2007 JCO Orthodontic Practice Study, Part 2: Practice Success
Last month, in the first of this series of articles on the 2007 JCO Orthodontic Practice Study, we discussed trends in the economics and administration of orthodontic offices since the initial biennial survey was conducted in 1981, and we covered the methodology of these reports (JCO, October 2007). For the complete tables of the 2007 Study, click here.
This month, we will describe factors that seem to be related to practice success in terms of net income and numbers of case starts. Because means are required for tests of statistical significance, most of the tables in this article report means instead of medians, which are used elsewhere in the Practice Study. We have selected the significance level ("p") of .01 rather than the more customary .05, since the large number of variables in this survey increases the likelihood of chance affecting the data.
In these tables, annual figures such as income and numbers of cases refer to the preceding calendar year, which, in the case of the present Study, was 2006. Every practice in this report had a single orthodontist-owner, because practices with multiple owners were excluded from the main survey results.
Similar articles from the archive:
Net Income Level
The respondents were arbitrarily divided into three net income categories, as in every previous Practice Study, so that we could pinpoint differences for purposes of comparison. To keep about one-fourth of the respondents in each group, the income levels used were slightly higher than in the 2005 Study: high ($600,000 or more), moderate ($325,000-525,000), and low ($25,000-250,000). The remaining one-fourth of the respondents were omitted from these particular tables.
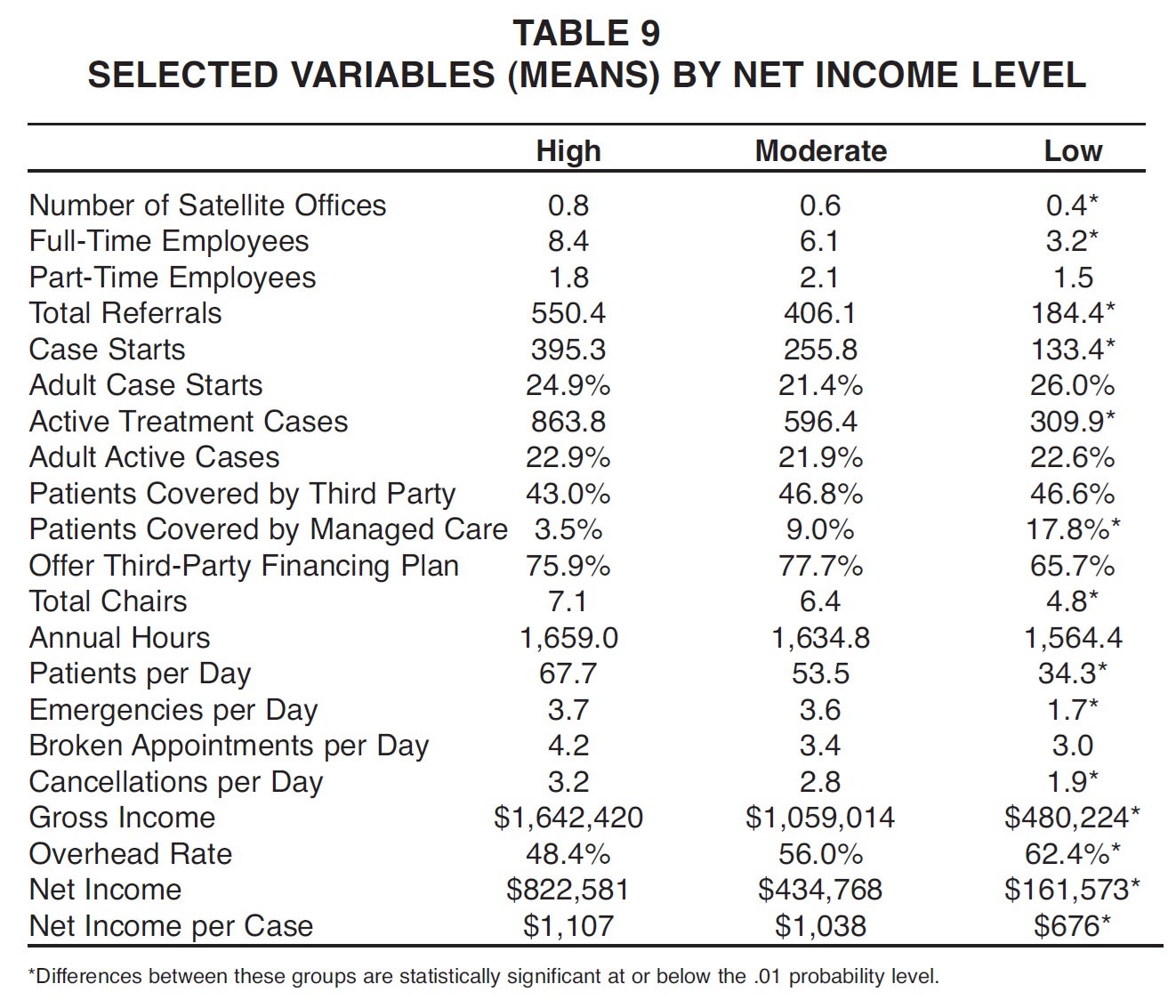
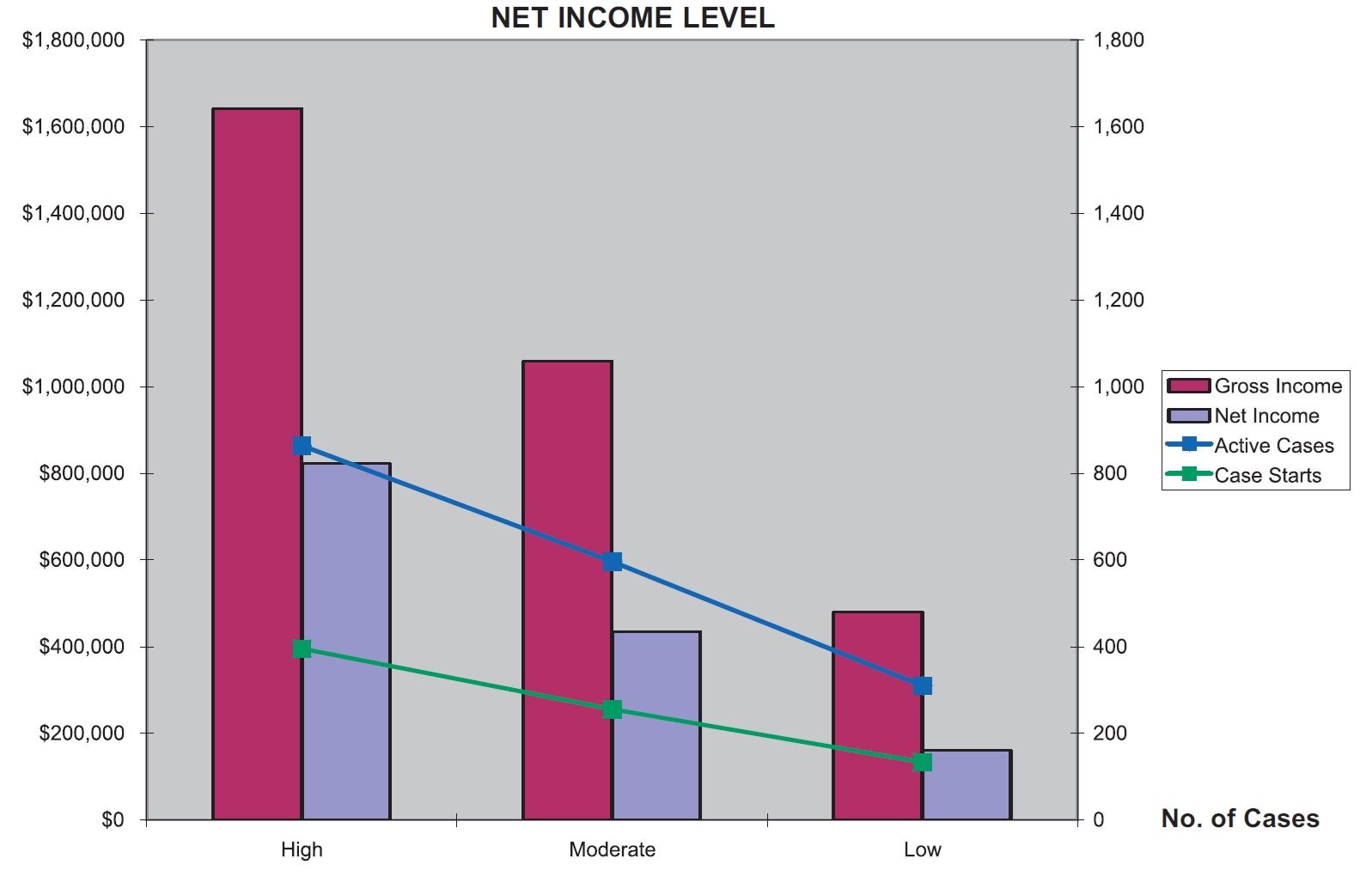
As in previous surveys, high net income practices were able to treat nearly three times as many active patients as low net income practices did, while taking in nearly twice the amount of net income per case (Table 9, Graph 4). High net income practices reported more than twice the number of employees, but significantly lower overhead rates--48% vs. 62%. There were no significant differences among the three groups in their percentages of adult and third-party patients, but low net income practices had significantly higher percentages of patients covered by managed care.
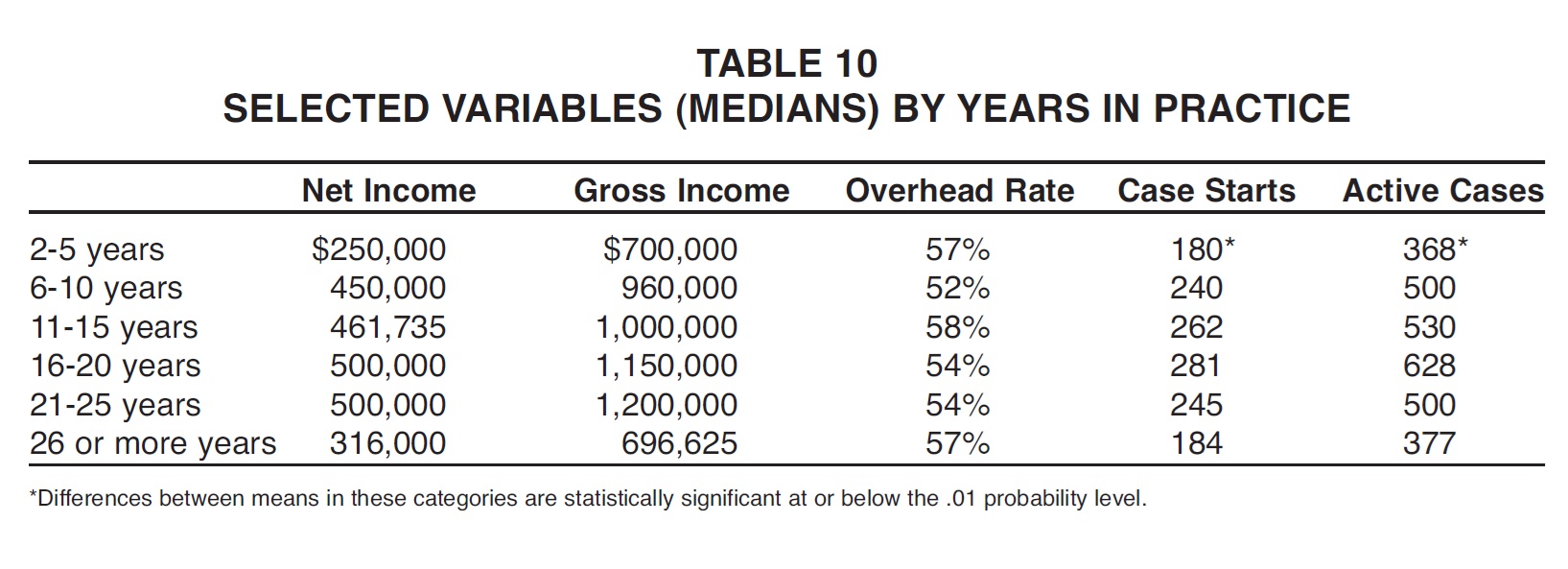
The most productive respondents were those who had been in practice between 16 and 25 years, although the 6-to-10-year group reported the lowest median overhead rate (Table 10). The newest and oldest practices, which make up disproportionately high percentages of the low net income category, tended to have the highest overhead rates.
