An Alternative Method of Space Closure: The Hycon Device
In the standard edgewise technique, space closure is usually performed with closing-loop arches rather than sliding mechanics. This is primarily because of the friction created by 1st-, 2nd-, and 3rd-order bends when sliding mechanics is attempted. With a closing-loop arch, the friction in the system is overcome by activating the loops--usually only about 1mm at a time, which allows the roots to "catch up" to the initial tipping effect of the activation.
A number of variables must be considered when using closing-loop mechanics, including bracket slot size, wire size, loop design, and the amount and frequency of loop activation. As a result, when preadjusted appliances became available, many orthodontists began to use sliding mechanics as their primary method of space closure. Various force systems, such as Pletcher coil springs, elastic chains, elastic modules, and nickel titanium springs, have been used effectively.1,2
Still, there are cases where space closure is problematic because of excessive friction, increased bone density, or narrowing of the alveolar process in the extraction sites.
The Hycon Device for Space Closure in Difficult Cases
Similar articles from the archive:
- Extraction Space Closure with Vacuum-Formed Splints and Miniscrew Anchorage February 2005
- Use of Bonded Power Arms for Interdental Space Closure September 2001
- A Sliding Bridge Appliance for Space Closure February 1991
A new device for extraction space closure was developed in Germany in the 1980s.3 In the original design, a small screw was connected to the first molars and to the anterior segment. The most recent version, now called the Hycon Device*, uses a rectangular support wire that is inserted into an auxiliary tube of the double or triple first molar tubes (Fig. 1). A bolt-and-nut assembly is soldered buccally to this rectangular wire; a ligature wire is tied to the end of the bolt, and the opposing end of the wire is tied to the anterior segment. The patient is instructed to turn the bolt for space closure. The Hycon Device is compatible with all common fixed appliances.

Fig. 1 Hycon Device.
Unlike closing loops and sliding mechanics, which rely on elastic forces, the Hycon Device is based on a design that has been used successfully since the early days of orthodontics--a screw-type mechanism. Liou and Huang,4 Sayin and colleagues,5 and Iseri and colleagues6 have used similar appliances to retract canines, referring to this movement as "distraction" of the periodontal ligament. With the Hycon Device, a single 360° turn of the screw provides an activation length of .35mm (Fig. 2), as tested with a profile projector at 50× magnification.7 This makes it possible to deliver a precise space-closing activation at a relatively high force level, but over a short distance. The force generated by a single activation was measured at 410g in a strength-testing machine**.
The screw mechanism is actually easier to control than conventional methods of space closure. With elastic forces, the orthodontist is constantly trying to manage the amount of force, the length of force application, the degree of archwire deflection, and the amount of friction. With the Hycon Device, the amount of tooth movement is determined strictly by the advancement rate of the bolt and the number of activation turns. Friction is of little concern because of the relatively high forces generated. Deflection is not a problem because the activation is over such a short distance. A full-size wire can be used, reducing deflection and improving torque control.
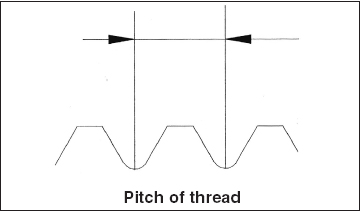
Fig. 2 Hycon thread measures 1.7mm × .35mm, with pitch of .35mm.
This technique minimizes tissue turnover, producing nearly ideal bodily movement. The force created by turning the screw is enough to overcome friction, but less than the amount that would adversely affect the periodontium. When the screw is activated, space closure typically occurs anterior and posterior to the periodontal space, which has been measured at .25mm ± 50%.8 If one 360° turn produces .35mm of activation, the activation for each tooth is about .175mm, less than the periodontal space. In maximum anchorage situations, where one segment needs to be held in place, a half-turn (180°) will permit adequate stimulation of tissue response, while ensuring a continuous blood supply to the periodontium and the surrounding structures. This is an optimal situation for the metabolism and subsequent osteoclast and osteoblast activity.
