The Butterfly System
In 1996, the American Board of Orthodontics listed the mistakes found most often in cases presented by candidates who failed the Phase III examination.1 These clinicians were presumably submitting their best work, which indicates that cases failing the examination might be representative of fairly prevalent errors in today's orthodontic practices. Since preadjusted brackets are currently the most commonly used fixed appliances, these cases might also point out some limitations of today's popular prescriptions.2-7
Andrews's original Straight-Wire Appliance* was intended to allow the clinician to complete treatment more efficiently and effectively, based in part on the shortcomings he had found in ideal, finished cases.8 Although many practitioners have modified Andrews's original prescription,2,3,5,6,9-11 analysis of the results achieved by these second-generation appliances indicates that further enhancements could be beneficial.
Creekmore and Kunik described five reasons why current preadjusted appliances do not achieve ideal tooth positions with the use of "straight" wires2:
- Inaccurate bracket placement.
- Variations in tooth structure.
- Variations in anteroposterior jaw relationships affecting incisor position.
- Lack of overcorrection built into treatment mechanics (i.e., tissue rebound).
- Mechanical deficiencies of the orthodontic appliance--force not applied at the center of resistance, play between wire and slot, or force diminution.
Similar articles from the archive:
If teeth were moved through air or the "virtual reality" of a computer simulation,11 the preadjusted prescription would always work. In reality, however, a straight wire never becomes entirely straight. Consequently, it is not enough simply to plan for ideal tooth positions; some overcompensation or overcorrection is needed in the prescription.12
The misconception that preadjusted appliances require no wire bending may contribute to some of the failures observed by the ABO. Superb results may be obtained with virtually any appliance or prescription if there is enough attention to detail and wire bending. Still, if bracket prescriptions were modified to account for common errors, perhaps the effectiveness and efficiency of these systems could be improved. That was the basis for developing a hybrid, third-generation appliance, as described in this article.13
Butterfly System
The Butterfly System** is based on a new low-profile, twin-wing bracket (Fig. 1). The bracket's reduced profile, its miniature twin-wing design and rounded tie wings, and the elimination of standard hooks results in an appliance that is more comfortable, esthetic, and hygienic.
The Butterfly System has several unique features designed to improve upon existing preadjusted appliance concepts, in response to the findings of the ABO. These are outlined below.
Versatile Vertical Slot
The incorporation of a simple vertical slot opens an entire new realm of treatment options (Fig. 2). First, the elimination of ball hooks on the brackets significantly reduces the likelihood of tissue impingement, trapped food, and plaque, while making archwires easier to tie. When elastics are needed, a simple hook pin or T-Pin*** can be inserted into the vertical slot of any bracket--virtually eliminating the need for Kobayashi ties, soldered hooks, and crimpable surgical hooks.
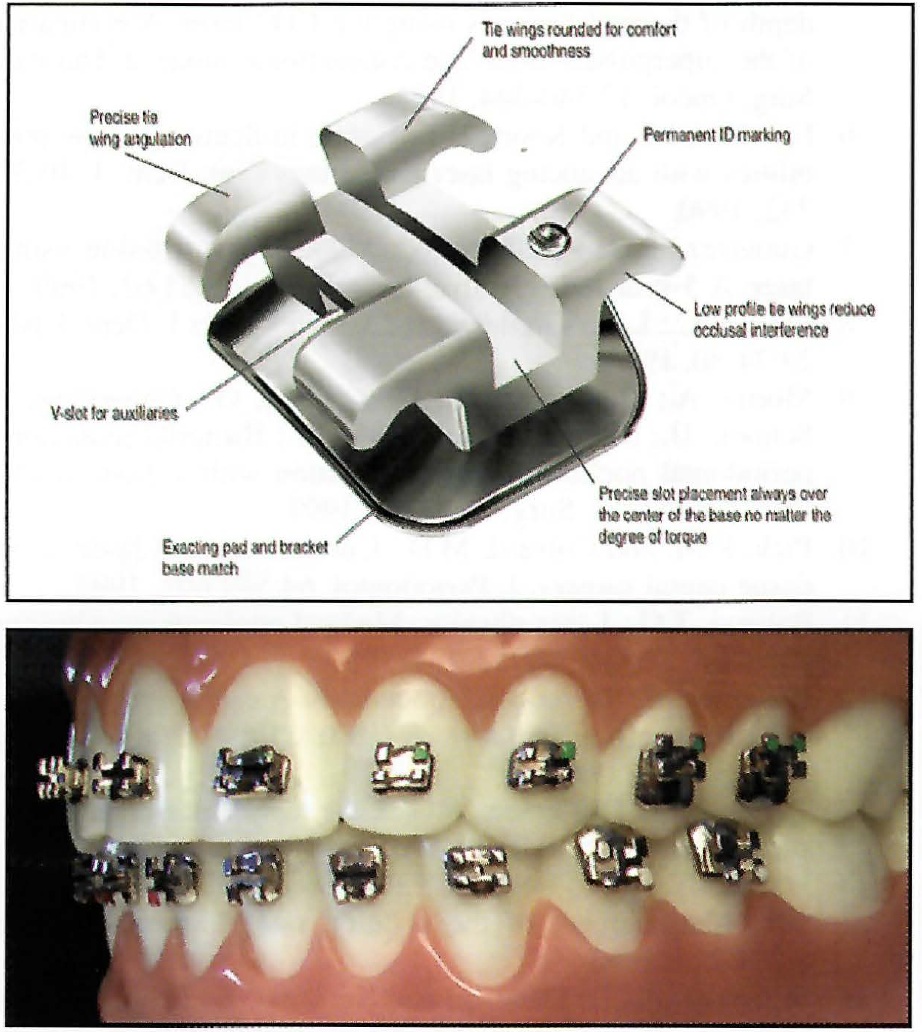
Fig. 1 Butterfly System features low-profile miniature bracket with vertical slot.
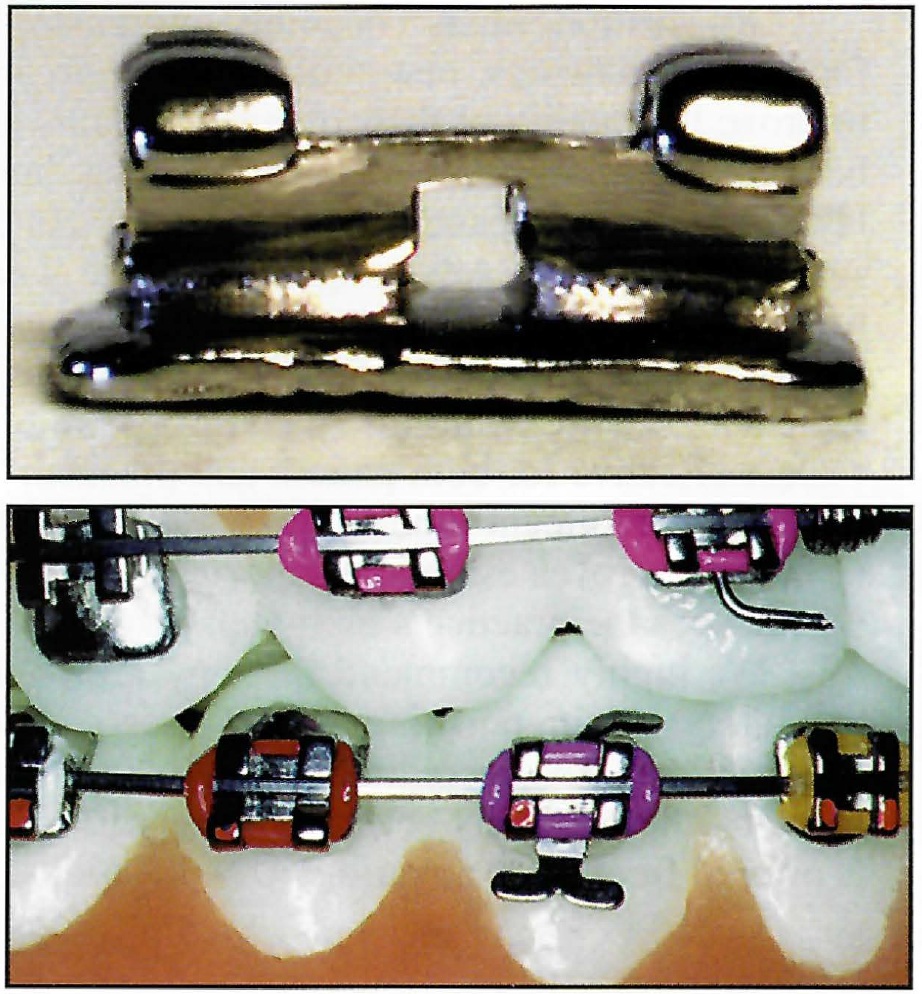
Fig. 2 Removable T-Pins or hook pins can be placed through vertical slots of any brackets when needed, eliminating integral bracket hooks.
One of the simplest uses of the vertical slot is for teeth that are blocked out, lingually displaced, or ectopically erupted. In these instances, it is nearly impossible to tie an archwire into the bracket during early alignment, but a stainless steel ligature or elastic thread can be placed through the vertical slot to form a vertical or "sling" tie around the archwire (Fig. 3). A loose stainless steel tie, especially a single vertical tie, produces even less friction than a self-ligating bracket.
A series of vertical-slot auxiliaries has also been developed. The U-Turn Rotating Spring**,a unique square-wire spring, can be inserted into the square vertical slot on any bracket to help correct severe rotations (Fig. 4). The universal, friction-fit U-Turn can be inserted from either the occlusal or the gingival for clockwise or counterclockwise rotations.