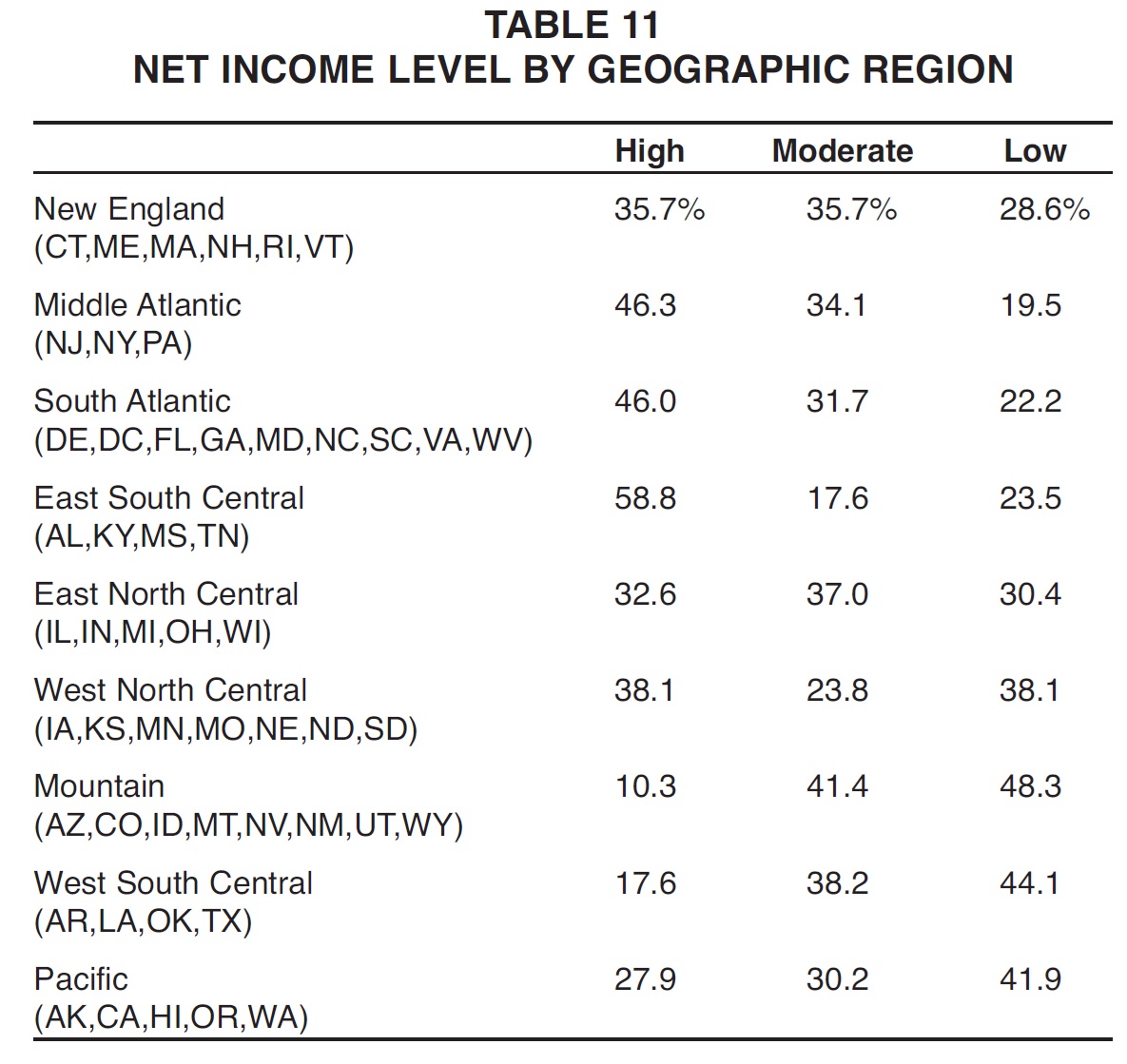
As in the 2005 Study, the highest percentage of respondents in the high net income group was found in the East South Central region (Table 11). The lowest percentage of high net income practices was in the Mountain region, followed by the West South Central region. The lowest percentages of low net income respondents were in the Middle Atlantic, South Atlantic, and East South Central regions.