Placement Procedure
Space closure is initiated after leveling and alignment have been completed and rectangular archwires have been placed. Traditional methods can be used first, or the Hycon Device can be employed at the beginning of space closure. Prior to its insertion in the mouth, a soft ligature wire is twisted around the neck of the bolt and bent 90°. We recommend leaving some slack in this ligature to prevent binding during activation. The assembly is then installed by inserting the rectangular support wire into the auxiliary molar tube from the mesial side (Fig. 3). It is secured by bending back the end of the support wire that extends distally from the auxiliary tube. The ligature wire that was initially twisted around the neck of the bolt is then connected on the mesial side of the extraction space to a bracket hook or Kobayashi hook to move a single tooth, or to an anterior archwire hook to move an entire segment. In functional terms, it has now become the connecting wire.
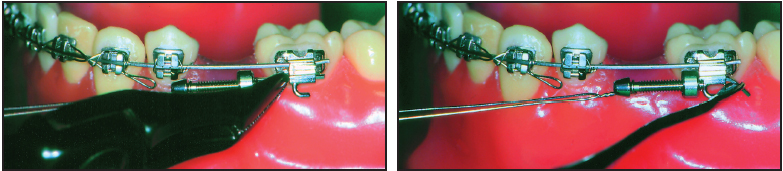
Fig. 3 Placement of Hycon Device.
Using a small screwdriver, the patient preactivates the appliance by turning the bolt clockwise until the slack is taken out of the connecting wire and the patient begins to feel a slight tension. From this point, the patient activates the appliance with one full 360° turn in the same direction. This will close the space a maximum of .35mm; if there is any slack remaining in the wire from the preactivation, the amount of activation will be reduced accordingly.
As a general rule, the Hycon Device can be reactivated one full turn twice a week. This will provide approximately 1-2mm of space closure per month, which is similar to the amount that can be achieved with elastic forces. Pain-free function is the clinical indicator that the Hycon is activated within the physiologic range. The only sensation felt by the patient should be one of pressure. If pain occurs, then a half-turn activation may be indicated. Patients with periodontally involved teeth should certainly activate the device more slowly than usual. If any activation creates too much pressure, the patient can reduce it by turning back the bolt. This has proven to be a good clinical guide to activation over the 15 years that the device has been in use.
Anchorage control must be carefully considered. As with all space-closure methods, the Hycon Device does not discriminate. It pulls from both ends, and the weakest attached units tend to move the most. This device is particularly sensitive in that regard, because friction will not reduce the impact of improper anchorage control.
Bone Remodeling
The short-acting but relatively high forces generated by the Hycon Device are quite different from those generated by either closing-loop arches or sliding mechanics. More than 1,000 patients have been treated with the Hycon to date, however, and root resorption has been observed in fewer than 2% of the cases--primarily on the upper lateral incisors. In short, the use of the Hycon Device does not seem to cause root resorption.
Radiovisiographic images of the periodontal ligament space mesial to the canines, taken with an UltraCam***, show a uniform pattern of periodontal space compression and a distal stretching of the PDL, with minimal tipping (Fig. 4). Image inversion with Dexis† 3.0 software makes this change in the PDL space easier to visualize. It appears that the ability of the Hycon Device to overcome friction while preventing tipping leads to a uniform stress and strain distribution in the PDL and adjacent alveolar bone, eliciting a favorable catabolic/anabolic remodeling response.
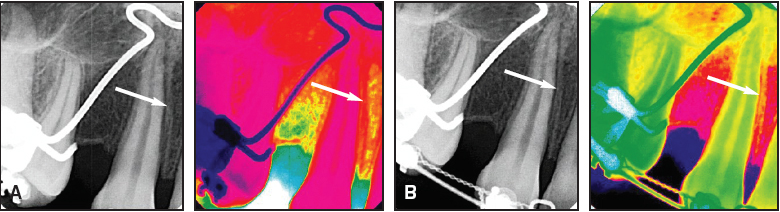
Fig. 4 Radiovisiographic images of periodontal ligament space (arrows). A. Before activation of Hycon Device. B. Three weeks later, after second activation.
