Easy Fabrication of an Occlusal Deprogrammer
The value of a deprogramming appliance for recording accurate centric relation, especially in cases with TMD, is well established. Horizontal and vertical overlapping of the anterior teeth can promote proper disclusion and effective long-term maintenance of the dentition, in addition to a better esthetic appearance.1
This article describes a simple deprogrammer, fabricated from a 1mm Essix* sheet with no need for wire bending.
Design and Fabrication
The deprogrammer is a combination of a thermoformed Essix retainer with an anterior biteplane to separate the posterior teeth. The biteplane should be just thick enough to eliminate proprioception and establish a single contact with one of the mandibular incisors. There should be no deviation when the mandible is protruded, and the patient should not be able to disengage during functional movements.2-4
Similar articles from the archive:
Fabrication is as follows:
1. Make full stone casts of both arches, omitting the entire palate from the maxillary cast.
2. Thermoform a 1mm Essix sheet over the upper cast (Fig. 1A). (A lower appliance can also be prepared if needed, as in a Class III case with no overjet or reverse overjet.)
3. With the Essix plate in place, mount the casts on a mean-value articulator in maximum intercuspation (Fig. 1B). No bite registration or facebow is required. Although mounting is not mandatory, it helps reduce chairtime.
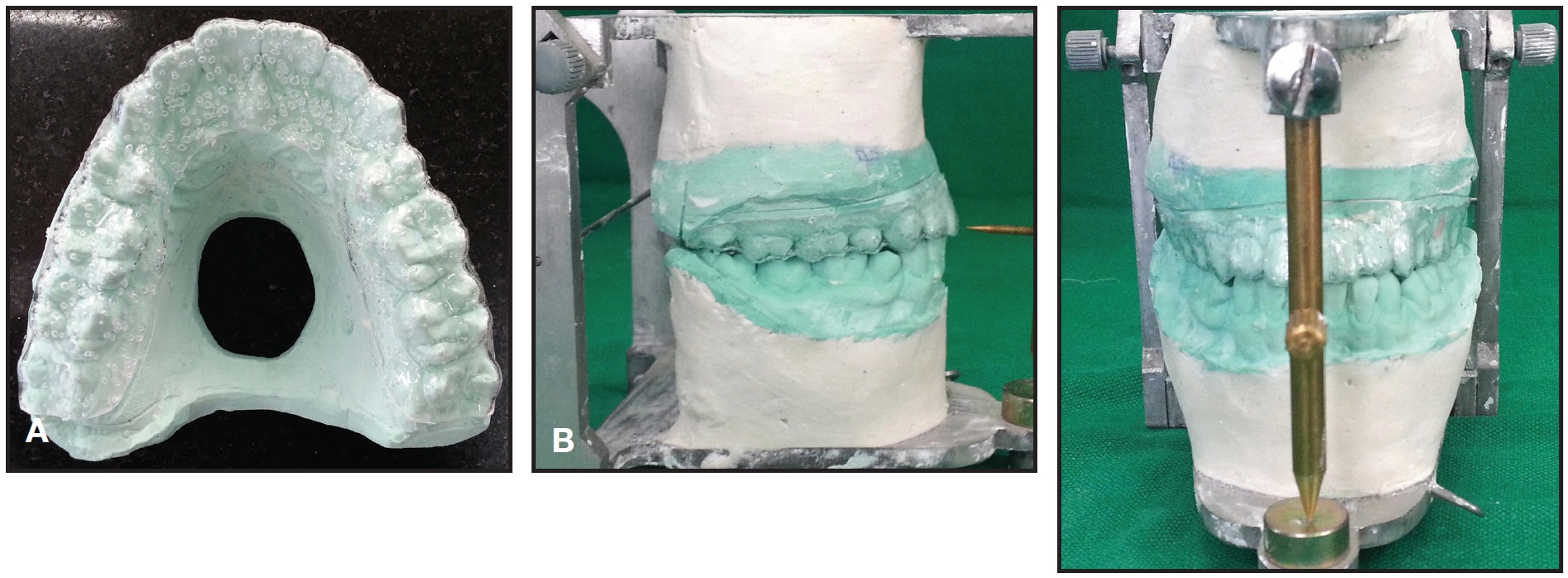
Fig. 1 A. Maxillary Essix plate thermoformed on plaster cast. B. Casts with maxillary Essix plate mounted on mean-value articulator in maximum intercuspation.
4. Using cold-cure acrylic, add a small bite platform on the palatal surface along the midline between the upper central incisors, so that there is a single point of contact with one of the mandibular incisors (Fig. 2).