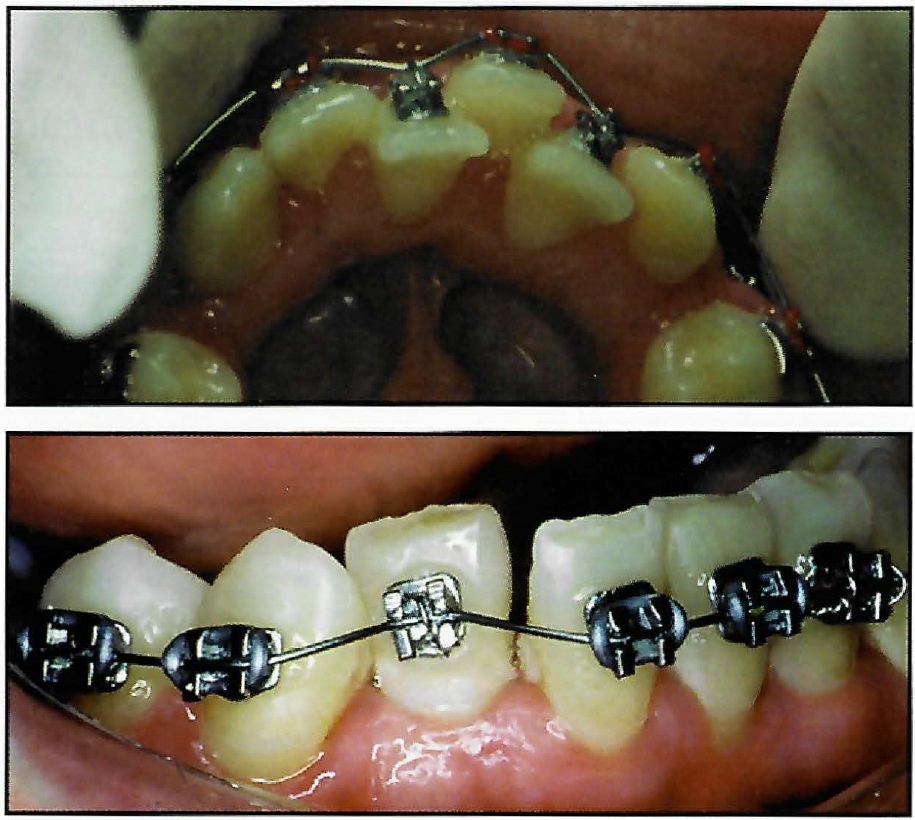
Fig. 3 Vertical or “sling” tie: stainless steel ligature placed through vertical slot and around archwire for severely displaced teeth.
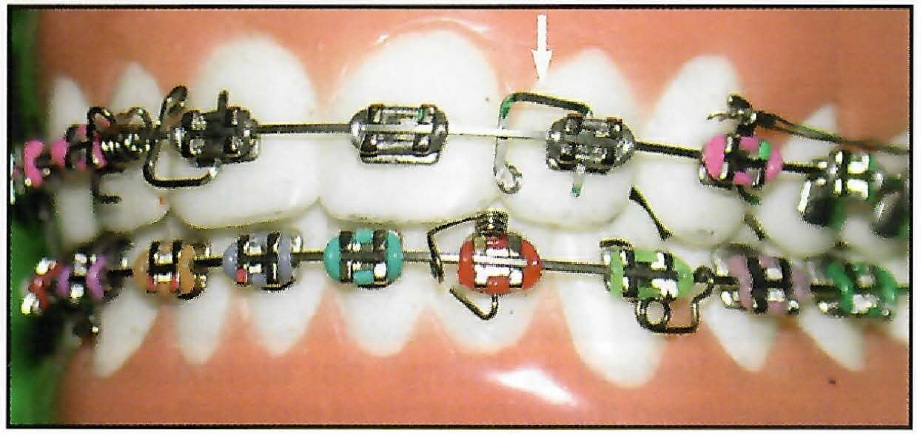
Fig. 4 U-Turn square-wire rotating spring (arrow).
The Compliance Spring** is an auxiliary that can be used for two distinct purposes. With a round archwire, an intermaxillary elastic from this spring will produce labial root torque for a specific tooth, such as a lingually displaced maxillary lateral incisor (Fig. 5A). With a rectangular archwire, the Compliance Spring can also be used to encourage cooperation with elastics (Fig. 5B). If the elastic is not worn, the spring will protrude enough to provoke a mild irritation of the cheek.
The Power Arm** was designed as a couple to apply forces from elastic chain, closed-coil springs, or intraoral elastics closer to the tooth's center of resistance (Fig. 6). This technique can help prevent tipping during space closure or retraction.
Traditional Begg uprighting springs*** are useful for root paralleling. When placed in the mandibular canine and/or first premolar brackets, they produce mesial crown tip that can counteract retraction forces on the mandibular anterior teeth14 (Fig. 7). Springs used in this configuration improve the effectiveness of mesial molar movement in cases where it is desirable to "slip anchorage", such as with congenitally missing second premolars.
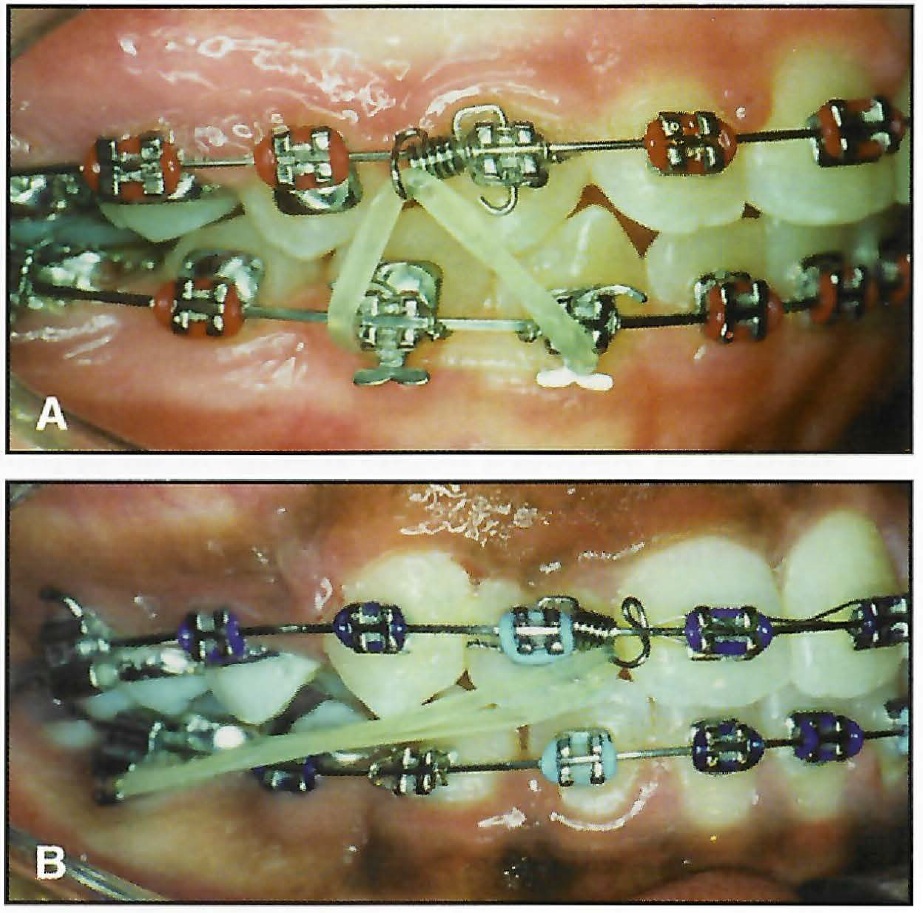
Fig. 5 A. Compliance Spring used with round stainless steel archwire and intermaxillary elastics to provide labial root torque. B. Compliance Spring reinforces wear of Class II elastics when used with rectangular archwire.
Progressive Posterior Torque
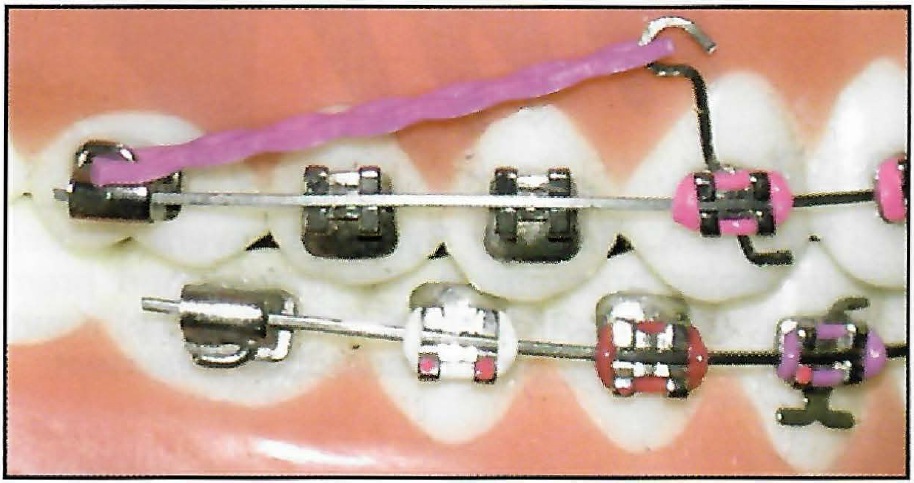
Fig. 6 Power Arm limits tipping when used with elastics, chains, or nickel titanium coil springs.
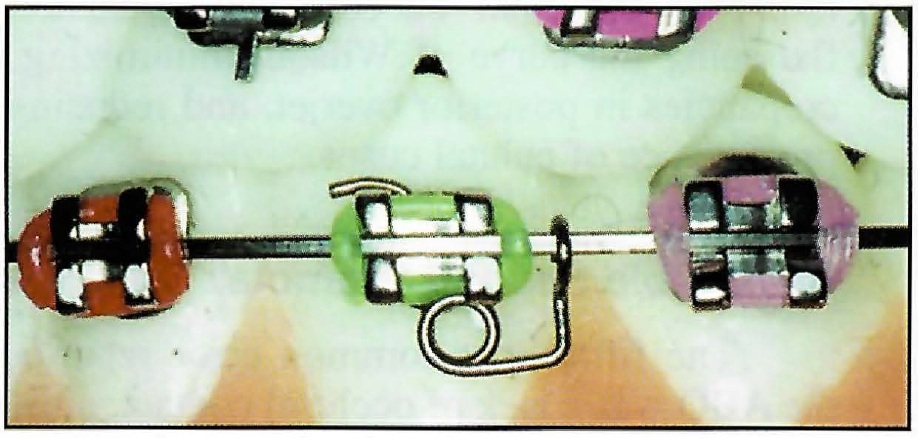
Fig. 7 Traditional Begg uprighting spring.