In a pilot study, an active tieback (a typical technique used in sliding mechanics) produced an increase of as much as 100 international units of alkaline phosphatase9-11 in the gingival crevicular fluid on the mesial aspect of the canines after a three-week period of standard activation. After a similar three-week period of activation with the Hycon Device, there was a steady increase in the alkaline phosphatase level from a baseline of 60 international units to a peak of 160 international units (Fig. 5). This seems to indicate that the Hycon Device has a more favorable bone remodeling response than is seen in traditional sliding mechanics.
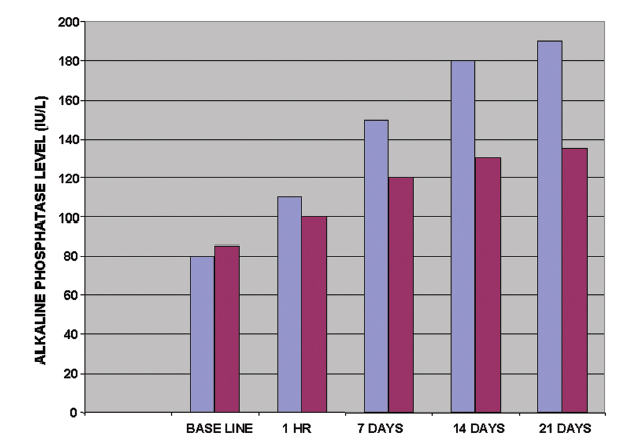
Fig. 5 Alkaline phosphatase levels in gingival crevicular fluid on mesial aspect of canines, after three-week activations of tiebacks for sliding mechanics (red) and Hycon Device (blue).
Case 1
A 30-year-old male presented with a Class I occlusion, a moderate Class II skeletal pattern, and severe lower anterior crowding (Fig. 6).
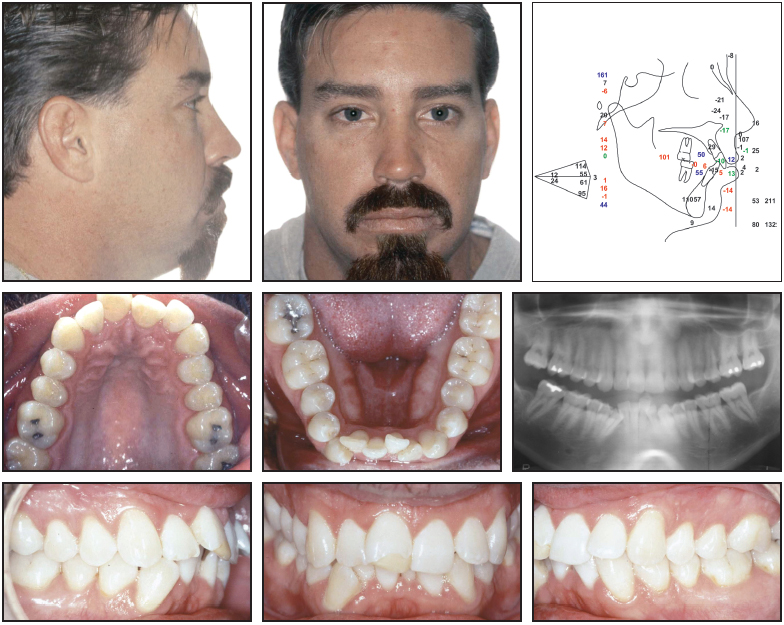
Fig. 6 Case 1. 30-year-old male patient with Class I occlusion, moderate Class II skeletal pattern, and severe lower anterior crowding before treatment.
Four first bicuspids were extracted. Space closure occurred routinely in the lower arch, but was slow in the upper arch. Upper Hycon Devices were placed (Fig. 7) to complete space closure efficiently (Figs. 8A and 8B).

Fig. 7 Case 1. Upper space closure with Hycon Devices.