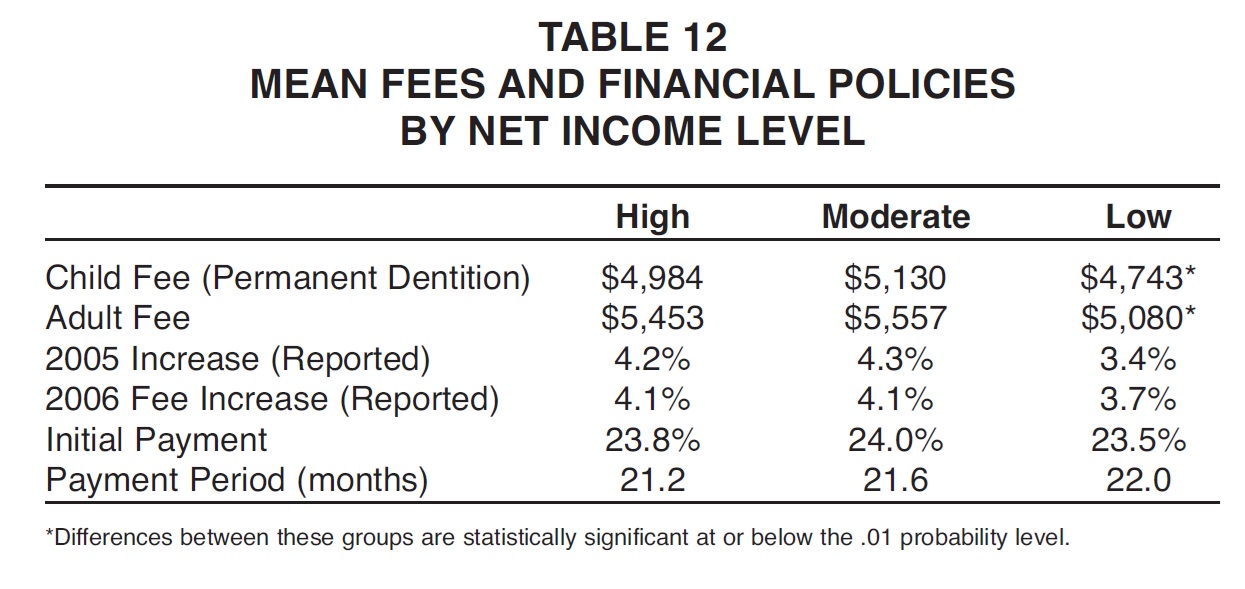
The high net income practices showed significantly higher fees than the low net income practices did, but the moderate group reported the highest fees (Table 12). High and moderate net income practices also had slightly higher fee increases and initial payments and shorter payment periods than the low net income practices, although the differences were not statistically significant.
Management Methods
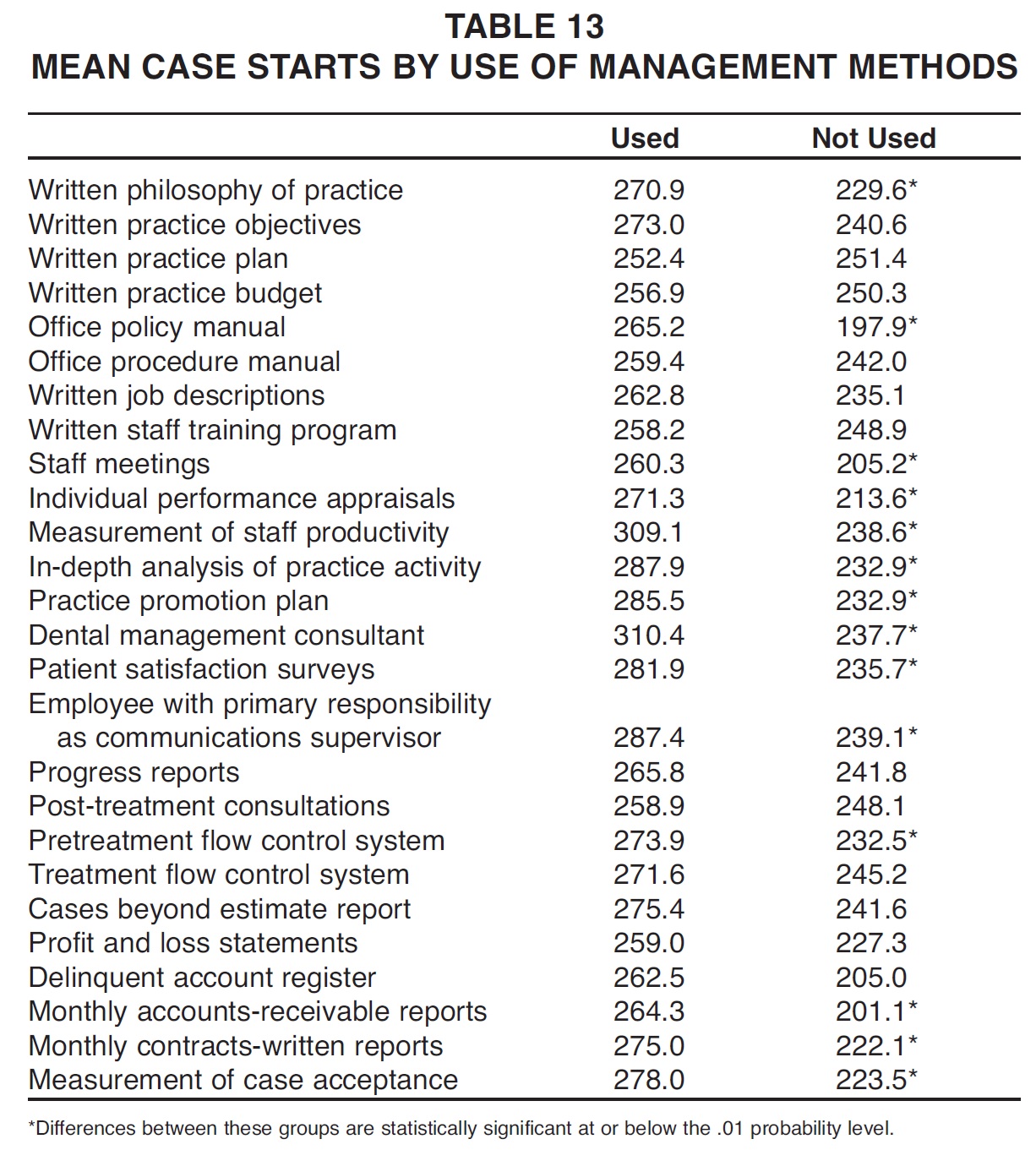
More than half the management methods surveyed were associated with significantly greater mean numbers of case starts for users than for non-users (Table 13). Although the differences were not statistically significant for the remaining methods, users still reported more case starts than non-users did in every category.