The most common deficiency of finished cases presented by either orthodontic residents or successful ABO candidates is improper buccolingual inclinations.1,15 Torque is not efficiently expressed with preadjusted appliances, because the area of torque application, which depends on the twisting effect of a thin wire, is quite small compared with the bulk of the tooth.5,12 In addition, most practitioners do not use full-size archwires of sufficient stiffness to express torque; for example, an .019" × .025" wire in an .022" ×.028" system has about 10° of play.
Many bracket prescriptions contain an extreme amount of mandibular posterior lingual crown torque, intended to obtain so-called "cortical anchorage".9 Compounding this problem is the increasingly popular use of "arch development", with overexpanded, highly resilient commercial arch blanks16 and bracket prescriptions having limited maxillary posterior lingual crown torque.11,17 This combination tends to tip the upper posterior teeth to the buccal and "roll in" the lower posterior teeth to the lingual, resulting in overly prominent maxillary palatal cusps, inappropriate interdigitation of the maxillary buccal cusps, increased occlusal interference, and an accentuated curve of Wilson12 (Fig. 8). It may lead to the fourth most prevalent error noted by the ABO--inappropriate overjet (with two-thirds of the errors exhibited in the posterior teeth).
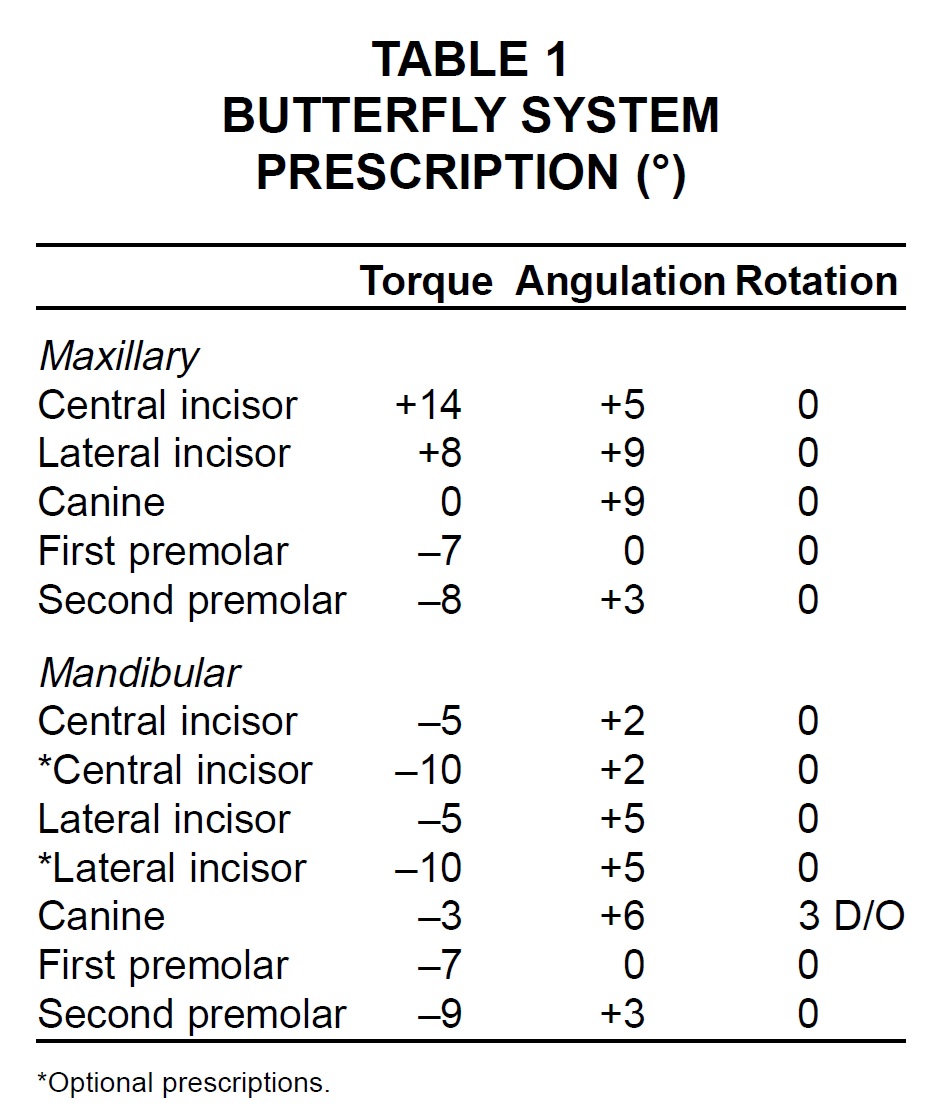
Progressive posterior torque was designed into the Butterfly System prescription to overcome these undesirable effects (Table 1). The maxillary posterior brackets have -14° of torque to help prevent buccal tipping of the first and second molars (Fig. 9). On the other hand, the mandibular first and second molar brackets have only -10° of lingual crown torque. Reducing the lower posterior torque while increasing the upper improves the final buccolingual occlusion by flattening the curve of Wilson, minimizing discrepancies in posterior overjet, and reducing the prominence of palatal cusps.
Reversible Second Premolar Brackets
The fifth most common error reported by the ABO was a lack of occlusal contact; although 50% of these errors involved second molars, the second premolars were also problematic. Ideally aligned second premolars have 2° of distal root inclination. The lack of tip in the many second premolar bracket prescriptions tends to promote inappropriate intercuspation, especially when there is a difference in height between the mesial and distal marginal ridges (Fig. 10). Therefore, mesial crown tip of +3° was designed into the Butterfly System second premolar bracket. This angulation helps reduce marginal-ridge discrepancies between the second premolar and first molar in the finished occlusion (Fig. 11).
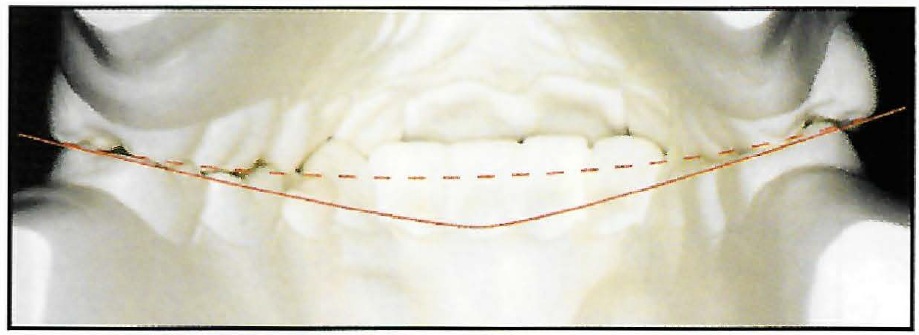
Fig. 8 Inappropriate posterior torque causes excessive curve of Wilson (solid line). Buccally tipped maxillary posterior teeth and “rolled-in” mandibular posterior teeth (dashed line = ideal curve of Wilson) lead to increased interferences.
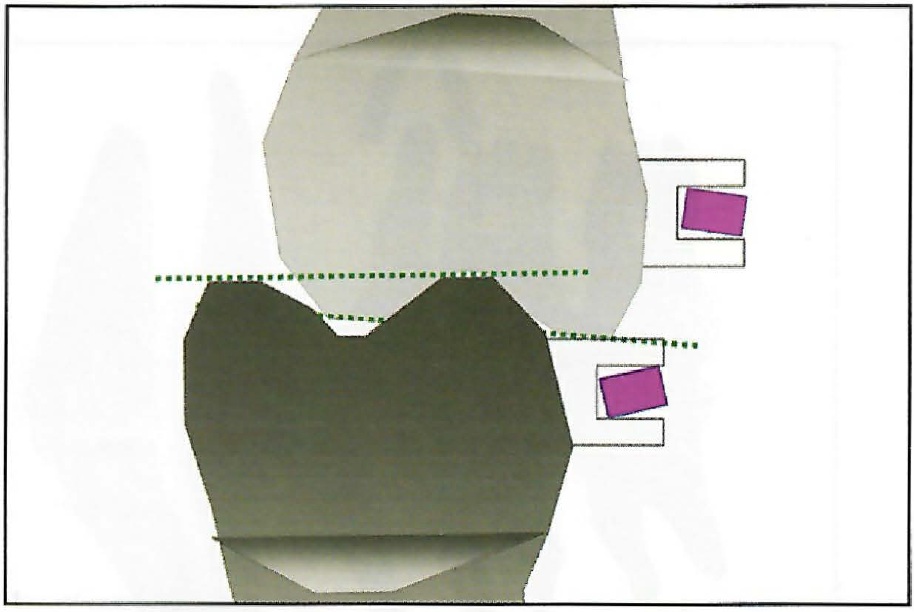
Fig. 9 Butterfly System features increased maxillary posterior torque (–14°) and reduced mandibular posterior torque (–10°) to improve intercuspation and posterior overjet, flatten curve of Wilson, and reduce interferences.
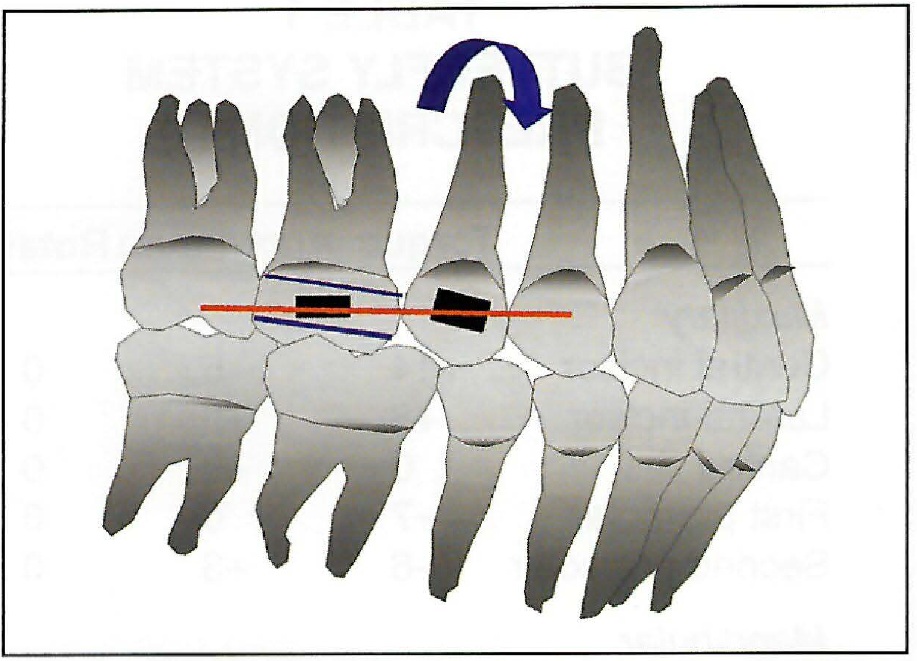
Fig. 10 Zero or negative angulation in second premolar bracket promotes improper intercuspation in nonextraction cases.
