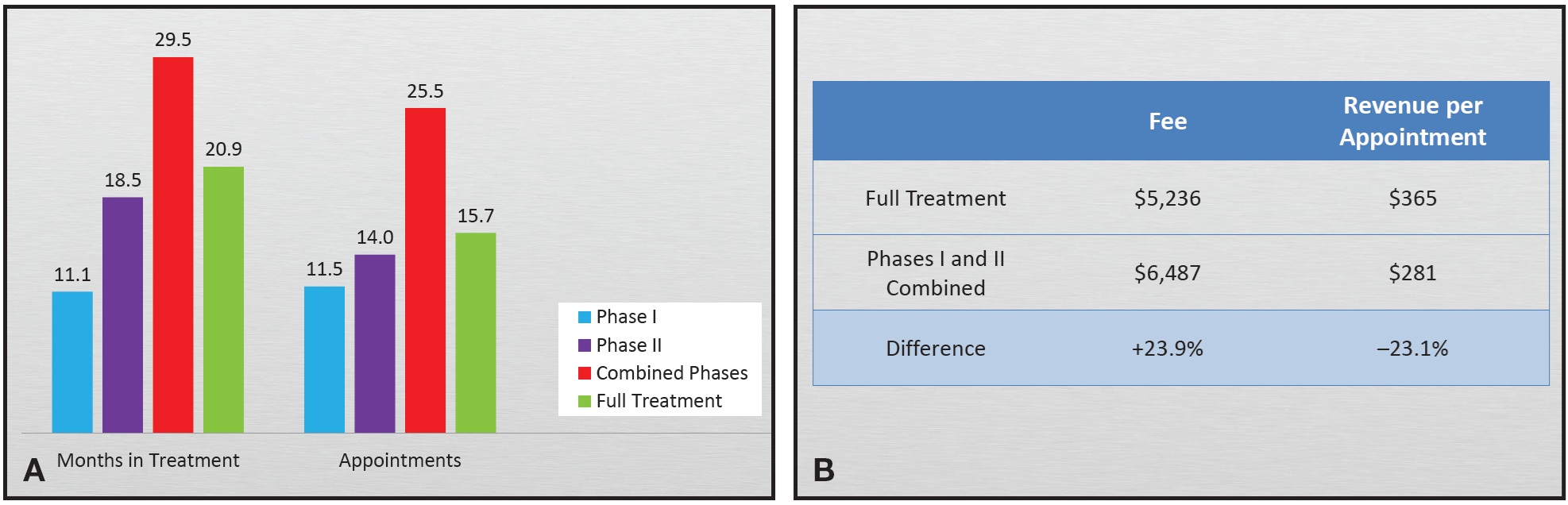
Fig. 1 Two-phase vs. full treatment. A. Months in treatment and number of appointments. B. Differences in total fee and revenue per appointment.
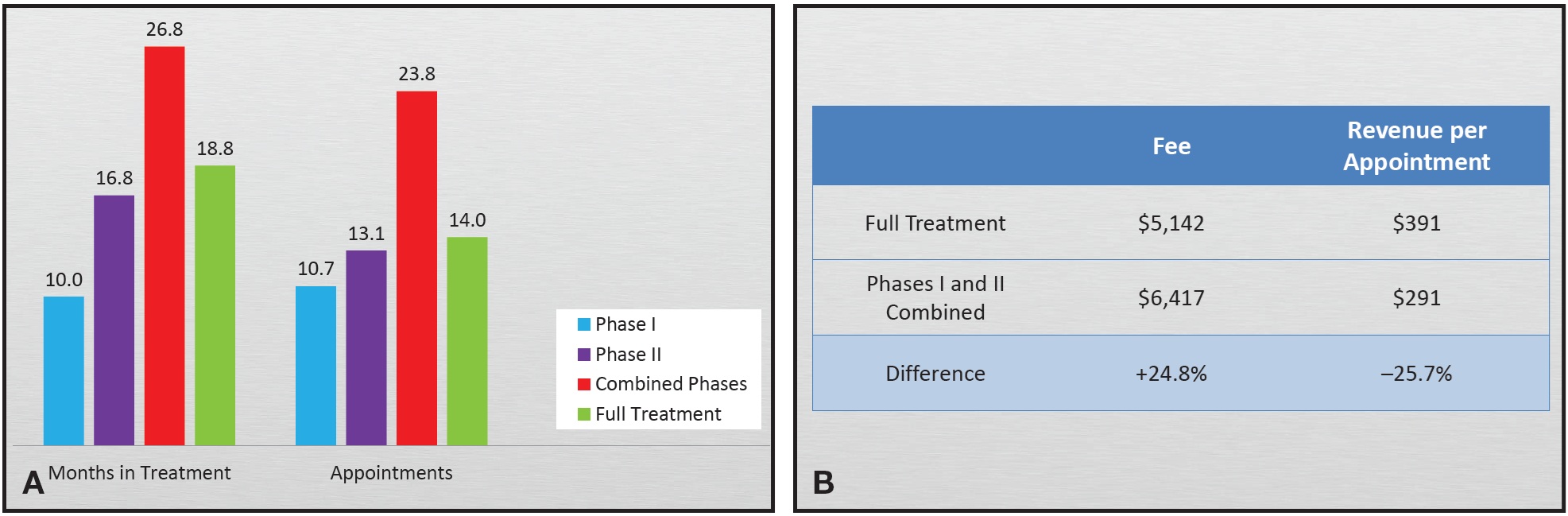
Fig. 2 Class I two-phase vs. full treatment. A. Months in