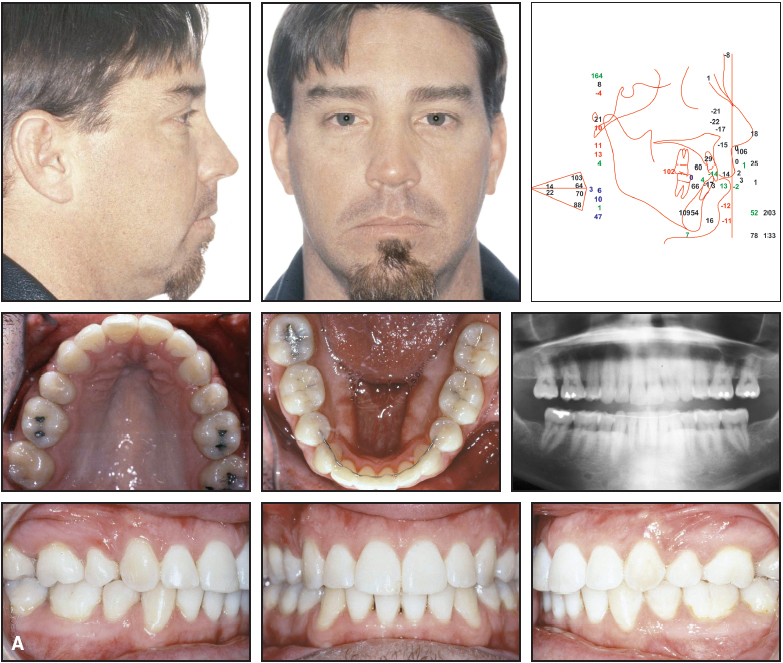
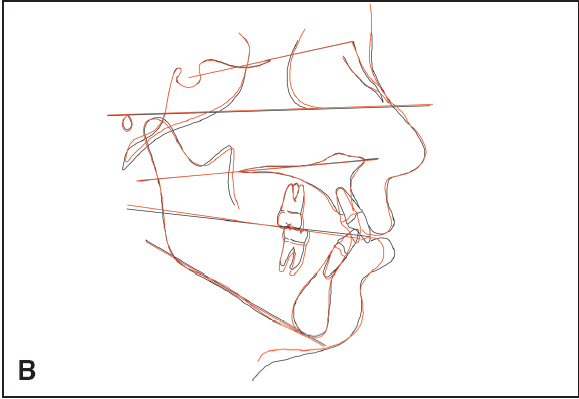
Fig. 8 Case 1. A. Patient after treatment. B. Superimposition of cephalometric tracings before (black) and after (red) treatment.
Case 2
This 17-year-old female displayed a Class I dental and skeletal pattern and a satisfactory profile, with moderate crowding in both arches (Fig. 9).

Fig. 9 Case 2. 17-year-old female patient with Class I dental and skeletal pattern before treatment.
Her lower first molars had large restorations, and the lower right first molar had developed a periapical abscess. Upper first bicuspids and lower first molars were extracted. The upper spaces were closed with normal sliding mechanics, while the lower spaces were closed with Hycon Devices (Fig. 10).
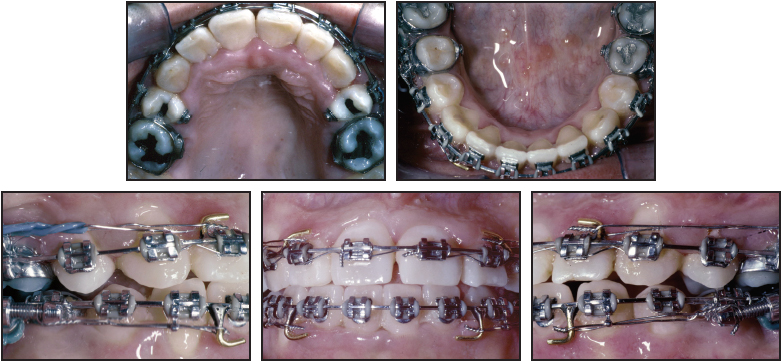
Fig. 10 Case 2. Lower space closure with Hycon Devices.