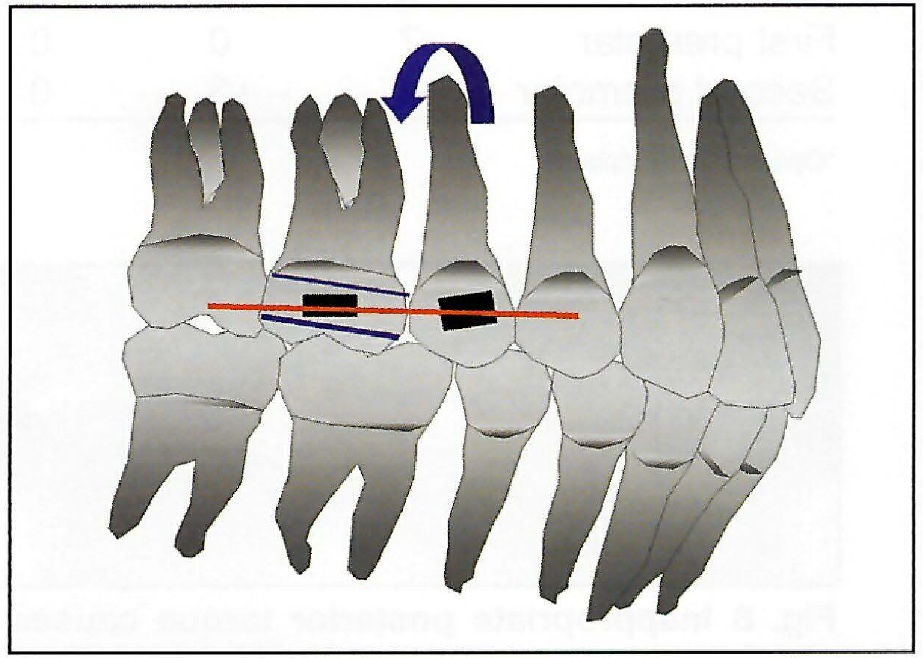
Fig. 11 Butterfly System second premolar brackets (+3° tip) improve posterior marginal ridge adaptation in nonextraction treatment.
The ABO described root angulation errors as the sixth most prevalent, with two-thirds occurring in the maxillary arch (lateral incisors, canines, and second premolars). Interestingly, ABO diplomates were found to have lower scores for root paralleling than those of orthodontic residents.15 Zero or positive angulation in second premolar brackets can lead to improper root angulation during space closure (Fig. 12). With the Butterfly System, in first premolar extraction cases, the second premolar brackets in both arches are switched to the contralateral sides (Fig. 13). This produces a distal crown tip of -3° to improve root paralleling between the second premolars and canines as their crowns tip toward each other during space closure.
In cases where second premolars are extracted or "slipping" posterior anchorage is planned, the upper and lower second premolar brackets are simply placed on the first premolars. The positive crown tip will help maintain the first premolar positions, assist in root paralleling with the first molars, and resist anterior retraction (Fig. 14). Placement of an uprighting spring, oriented to produce mesial crown tip, in the vertical slot of the canine bracket is another strategy that can be used to maintain the positions of anterior teeth while pulling the posterior teeth forward14(Fig. 7).
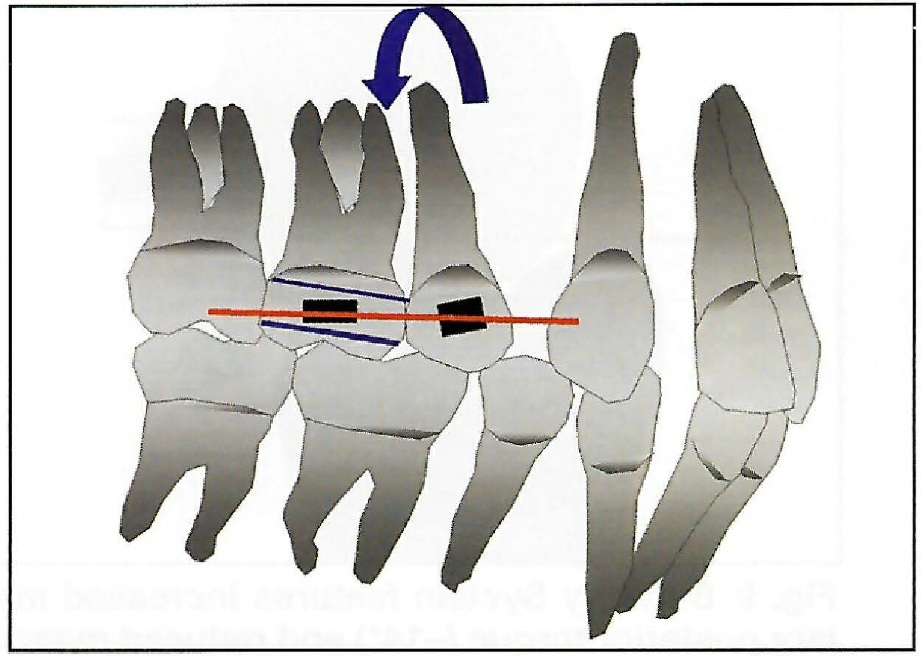
Fig. 12 Zero or positive angulation in second premolar brackets promotes improper root angulation during space closure.
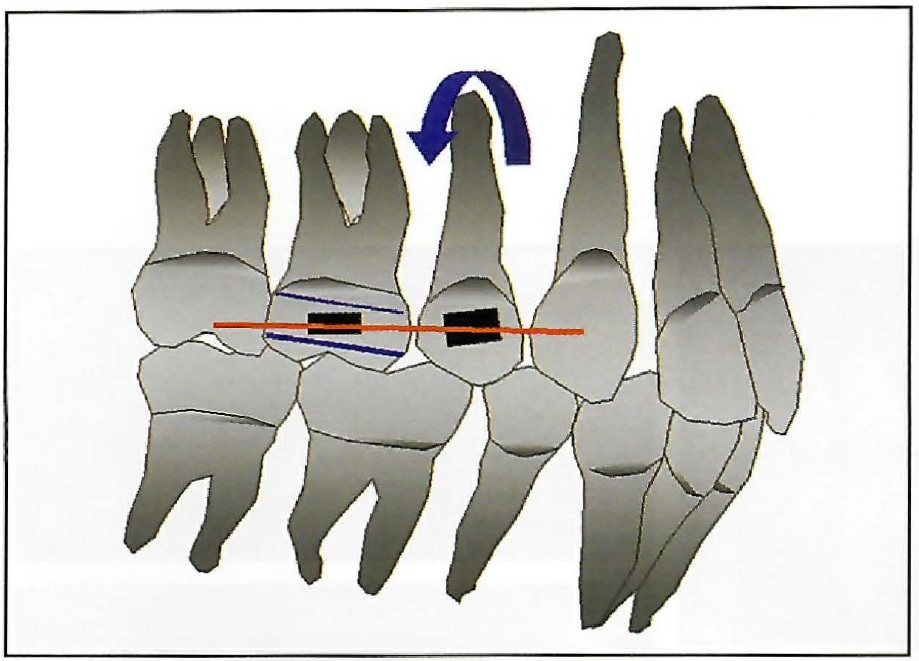
Fig. 14 Butterfly System second premolar brackets placed on first premolars to improve root parallel in during space closure after extraction of second premolars.
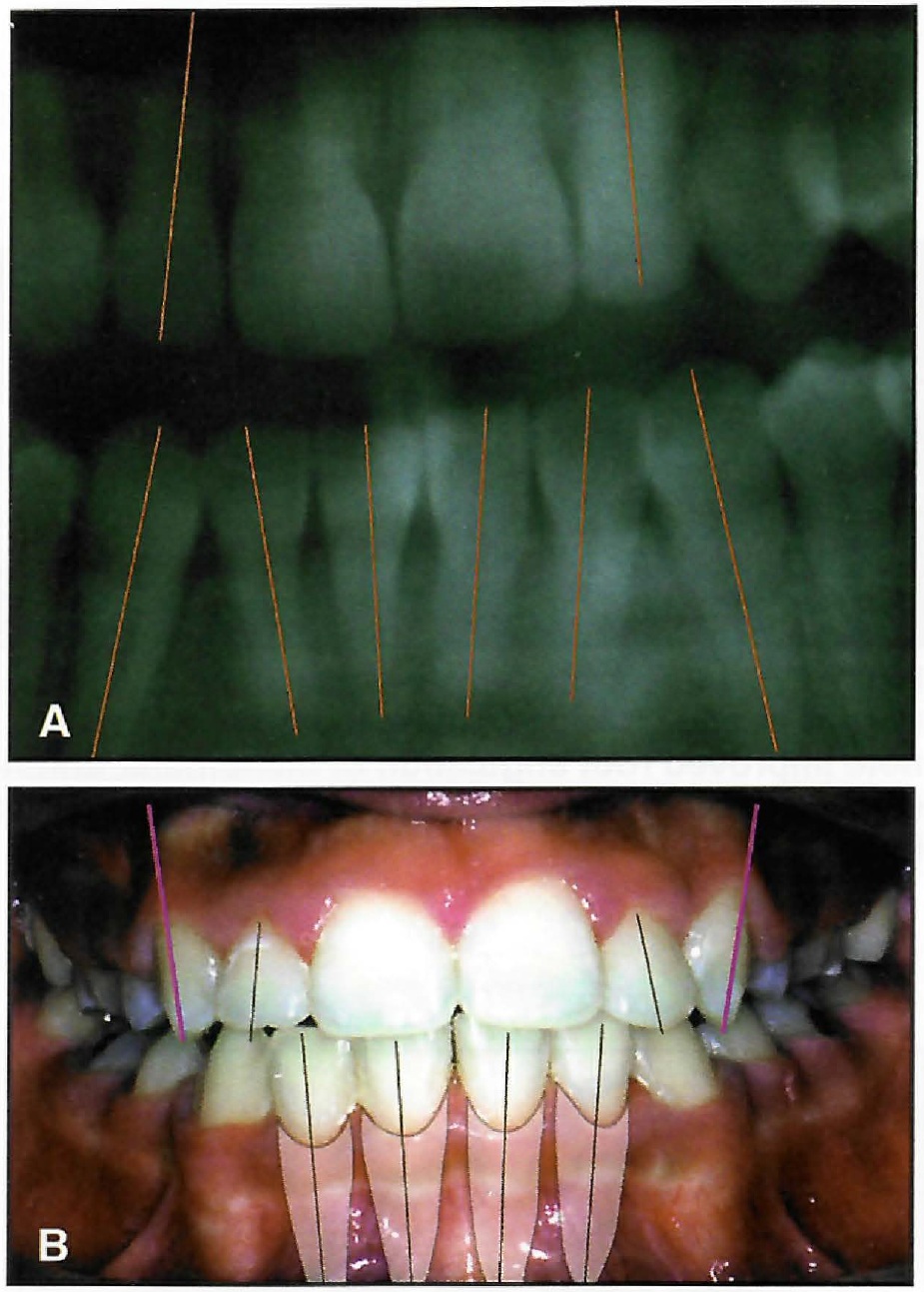
Fig. 15 A. Most popular preadjusted prescriptions have no angulation in mandibular anterior brackets. This may result in distal tipping of incisor crowns or root convergence, especially if less than-full-size archwires are used. B. Lingual displacement of maxillary canines can result from excessive lingual crown torque in many prescriptions.