treatment and number of appointments. B. Differences in total fee and revenue per appointment.
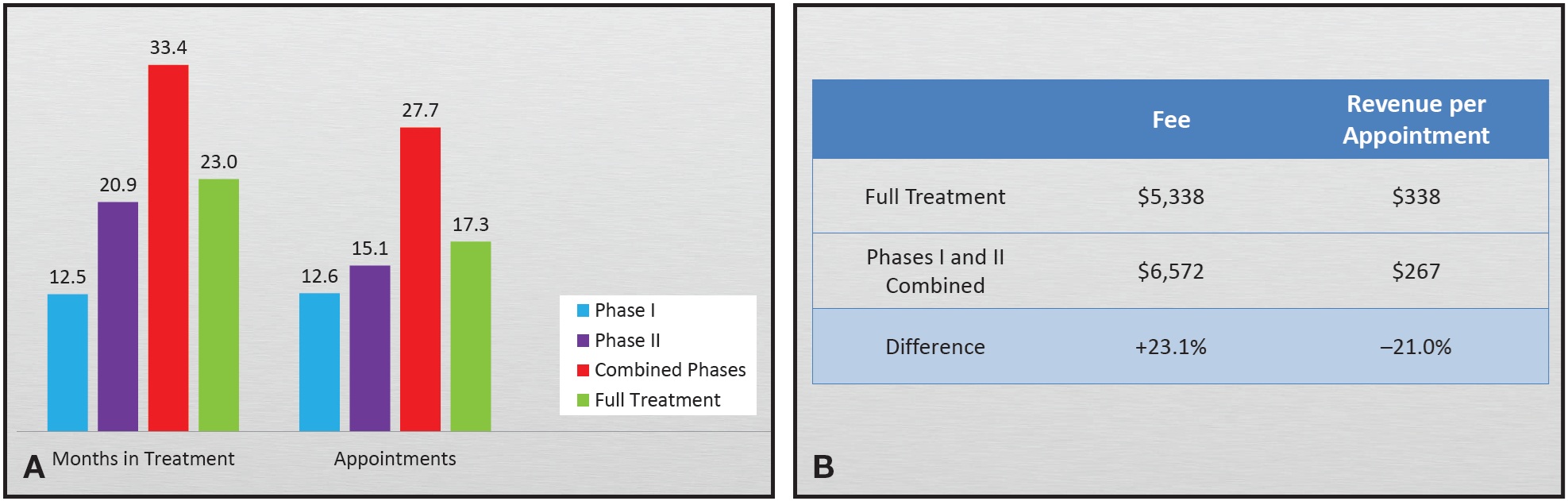
Fig. 3 Class II two-phase vs. full treatment. A. Months in treatment and number of appointments. B. Differences in total fee and revenue per appointment.