An .021" × .025" stainless steel lower archwire was used to avoid any deepening of the curve of Spee during space closure (Figs. 11A and 11B). (This case was treated at the University of Southern California by Dr. Steven Olsburgh, under the supervision of Dr. McLaughlin.)
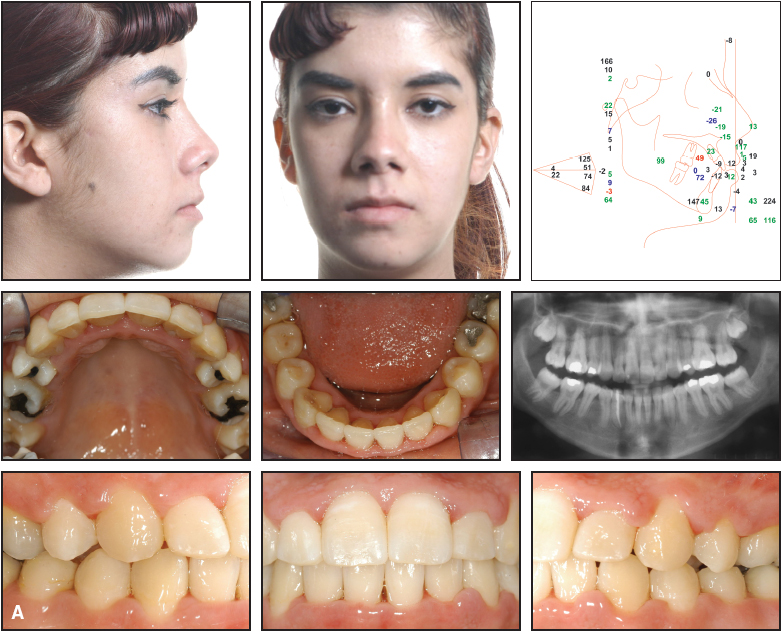
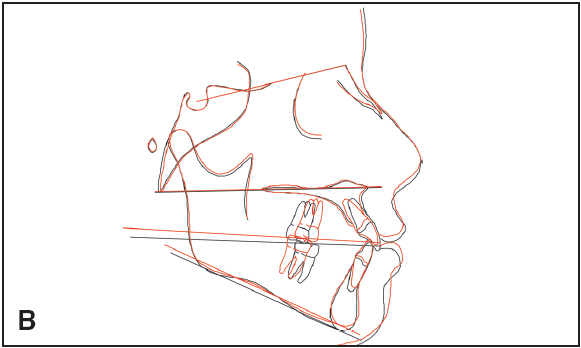
Fig. 11 Case 2. A. Patient after treatment. B. Superimposition of cephalometric tracings before (black) and after (red) treatment.
Case 3
A 22-year-old male presented with a Class I dental and skeletal pattern, a satisfactory profile, and congenitally missing upper lateral incisors (Fig. 12).
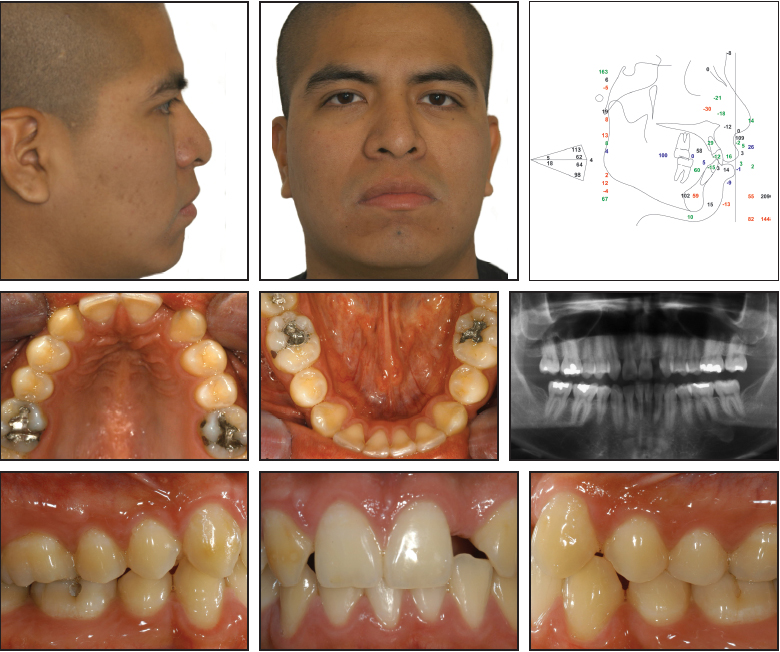
Fig. 12 Case 3. 22-year-old male patient with Class I dental and skeletal pattern and congenitally missing upper lateral incisors before treatment.