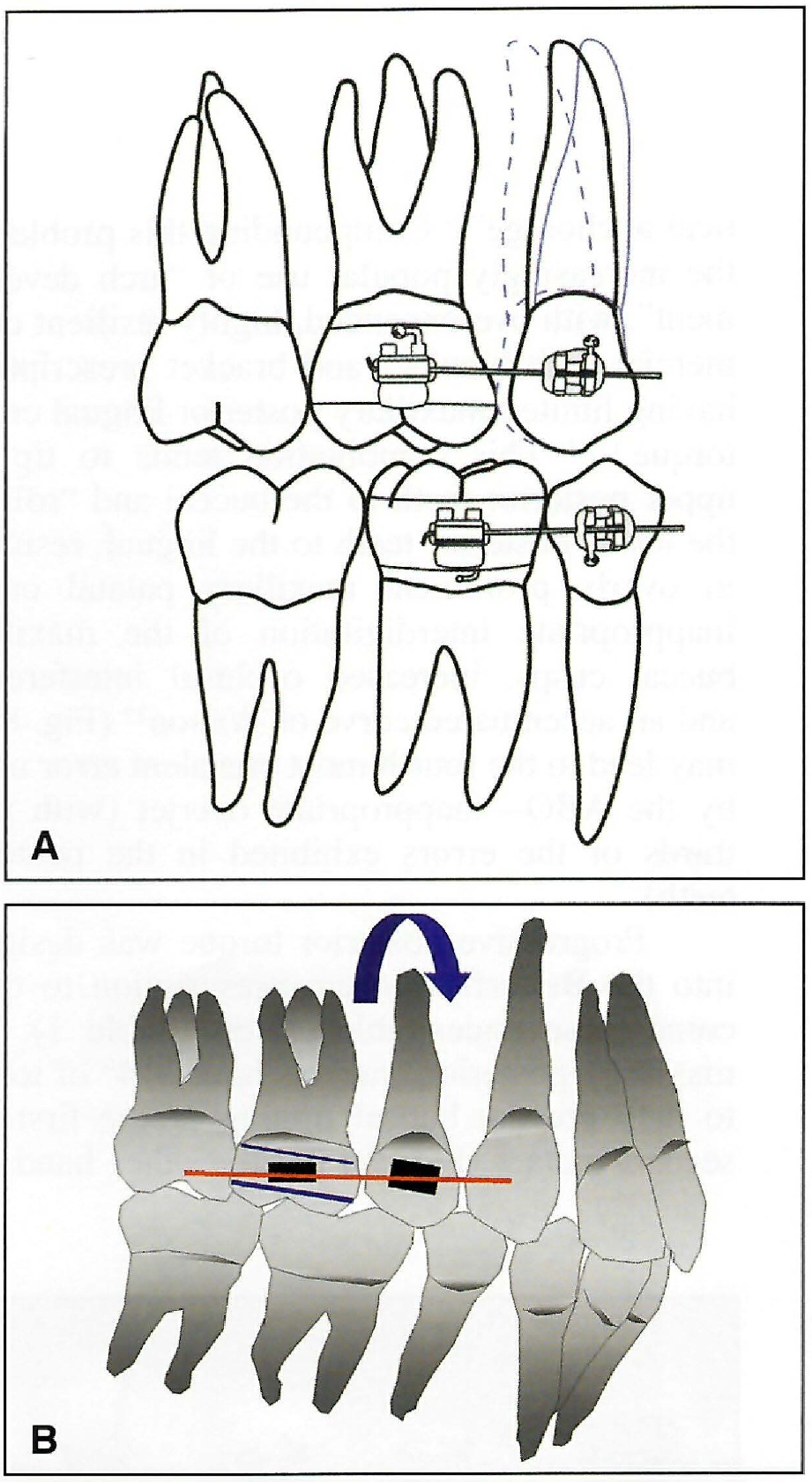
Fig. 13 A. Butterfly System’s reversible second premolar brackets. B. Placing second premolar brackets on contralateral sides (–3° tip) improves root paralleling during extraction treatment.
Progressive Mandibular Anterior Tip
The second most common error described by the ABO involved alignment of teeth. Although 50% of these errors were associated with second molars, the ABO was also concerned about anterior root angulation (Fig. 15). Consequently, progressive mandibular anterior mesial crown tip was incorporated into the Butterfly System. This reduces the typical distal crown tipping and root convergence of the lower incisors, improving the stability of finished cases by "tent-posting "the incisors (Fig. 16).
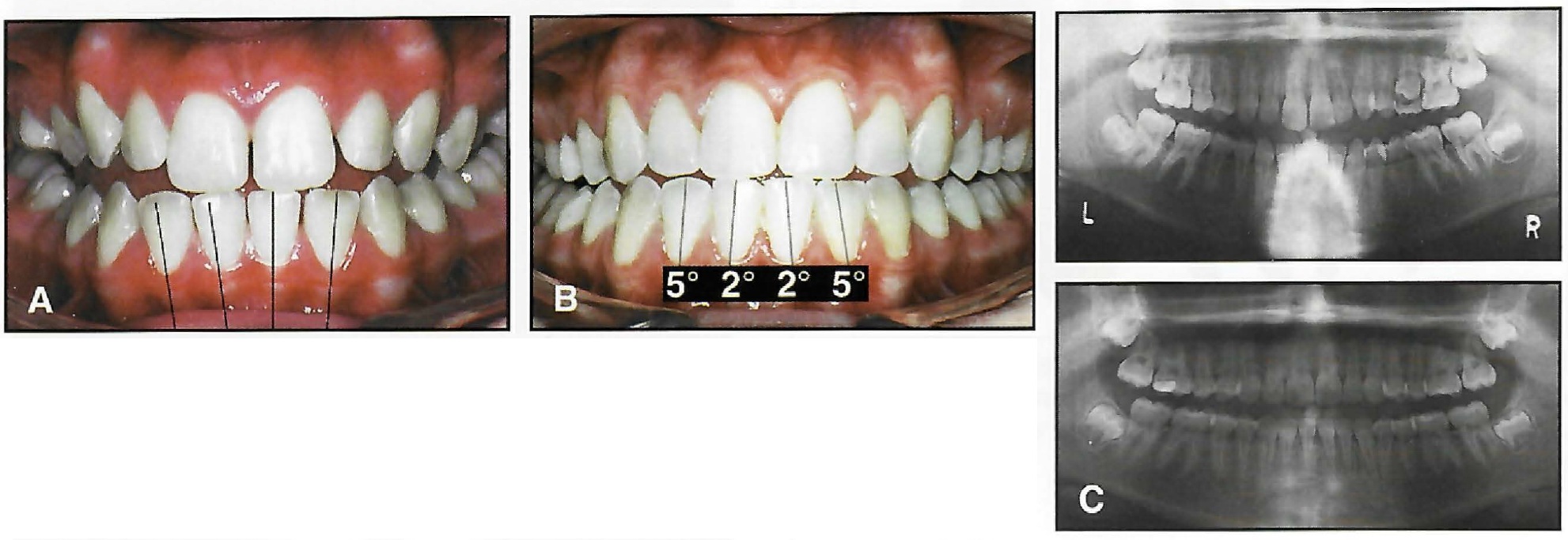
Fig. 16 A. 14-year-old female patient treated without extractions (patient shown in edge-to-edge position, not in occlusion). B. After 21 months, note improved root angulation of mandibular anterior teeth. C. Progressive anterior angulation in Butterfly System produced “tent-posting” of incisors.
Angulated First Molar Attachments
Third on the list of problems noted by the ABO were marginal ridge discrepancies, with 55% between the first and second molars and 33% between the second premolars and first molars. These errors may result from difficulties in posterior appliance placement due to limited visibility, gingival hypertrophy, variable clinical crown height, or delayed eruption.7 Another contributing factor is the difference in height between the mesial and distal marginal ridges of the maxillary first molar. Standard molar bands, fitted to the marginal ridge heights, are often positioned too far gingivally on the distal side, thus tipping the buccal molar tube distally. The results are excessive prominence of the first molar's distobuccal cusps, marginal ridge discrepancies, and occlusal interferences (Fig. 17). Bennett and McLaughlin recommended that the attachments, not the margins of the band, be placed parallel to the buccal cusps,5 but this makes it difficult to achieve an ideal fit of the band to the molar.
The Butterfly System incorporates -6° tip of the attachments welded to the first molar bands to compensate for the difference in marginal ridge heights, as in the Ricketts and Alexander prescriptions. When the bands are fitted evenly at the mesial and distal ridges, the bracket slot will be level (Figs. 18 and 19).