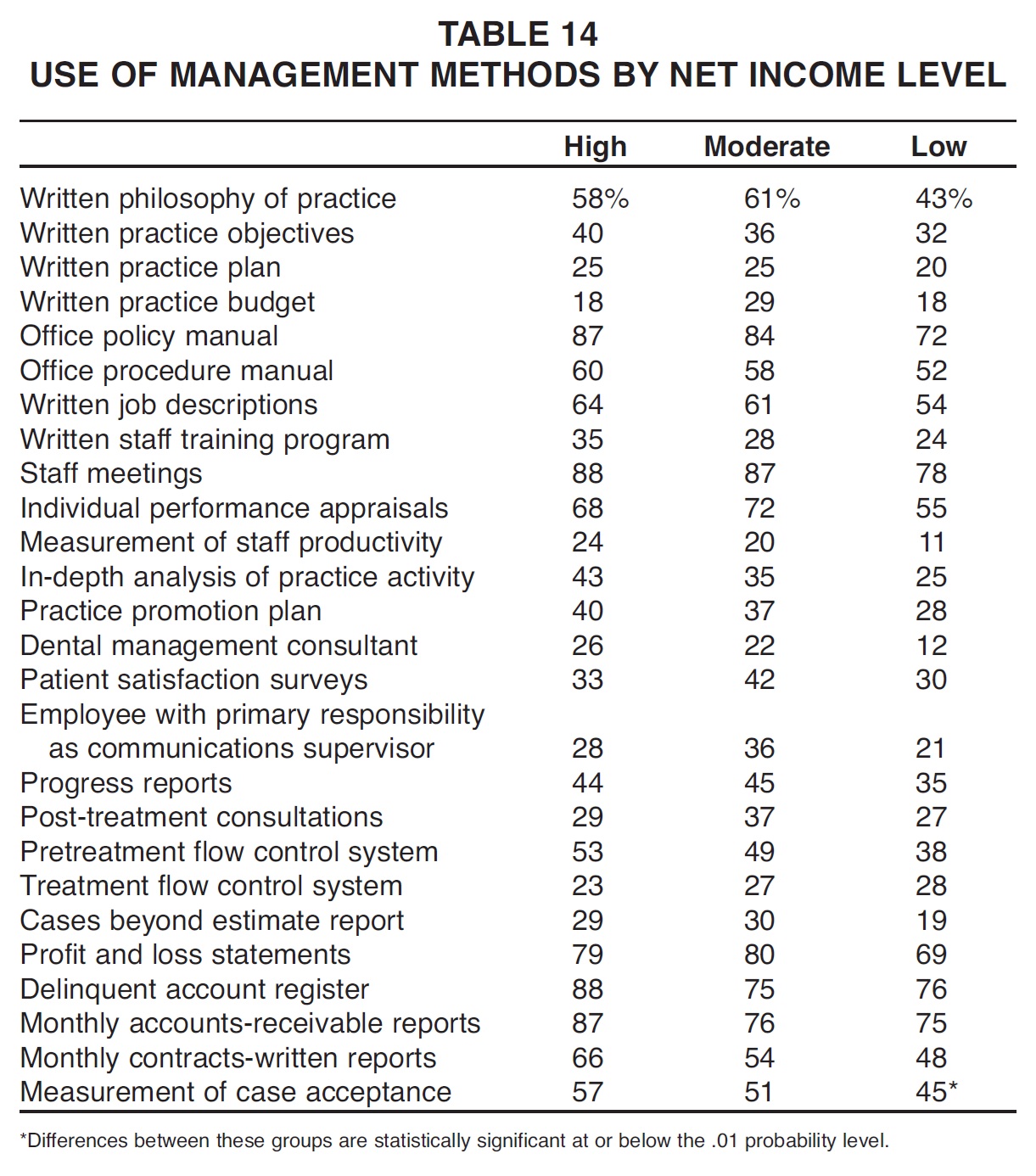
The use of management methods varied less according to net income level than in any Practice Study to date, with only the measurement of case acceptance showing a statistically significant difference among the three income groups (Table 14). The other management methods that were used more by the high net income respondents than by the practices in the moderate and low net income groups were written practice objectives, office policy manual, office procedure manual, written job descriptions, written staff training program, staff meetings, measurement of staff productivity, in-depth analysis of practice activity, practice promotion plan, dental management consultant, pretreatment flow control system, delinquent account register, monthly accounts-receivable reports, and monthly contracts-written reports.