Based on these figures, I would have had to charge an average $3,547 more for two phases of treatment compared to full treatment to generate the same revenue per visit ($3,883 for Class I cases, $3,229 for Class II cases). According to 2013 data from Truenortho practices, profits are maximized when the charges for two phases of treatment total about $2,500 more than a full-treatment Class I fee. Even then, however, the practice is still not as productive per appointment as it would be if every patient were treated in a single stage.
3. Medical Pricing
There are two general strategies based on the medical model. To follow the first strategy, which we might call "everybody gets a discount":
- Set your fee high, even though no one actually pays that fee.
- Accept all insurance companies, and pass the discounts along to the patients
- Offer a 10-15% cash discount.
- Offer high discounts for sibling patients.
- Offer high discounts for immediate starts.
The second strategy is to price your service just below the next costlier alternative. For example, if an implant to replace a missing lower second premolar costs $5,000, set your fee to close the space using temporary anchorage devices (TADs) at $4,500. Since space closure prevents future crown replacement, you might charge more for child patients. If your community accepts the concept that treatment is more valuable when it is finished sooner, you should charge more for SureSmile or AcceleDent. This strategy requires positioning your practice as a premium product.
4. One Price Fits All
This traditional strategy involves setting one price for child patients and one for adults. Insurance companies favor such fee schedules, because the easy cases will subsidize the difficult ones. The risk is that you may lose the simpler cases to competitors. If you reduce your fee to stay competitive, the difficult cases will eat away your profits.
Furthermore, as your practice matures, your adult referrals will get more and more complex, and you'll have to bump up your adult fee if you don't want to end up paying to treat the interdisciplinary cases. Again, this strategy can cause you to lose the simple, high-profit-margin cases when patients shop around.
5. Charge Based on the Work Involved
The final strategy is to set your fee as a function of the projected treatment time and revenue per appointment. This creates a broad fee range based on the difficulty of each case, which is more equitable for both the practice and the patients. The major advantage compared to the one-price-fits-all strategy is that you do not have to subsidize the difficult cases with profits from the easy ones. You will win any price-shopping wars for the simple, highly profitable patients. If the complex patients choose to go somewhere else, that might be better than treating them at no profit. One potential risk is that if a new referring dentist decides to test your office by sending you difficult cases, you may appear to be the highest-priced orthodontist in the community.
In my practice, I tested the hypothesis that charging fees based on the work involved would be both fairer and more profitable by examining all new-patient exams and debonded cases from 2011 to 2013. Here were the results:
- For both child and adult cases finished during this period, the fees were indeed correlated with the number of months in treatment (Fig. 4A,B).
- With child new-patient exams, the decline rate increased as fees increased (Fig. 4C).
- With adult new-patient exams, the decline rate did not increase as fees increased (Fig. 4D).