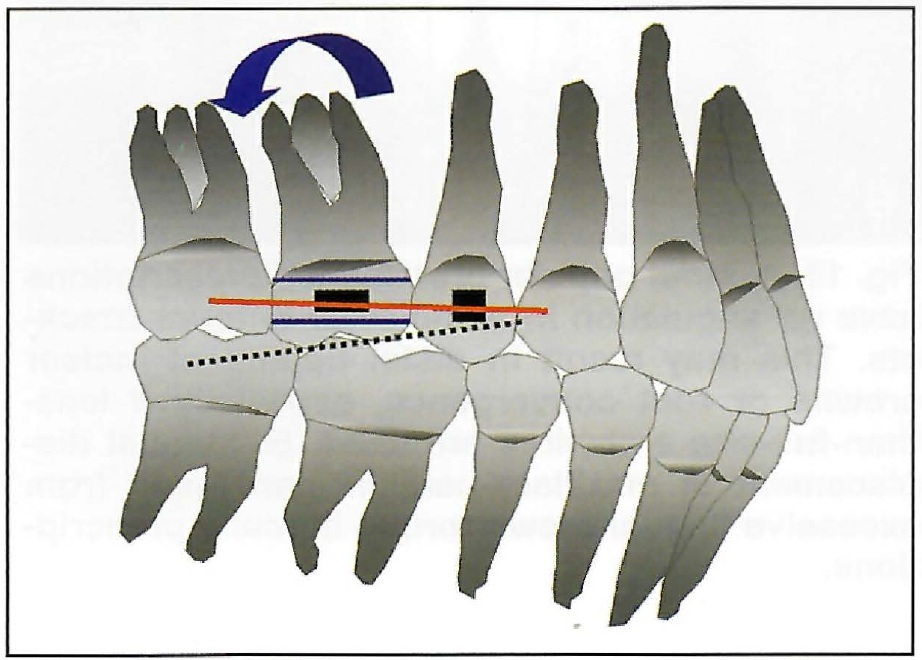
Fig. 17 Prominent distobuccal cusps result when first molar bands are fitted to marginal ridges instead of placing molar attachments parallel to buccal cusps.
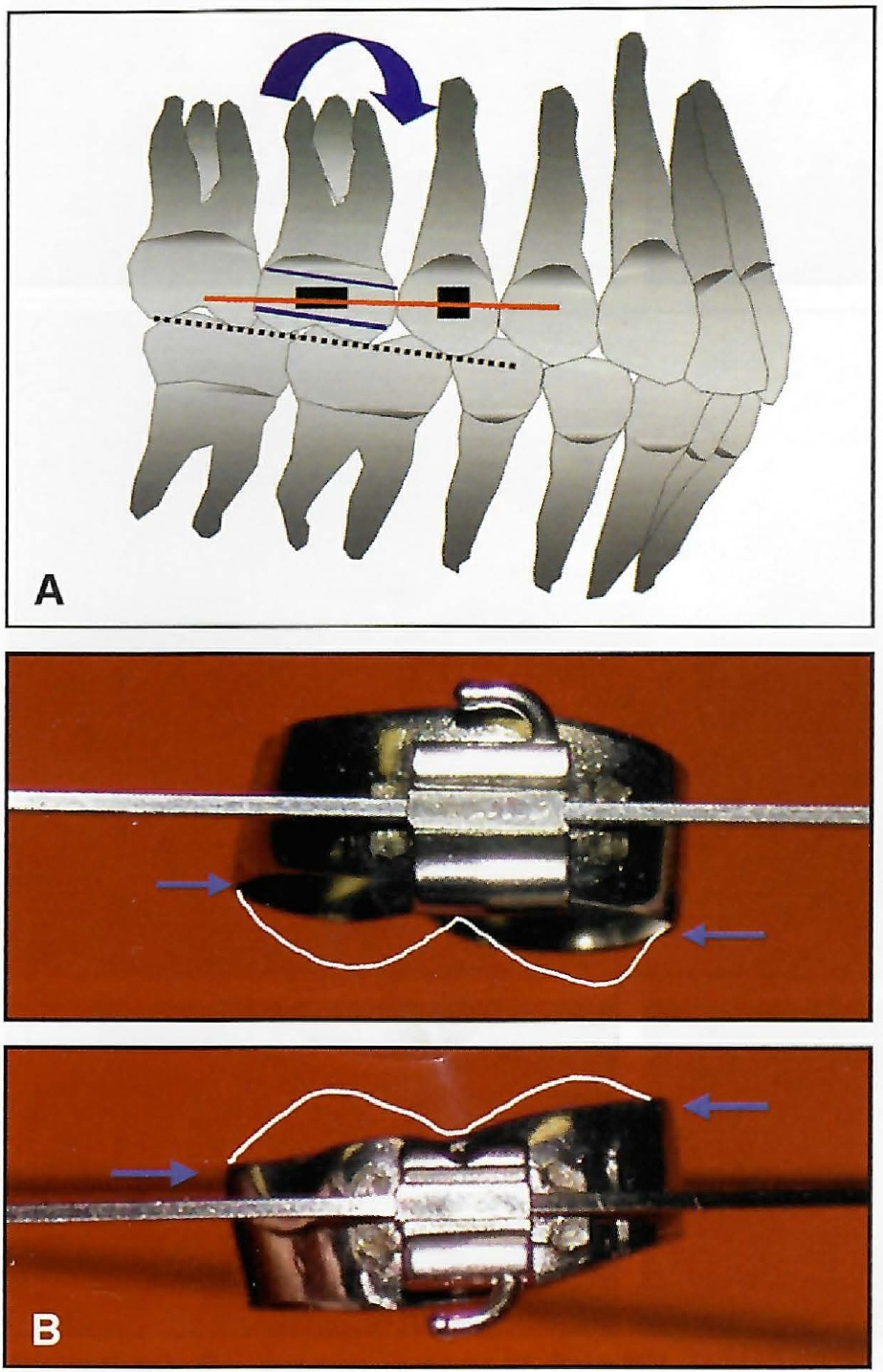
Fig. 18 A. Butterfly System molar attachments have –6° angulation to account for differences in first molar marginal ridges. B. When Butterfly System first molar bands are fitted to marginal ridges, tube angulation keeps buccal cusps parallel to occlusal plane.
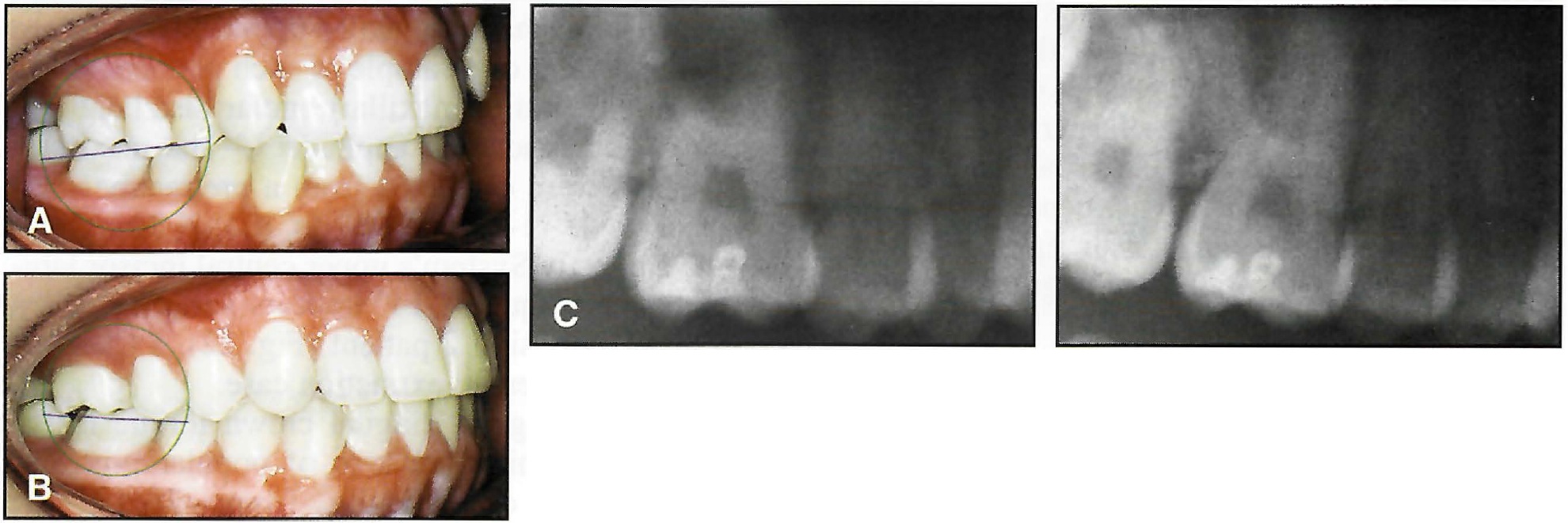
Fig. 19 A. 13-year-old female patient treated without extractions. B. After 12 months, note improved buccal cusp position due to angulation of attachments on Butterfly System’s first molar bands. C. Improved root paralleling and angulation of first molar (from panoramic x-rays).
Sondhi demonstrated the occurrence of "inappropriate or broken contacts between mandibular first and second molars" due to the distal offset of the first molar attachments in some popular prescriptions.11 Such an offset can displace the second molars to the lingual and/or rotate the first or second molars to the mesial, thus producing an incorrect lineup of the adjacent marginal ridges and contact points. There is no distal offset in the Butterfly System.
Preventive Mandibular Anterior Torque
Al Qabandi and colleagues reported 6-7° of lower incisor flaring simply from leveling the curve of Spee with fixed appliances.18 In addition, when Class II elastics are used, they can promote labial tipping of the mandibular anterior teeth (increasing instability and lip protrusion and taxing anchorage), clockwise rotation of the mandibular plane (increasing the Class II relationship and instability), and extrusion of the maxillary incisors (increasing gingival display).6,18-24 Even though various authors have recommended -5° to -10° of lower incisor lingual crown torque to limit flaring when supporting Class II mechanics,20-22 many bracket prescriptions have only -1° to +1° of torque.