Delegation
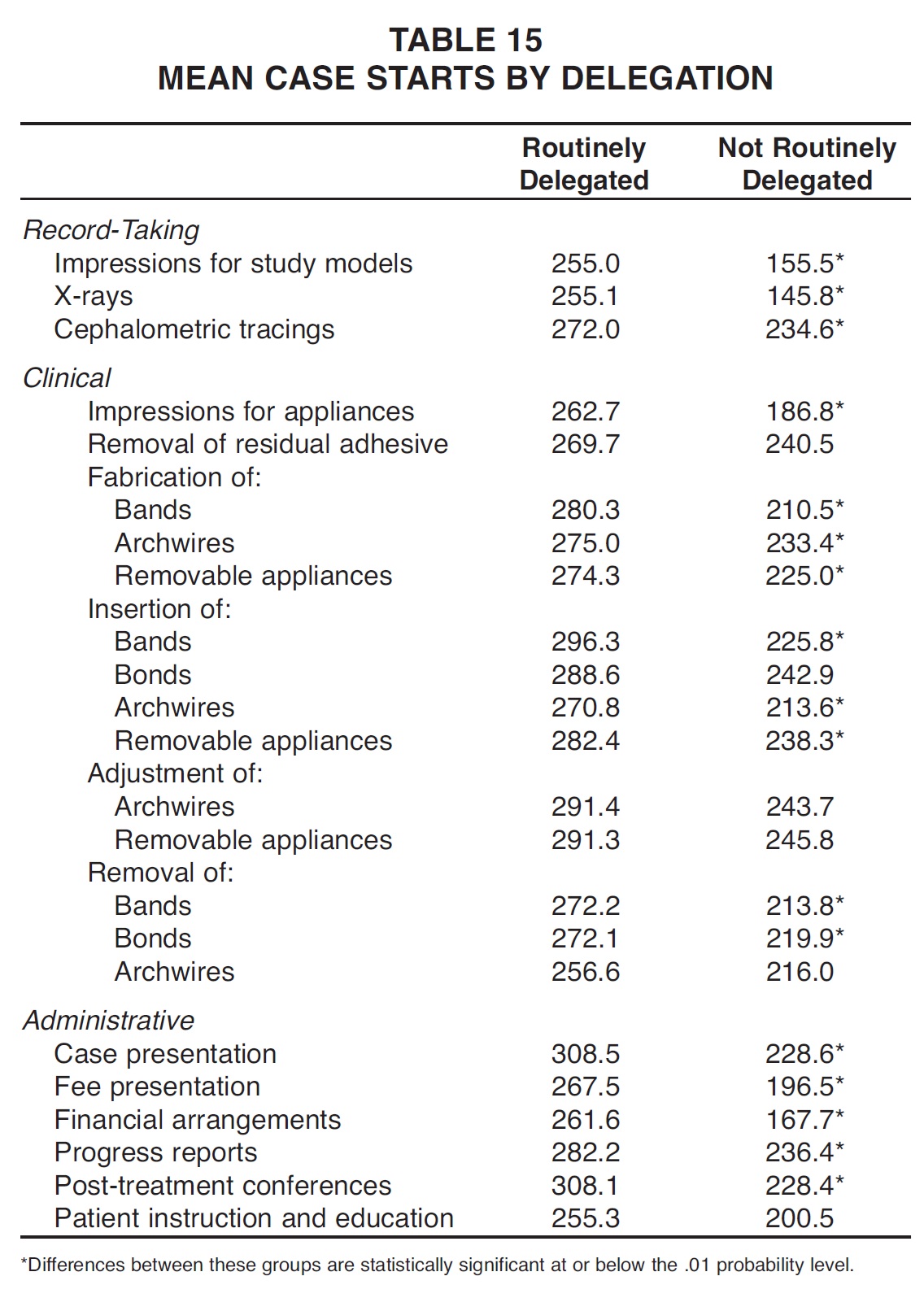
Routine delegation, as opposed to delegating occasionally or not at all, was associated with greater mean numbers of case starts for every task listed, as in previous surveys (Table 15). The differences were statistically significant for every task except removal of residual adhesive, insertion of bonds, adjustment of archwires and removable appliances, removal of archwires, and patient instruction and education.
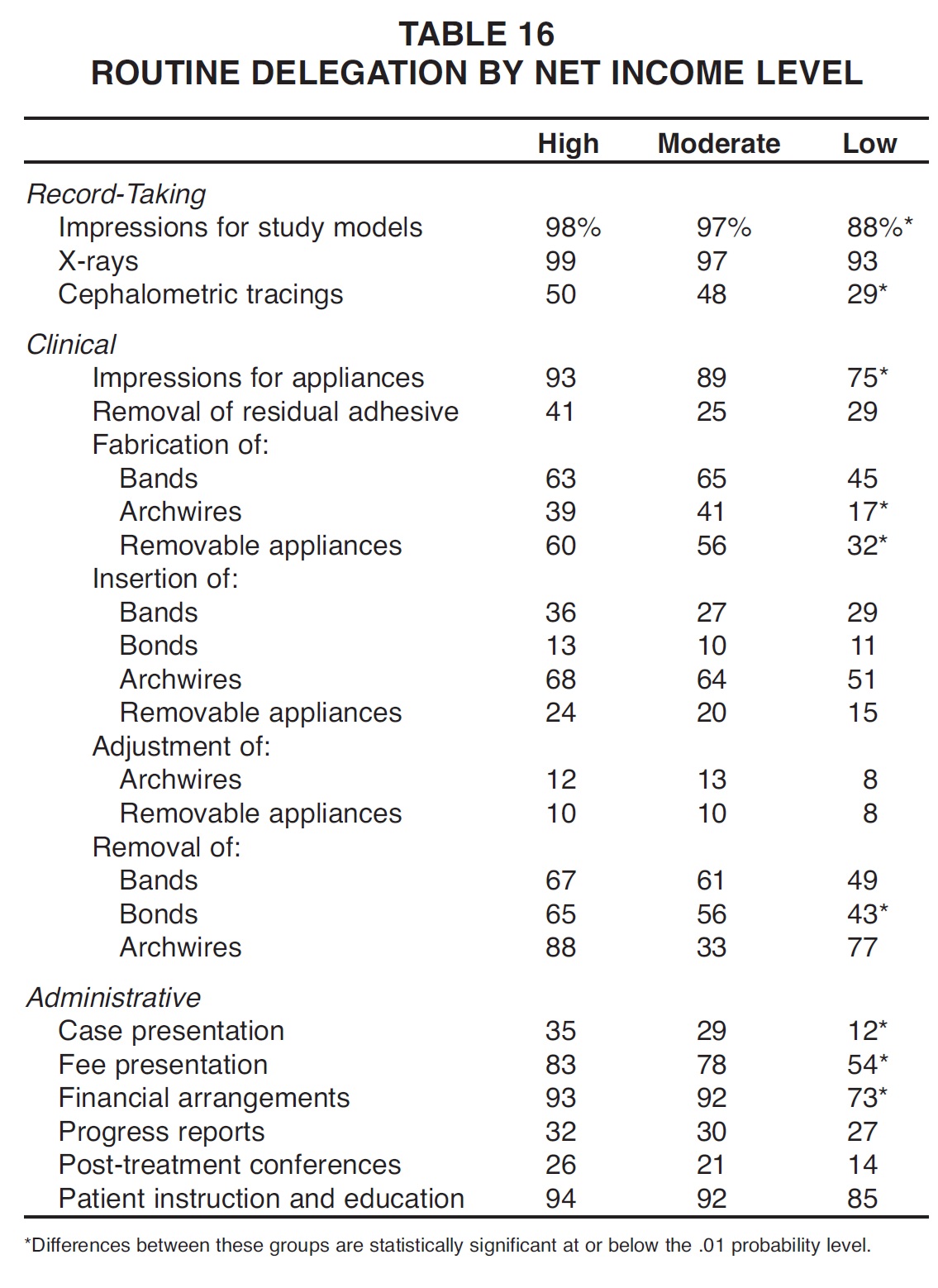
High net income practices delegated every task more routinely than moderate or low net income practices did, except for the fabrication of bands and archwires and the adjustment of archwires and removable appliances, which were routinely delegated as much or more by the moderate net income group (Table 16). Differences among the three net income categories were statistically significant in the cases of impressions for study models, cephalometric tracings, impressions for appliances, fabrication of archwires and removable appliances, removal of bonds, case presentation, fee presentation, and financial arrangements.