Fig. 2 Cold-cure acrylic used to form biteplane between upper central incisors.
Extend this platform posteriorly 6-8mm, enough to prevent disengagement. Trim the biteplane perpendicular to the lower incisors.
5. Instruct the patient to wear the deprogrammer full-time except when eating or brushing.
At the follow-up examination, the patient can be considered deprogrammed if he or she occludes on the same spot repeatedly without any guidance. A patient who closes on more than one spot will need to wear the appliance longer5 (Fig. 3).
Case Report
A 25-year-old male reported with the chief complaint of facial asymmetry. Clinical examination showed a skeletal Class III malocclusion, a severe (10mm) mandibular midline shift, and a crossbite of the upper left incisors, canine, and first premolar (Fig. 4A). The diagnosis was asymmetry due to occlusal interference.

Fig. 3 Multiple, diffuse marks on biteplane indicate patient needs further deprogramming.
An attempt to record centric relation failed to elicit a functional shift, suggesting a true skeletal asymmetry that would require surgical intervention. Nevertheless, the presence of wear facets in the dentition prompted us to prescribe a deprogrammer.
After one week of deprogramming, the midline deviation had been reduced to 3mm, and the crossbite was completely eliminated. The anterior bite had opened, with contact only on the upper right lateral incisor, canine, and first premolar and the upper left canine (Fig. 4B).

Fig. 4 A. 25-year-old male patient with facial asymmetry and severe midline deviation before treatment. B. Significant reduction in asymmetry and midline deviation after one week of deprogrammer wear.
The ability to record an accurate centric relation allowed us to prescribe orthodontics-only treatment for a patient who initially appeared to need orthognathic surgery.
Conclusion
Our design has several advantages over conventional Hawley-style appliances:
- With no wire bending, it is easier to fabricate.
- Better comfort and esthetics promote patient compliance.
- Undesirable tooth movement is avoided in cases where extended wear of the deprogrammer is required.
FOOTNOTES
- *Registered trademark of Dentsply Raintree Essix Glenroe, Sarasota, FL; www.essix.com.
REFERENCES
- 1. McHorris, W.M.: Occlusion with particular emphasis on the functional role of anterior teeth: Part 1, J. Clin. Orthod. 13:606-620, 1979.
- 2. Dawson, P.E.: Optimum TMJ condyle in clinical practice, Int. J. Period. Restor. Dent. 5:10-31, 1985.
- 3. Williamson, E.H.; Evans, D.L.; Barton, W.A.; and Williams, B.H.: The effect of bite plane use on terminal hinge axis location, Angle Orthod. 47:25-33, 1977.
- 4. Wood, D.P.; Floreani, K.J.; Galil, K.A.; and Teleruck, W.R.: The effect of incisor bite force on condylar seating, Angle Orthod. 64:53-61, 1994.
- 5. Jayne, D.: A deprogrammer for occlusal analysis and simplified accurate case mounting, J. Cosmet. Dent. 21:96-102, 2006.
-
 DR. KONTHAM
DR. KONTHAM -
 DR. KONTHAM
DR. KONTHAM
Dr. Rakesh Kontham is an Associate Professor, Department of Orthodontics, Nair Hospital Dental College, Mumbai 400008, India; e-mail: rakeshkontham4973@gmail.com. Dr. Ujwal Kontham is a Professor, Department of Pediatric Dentistry, Dr. D.Y. Patil Dental College and Hospital, Pune, Maharashtra, India.