He had previously been treated orthodontically with extraction of the lower second bicuspids, but the upper space closure had not been completed. Hycon Devices were placed (Fig. 13) to close these remaining spaces (Figs.14 A and 14B). (This case was treated at the University of Southern California by Dr. Mark Fagin, under the supervision of Dr. McLaughlin.)
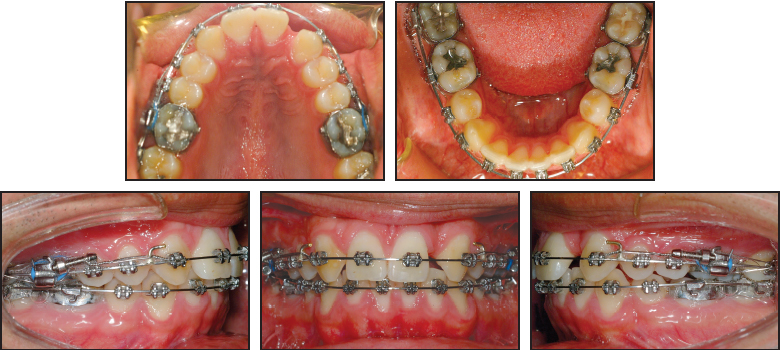
Fig. 13 Case 3. Completion of upper space closure with Hycon Devices.
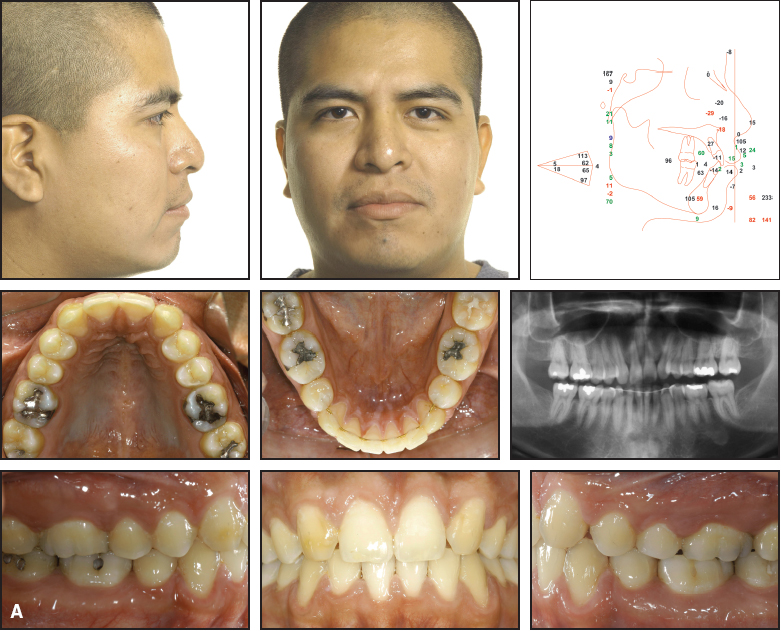
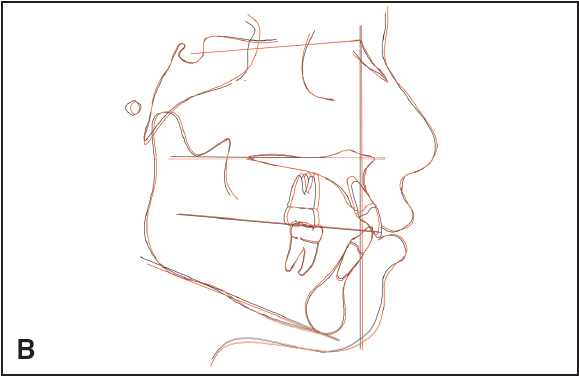
Fig. 14 Case 3. A. Patient after space closure. B. Superimposition of cephalometric tracings before (black) and after (red) treatment.