According to Creekmore, "If anterior teeth are pushed forward, they will end up with about 3° more torque than the torque in the brackets. If retracted, they will end up with about 3° less torque than the torque in the brackets. This is why prescriptions must be varied according to the treatment planned for the individual if 0° torque archwires are to be used (i.e., straightwire arch blanks)."4
The lingual crown torque of -5° in the mandibular anterior brackets of the Butterfly System is intended to resist the incisor tipping inherent in leveling mechanics. Optional brackets for the four mandibular incisors have -10° of preventive torque to counteract the additional labial tipping from Class II elastics or fixed functional appliances such as the Jasper Jumper** or the Herbst† (Figs. 20 and Figs. 21. These two torque options reduce the amount of wire bending required to compensate for labial incisor tipping. If less torque is desired, a smaller rectangular archwire can be used.
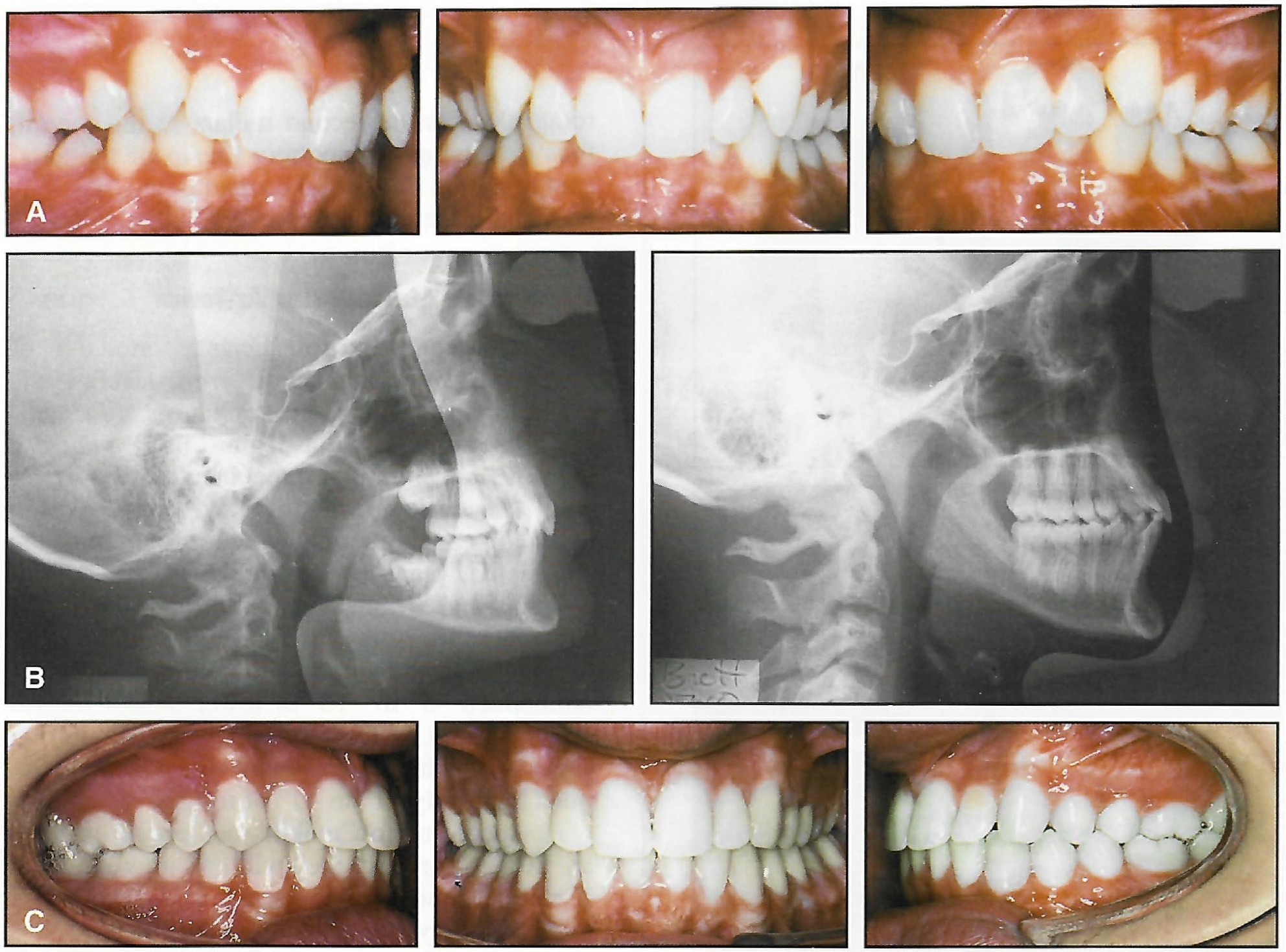
Fig. 20 A. 13-year-old male patient treated with combination of Distal Jet and Jasper Jumpers. B. Improved maxillary incisor position; lower incisor brackets with –10° lingual crown torque limited incisor flaring from fixed functional appliance (no change in IMPA). C. After 34 months of treatment.
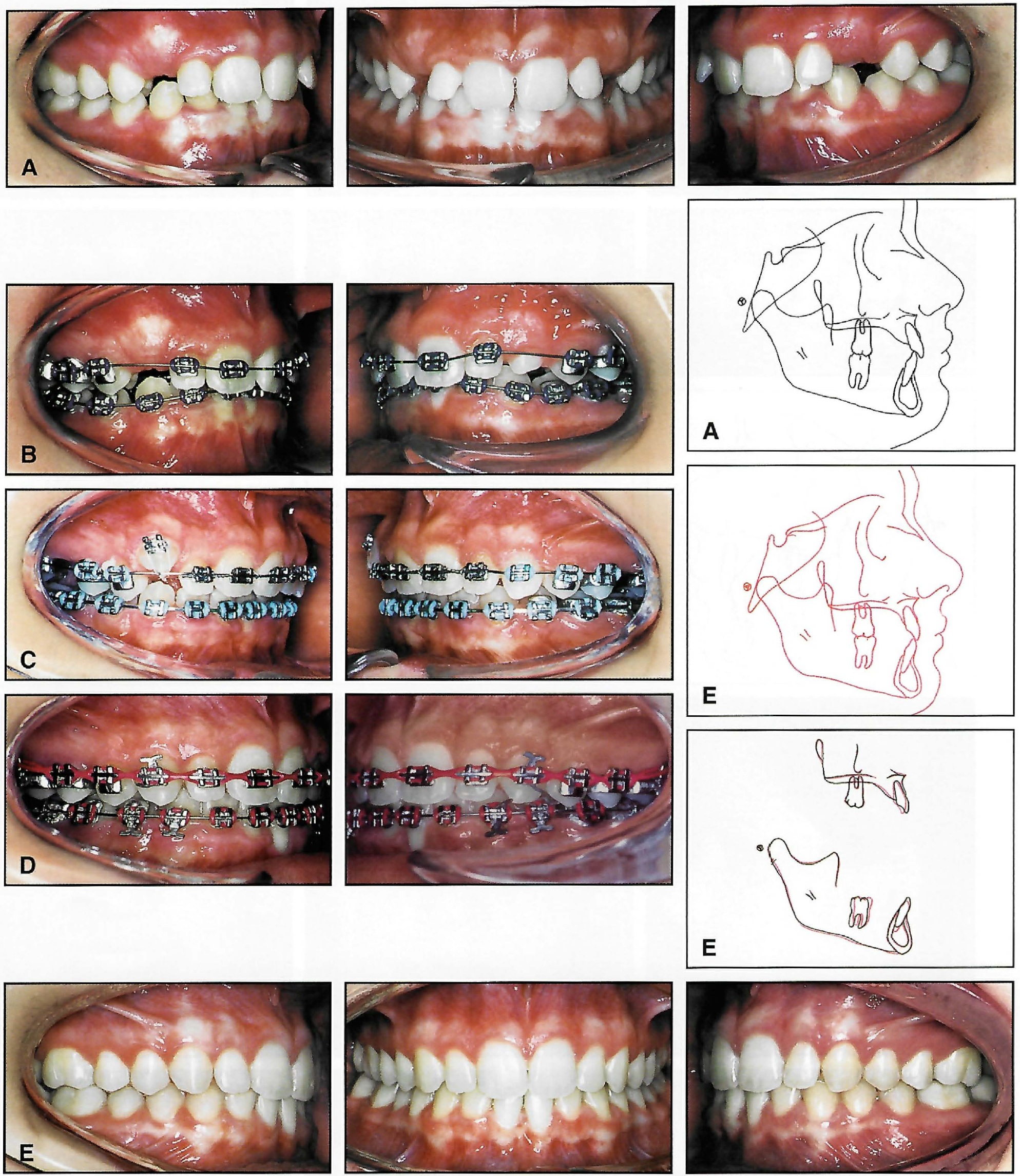
Fig. 21 A. 12-year-old female patient treated with Class II Combination Therapy (Distal Jet followed by Jasper Jumpers). B. Esthetics and oral hygiene improved by Butterfly System’s low-profile brackets without hooks. C. Jasper Jumpers used between stages. D. T-pins inserted into vertical slots only when intermaxillary elastics were required. E. After 24 months of treatment. Lower incisor angulation was maintained (no increase in IMPA) by using optional –10° torque brackets.
Conservative Anterior Torque
Sondhi indicated that more upper incisor torque is required for Class II, division 2 cases, which often have lingually tipped incisors.11 In our treatment of a sample of such patients, using a combination of maxillary molar distalization25 and fixed functional appliances,26 the maxillary incisors were corrected from a pretreatment incisal angle (1-SN) of 98° to 104°.27 Therefore, the Butterfly System's upper central incisor labial crown torque of 14° appears sufficient for a Class II, division 2 patient (Fig. 22), a Class III patient, or even an extraction case.