Practice-Building Methods
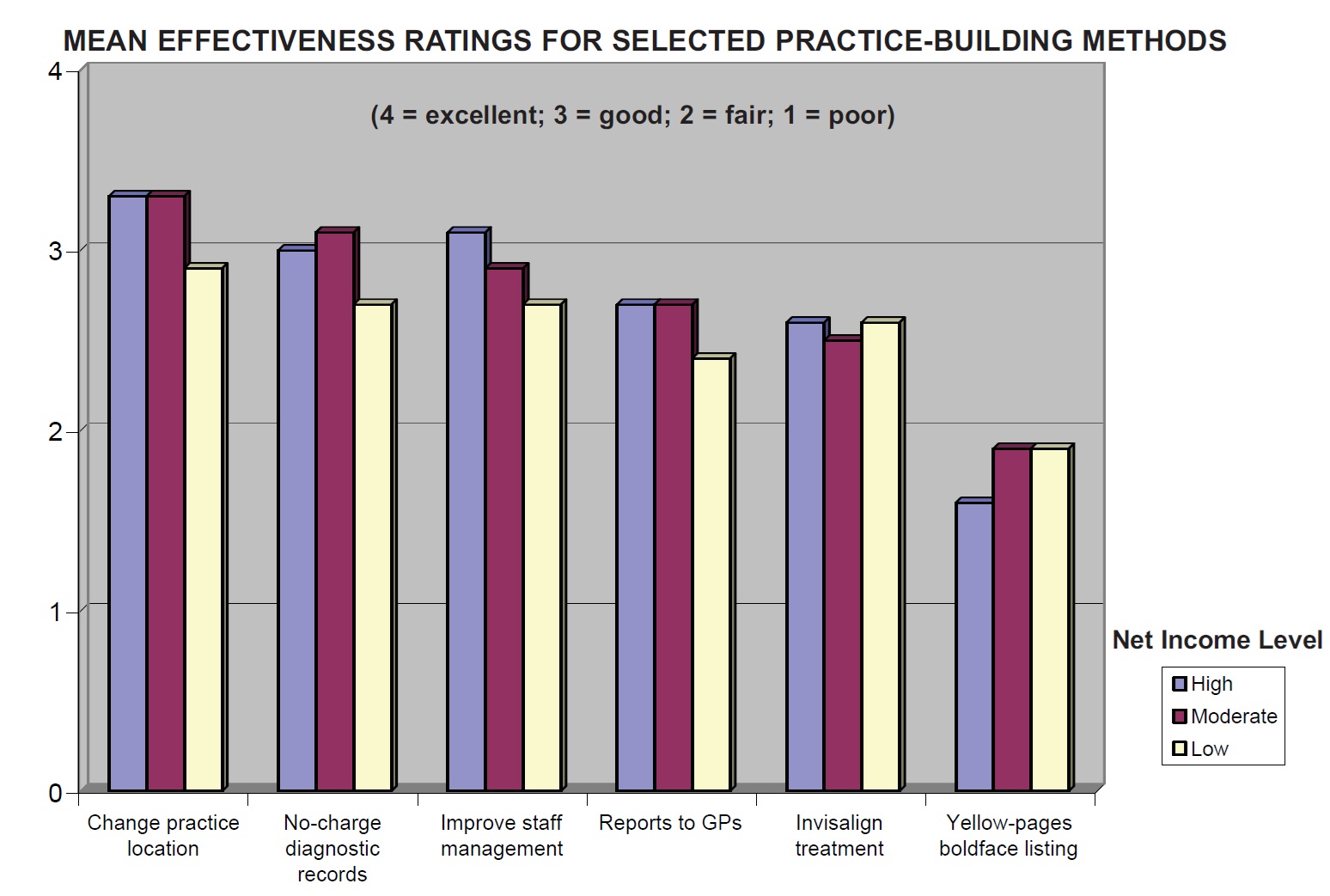
As has been true since the early 1990s, there was no significant association between the use of practice-building methods and net income level (Table 17, Graph 5). Still, the most effective methods might be considered those rated good (3.0) or better by the high net income practices. In the current Study, these methods were (from highest to lowest ratings): change practice location, open a satellite office, on time for appointments, improve case presentation, follow-up calls after difficult appointments, on time case finishing, improve staff management, no-charge initial visit, and no-charge diagnostic records. Expanding practice hours by opening on evenings or Saturdays now seems to be more popular among low net income practices than among other respondents.