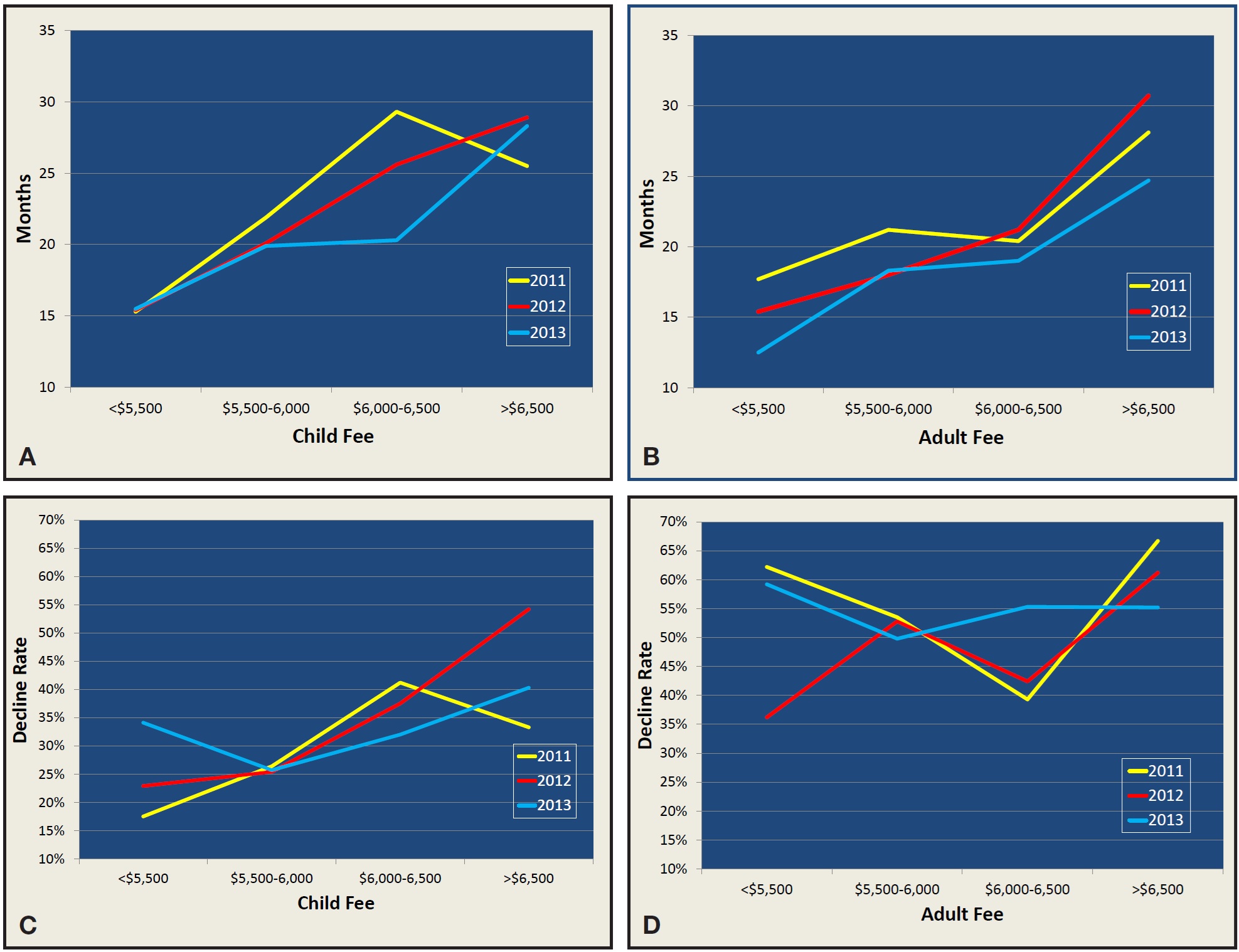
Fig. 4 Data from Dr. Haeger’s practice. A. Child fee vs. treatment time. B. Adult fee vs. treatment time. C. Child fee vs. decline rate. D. Adult fee vs. decline rate.
Based on this sample, what would have happened if I had capped my child fee at $6,000, in an effort to increase case acceptance by 10% among patients who were quoted higher fees?
• In 2011, 40 child patients were proposed treatment at fees greater than $6,000.
• A 10% higher conversion rate would have resulted in four new starts.
• At $6,000 per start, the additional patients would have generated $24,000 in new revenue.
• I would have lost the added revenue ($17,544) from all the other patients who accepted treatment at fees over $6,000.
$24,000 - $17,544 = $6,456 in additional revenue from the higher conversion rate.
• Since the practice was not at full capacity, the fixed costs (bands, brackets, supplies, retainers, etc.) for the four additional patients totaled $600 per patient. $6,456 - $2,400 = $4,056 in added profits.
• At full capacity and 60% overhead, four additional patients would have cost $24,000 x .6 = $14,400.
$24,000 - $14,400 - $17,544 = -$7,944 in lost profits.
Overall, because my practice was not operating at full capacity from 2011 to 2013, we lost more than $30,000 in potential profits by correlating treatment fees with treatment time (Fig. 5).