FOOTNOTES
- *Registered trademark of Adenta USA, 81 Clover Road, Ivyland, PA 18974.
- **Hounsfield Universal Strength Testing Machine, Hounsfield Test Equipment Ltd., Salfords, Surrey, UK.
- ***Registered trademark of American Medical Technologies, Inc., 5655 Bear Lane, Corpus Christi, TX 78405.
REFERENCES
- 1. Bennett, J.C. and McLaughlin, R.P.: Orthodontic Treatment Mechanics and the Preadjusted Appliance, Mosby, London, 1993.
- 2. McLaughlin, R.P.; Bennett, J.C.; and Trevisi, H.J.: Systemized Orthodontic Treatment Mechanics, Mosby, Edinburgh, Scotland, 2001.
- 3. Schuetz,W.: Edgewisetechnik mit Schraube—ein Hybrid in der Kieferorthopaedie, Inform. Orthod. Kieferorthop. 5:351-362, 1983.
- 4. Liou, E.J.W. and Huang, C.S.: Rapid canine retraction through distraction of the periodontal ligament, Am. J. Orthod. 114:372-381, 1998.
- 5. Sayin, S.; Bengi, A.O.; Gurton, A.U.; and Ortakoglu, K.: Rapid canine distalization using distraction of the periodontal ligament: A preliminary clinical validation of the original technique, Angle Orthod. 74:304-315, 2004.
- 6. Iseri, H.; Kisnisci, R.; Bzizi, N.; and Tuz, H.: Rapid canine retraction and orthodontic treatment with dentoalveolar distraction osteogenesis, Am. J. Orthod. 127:533-541, 2005.
- 7. Adenta Company, Gutenbergstr. 9-11, 82205 Gilching, Germany.
- 8. Lindhe, J.: Textbook of Clinical Periodontology, Munksgaard, Copenhagen, Denmark, 1988, pp. 19-66.
- 9. Keeling, S.D.; King, G.J.; McCoy, E.A.; and Valdez, M.: Serum and alveolar bone phosphatase changes reflect bone turnover during orthodontic tooth movement, Am. J. Orthod. 103:320-326, 1993.
- 10. Perinetti, G.; Paolantonio, M.; D’Attilio, M.; D’Archivio, D.; Tripodi, D.; Femminella, B.; Festa, F.; and Spoto, G.: Alkaline phosphatase activity in gingival crevicular fluid during human orthodontic tooth movement, Am. J. Orthod. 122:548-556, 2002.
- 11. Mao, J.J. and Nah, H.D.: Growth and development: Hereditary and mechanical modulations, Am. J. Orthod. 125:676-689, 2004.
-
 DR. MCLAUGHLIN
DR. MCLAUGHLIN -
 DR. KALHA
DR. KALHA -
 DR. SCHUETZ
DR. SCHUETZ
Dr. McLaughlin is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at 1831 Sunset Cliffs Blvd., San Diego, CA 92107. Dr. Kalha is Senior Professor and Head, Department of Orthodontics, College of Dental Sciences, Davangere, India; a Visiting Professor, University of Phnom Penh, Cambodia; and Director and Coordinator, Center for Evidence-Based Dentistry, Davangere, Karnataka, India. Dr. Schuetz is retired from the practice of orthodontics in Germany; he is the inventor of the Hycon Device and has a financial interest in the appliance.