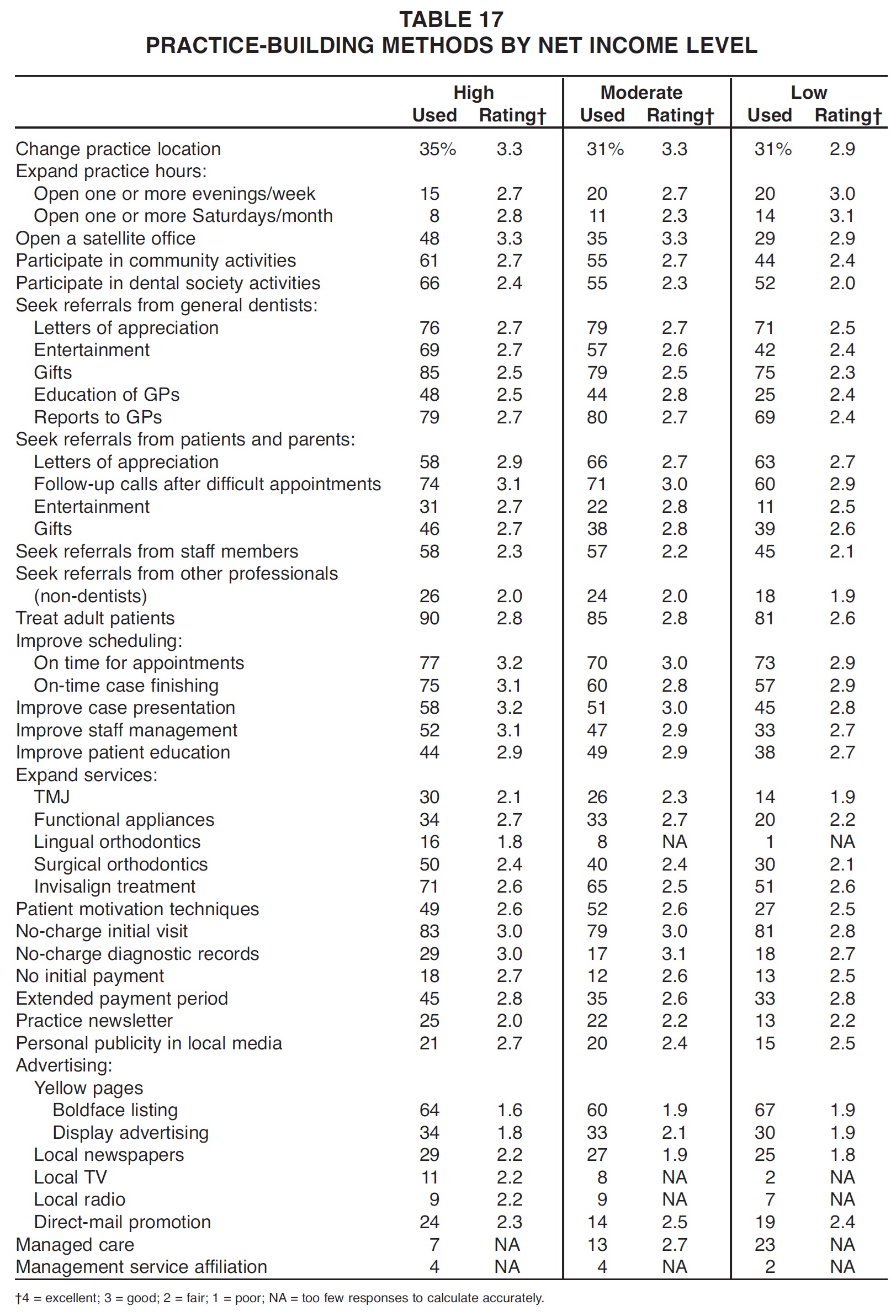
The practice-building methods used by more than 70% of the high net income practices were (in descending order of usage): treat adult patients, gifts to GPs, no-charge initial visit, reports to GPs, on time for appointments, letters of appreciation to GPs, on-time case finishing, follow-up calls after difficult appointments, and Invisalign treatment.
The practice-building methods rated fair (2.0) or worse by the practices with high net income were (from lowest to highest ratings): yellow-pages advertising, lingual orthodontics, seek referrals from other professionals, and practice newsletter.
-
 DR. KEIM
DR. KEIM -
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Keim is Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302.
Dr. Gottlieb is Senior Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302.
Dr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.
Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302.