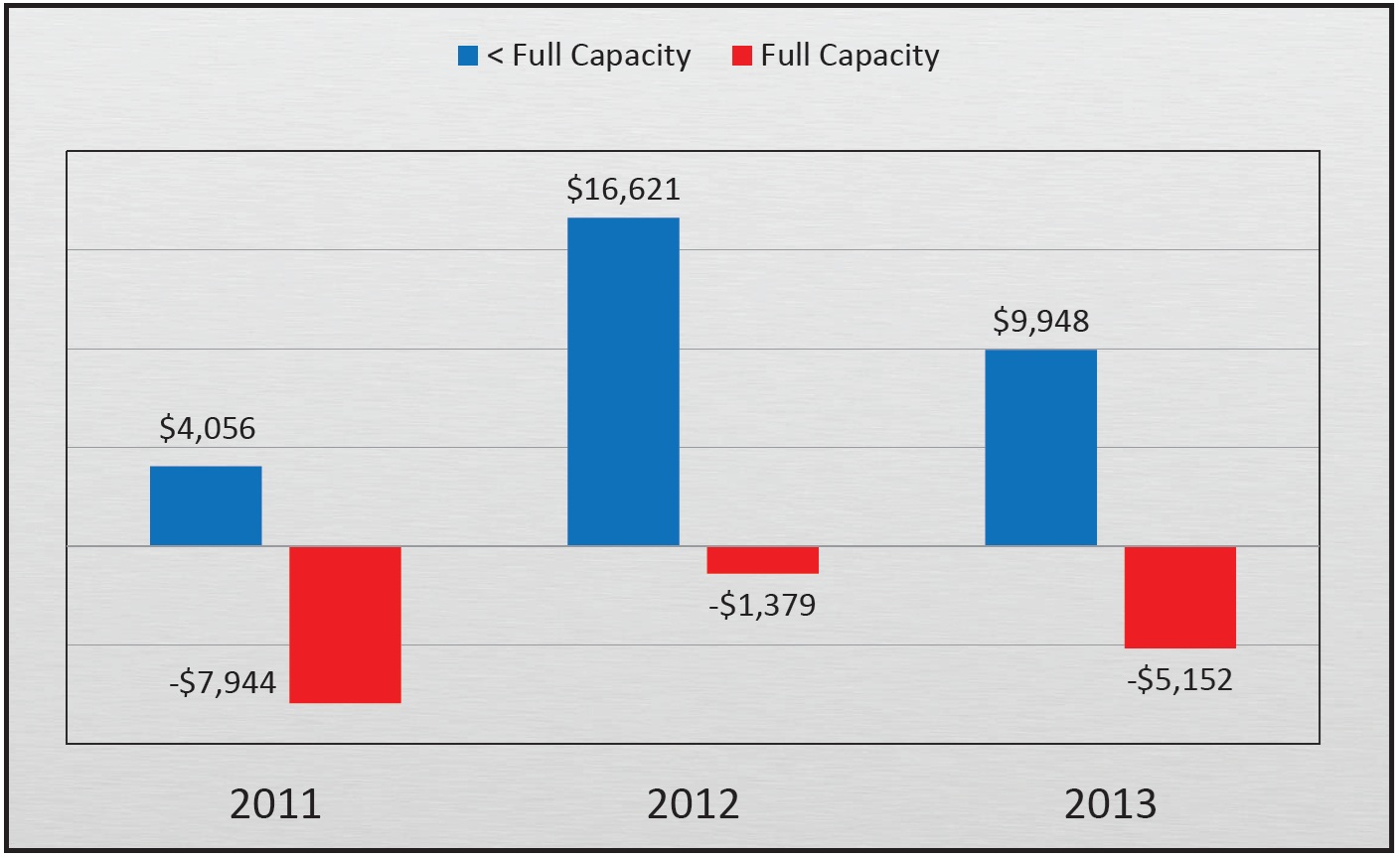
Fig. 5 Effect on profits of capping child fee at $6,000 in Dr. Haeger’s practice.
Discussion
Now, let's look at how the five pricing strategies apply to the seven orthodontic practice models.
1. High percentage of capitation or reduced-fee insurance-reimbursement patients.
These practices typically perform lots of two-phase treatment, because a Phase II fee usually falls below the insurance limit, and insurance companies make no distinction between Phase II and full treatment.
The one-price-fits-all model works well here for marketing purposes. Medical pricing where everybody gets a discount also works, starting with a high quoted fee and offering 10-15% cash discounts, substantial sibling discounts, $200-400 immediate-start discounts, and direct-mail discount coupons.
By referring TAD, surgical, and interdisciplinary cases to a local university, you can ensure better team treatment and avoid the higher costs.
2. High percentage of patients with fees capped by insurance companies such as Delta Dental.
This model similarly promotes two-phase treatment. It will not be advantageous for practices with high percentages of adult patients.
Under a one-price-fits-all strategy, you have to set fees high enough for the simple cases to cover the difficult cases. The risk with price-shopping patients is that you may lose the simple cases and win the difficult ones.
Charge separately for TADs, because the insurance company will pay extra for these devices. Refer complex TAD, surgical, and interdisciplinary cases to a local university for team treatment.
3. High percentage of child patients.
If you use medical pricing in which the fee is set just below the next costlier alternative, parents will tend to pay more to close spaces for missing teeth. Cap high-end fees at $750 above simple Class I cases, even though these patients may take twice as long to treat, because the higher conversion rate will make up for any lost revenue. Data from Truenortho confirm that practices with child-fee ranges between $600 and $750 have the highest profits. If determining a fee range proves too difficult, consider a simple two-tiered fee structure for child patients.
4. High percentage of Phase I patients.
Considering the analysis presented above, you should charge $2,500-2,700 more in total fees for two phases of treatment compared to a full Class I nonextraction child case. This strategy will be more palatable if you charge half the overall fee for Phase I, when esthetic improvements are often the most obvious.
5. High percentage of adult patients.
Do not use a one-price-fits-all model; charge adults based on the difficulty of the case, the projected esthetic improvement, and the treatment time. The conversion rate will not drop as the case fee increases. Adults understand the advantages of space closure vs. implants and will pay the additional fees required.
6. Operating well below capacity.
Stay away from one-price-fits-all unless you want to attract reduced-fee insurance-reimbursement patients. To maximize profits, keep your range of child fees at $750 or less. Charge extra for space closure by documenting the savings over implants to the patient and parents. Charge adults based on the work involved.
7. Operating at full or close to full capacity.
Limit your number of Phase I starts, because full treatment is more profitable per visit.
Your fee range should be about $2,000 for children and $3,000 for adults, who need twice as many visits. Even if your acceptance rate for child patients declines because of price shopping, you will still have enough patients who will pay the full fee.
Charge both children and adults extra for the work involved, for example
- $1,000 more to close spaces for missing lateral incisors.
- $750 more for missing lower second premolars without space closure.
- At least $2,000 more to close lower secondpremolar spaces with TADs.
- As much as $2,000 more for an impacted canine.
- $750 more to treat a 50% Class II.
- $1,750 more to treat a full Class II with a Herbst appliance*.
- $2,300 more for a case involving orthognathic surgery.
Conclusion
Every orthodontist needs to determine his or her practice model and recognize how the five pricing strategies described here will affect marketing, case conversion, and profitability. Fee ranges for children, adults, and two-phase treatment can then be set based on the practice's chosen model and its capacity for taking on new starts. In my experience, the most common fee structure in private practice involves a $750 fee range for children, a $2,500 range for adults, and an additional $2,500 in total fees for two phases of treatment.
FOOTNOTES
- *Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
REFERENCES
- 1. Haeger, R.S. and Colberg, R.T.: Statistical analysis of two-phase treatment compared with single-stage comprehensive treatment, J. Clin. Orthod. 42:149-154, 2008.
-
 DR. HAEGER
DR. HAEGER
Dr. Haeger is a Contributing Editor of the Journal of Clinical Orthodontics, founder and President of Truenortho, and in the private practice of orthodontics at 24909 104th Ave., S.E., Suite 203, Kent, WA 98030; e-mail: rhaeger@mybraces.net.