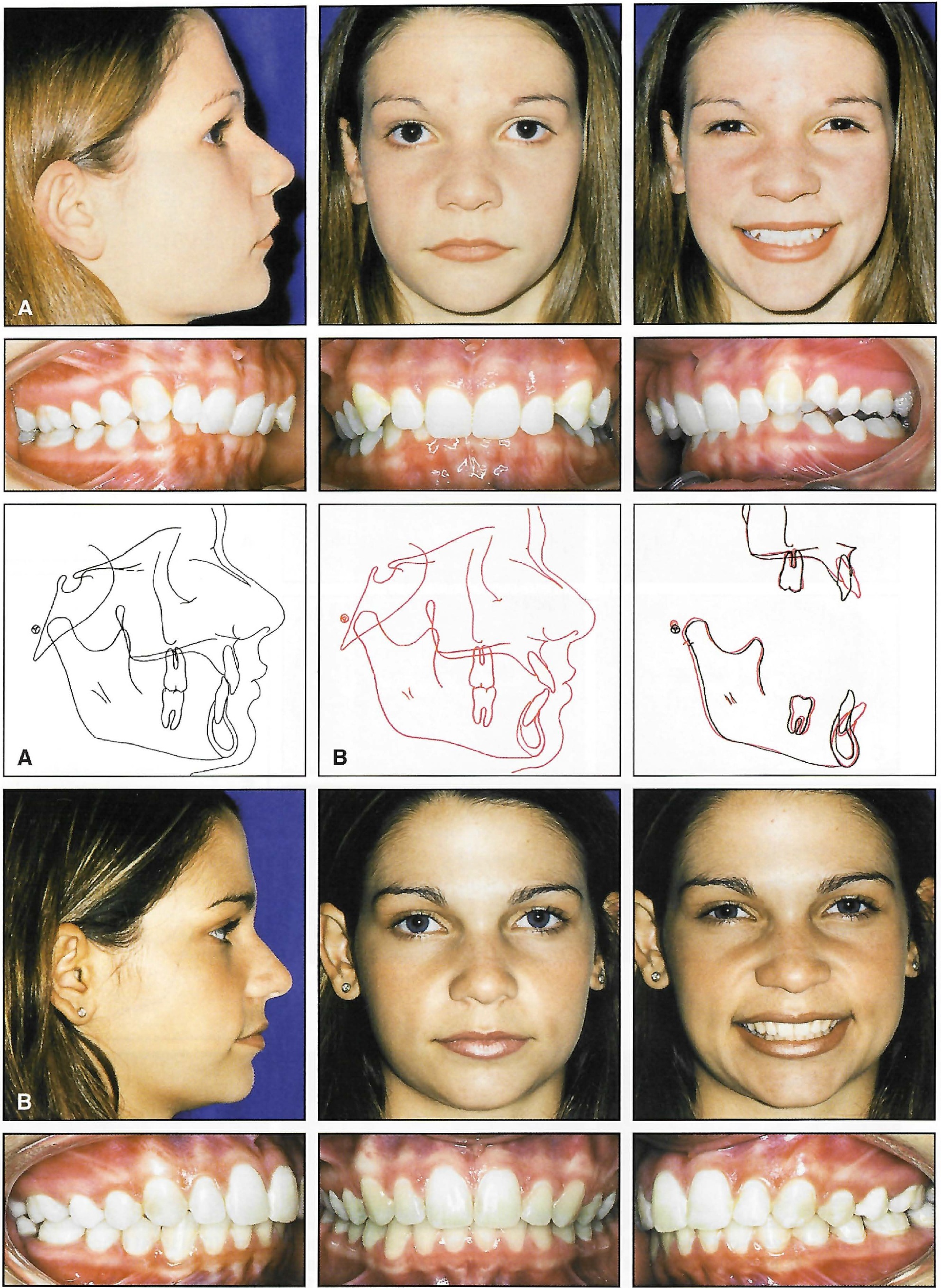
Fig. 22 A. 16-year-old female patient with Class II, division 2 malocclusion treated with Class II Combination Therapy (molar distalization followed by fixed functional appliance). B. Patient after 36 months of treatment.
The range of lingual crown torque in the maxillary canine brackets of popular prescriptions varies dramatically, from -7° to +7°. Excessive lingual crown torque of the maxillary canine produces lingual displacement compared to the other anterior teeth11 (Fig. 15). This is especially important when attempting to maintain the roots within the cancellous bone during retraction mechanics.12 McLaughlin and colleagues recommended no torque for canines that are prominently positioned in the pretreatment archform.12 To prevent lingual displacement of the canines and to split the difference between the extremes, the Butterfly prescription has no torque in the maxillary canine brackets.
A similar situation exists with popular mandibular canine prescriptions, which range from -11° to +7° of torque. To match the reduced progressive posterior torque of the Butterfly System, the mandibular canine features a moderate -3° of torque. In deep-bite cases, the canine bracket can be inverted (+3° torque) to move the crown labially while keeping the roots within the supporting bone.5,12
Improvements in Overjet
The fourth most prevalent error noted by the ABO was inappropriate overjet, with two-thirds of these problems in the posterior teeth. When overexpanded commercial arch blanks are combined with bimaxillary expansion therapies, the results may include a discrepancy in both anterior and posterior overjet, as well as flared molars and distally tipped incisors. The esthetic effect is a "wider than normal smile"24 or the "orthodontic look" described by Proffit.28
Progressive posterior torque in the Butterfly System (reduced mandibular and increased maxillary torque) helps prevent flared maxillary molars and rolled-in mandibular posterior teeth. It is also important, whenever possible, to select an archform that is consistent with the patient's pretreatment anatomical shape while maintaining the pretreatment intercanine width.5,12 Archforms should be coordinated throughout treatment with these principles in mind (Table 2).
Bonding Pad Enhancements
The Maximum Retention** bonding pads on Butterfly System brackets have photoetched pockets beneath the mesh to enhance bond strength (Fig. 23). Optional offset bases on the premolar brackets provide larger bonding surfaces that not only improve bond strength, but make bracket positioning easier to visualize (Figs. 1 and 24). The offset also offers the option of placing the bracket more gingivally to improve marginal ridge orientation.
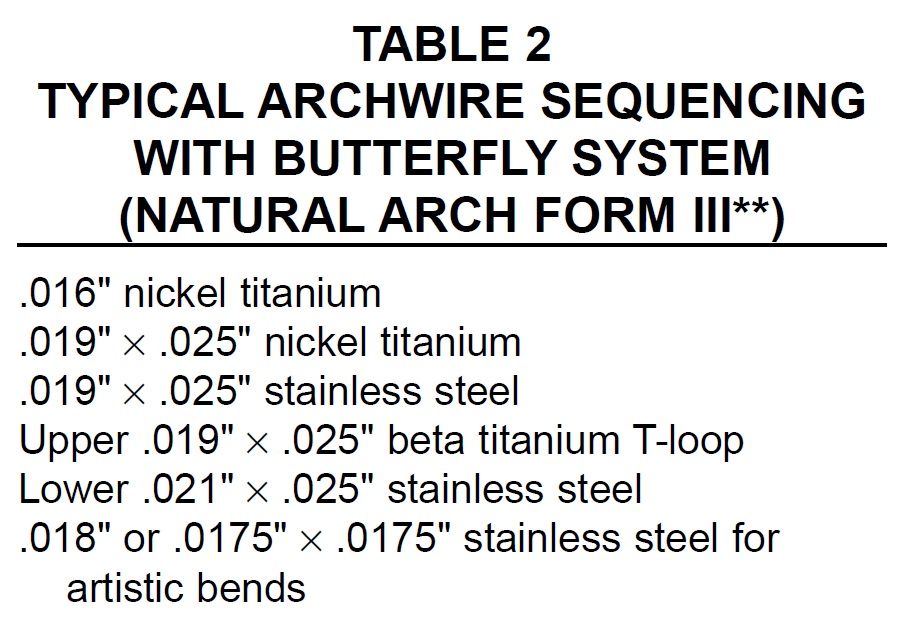
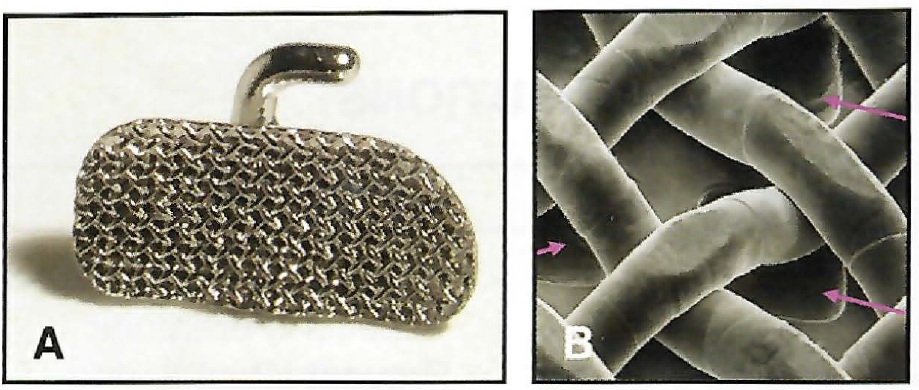
Fig. 23 A. Maximum Retention bonding pad. B. Photoetched pockets beneath mesh pad increase surface area for bonding adhesive.
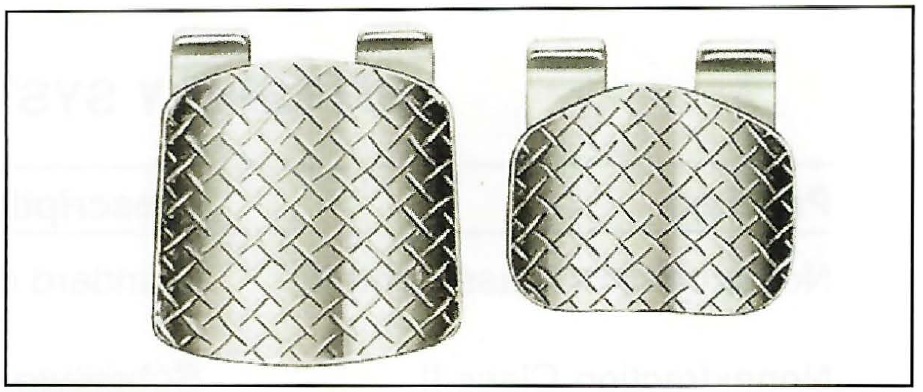
Fig. 24 Optional offset and standard Butterfly System premolar brackets. Offset pads increase surface area to enhance bond strength.
Conclusion
Design concepts of the Butterfly System included esthetics, comfort, versatility, and color. The miniature twin Butterfly bracket features a low profile and an improved radius for the tiewing corners. Its multipurpose vertical slot eliminates hooks. The system also accommodates the colorful elastomeric ligatures that many of today's patients are requesting to personalize their braces.
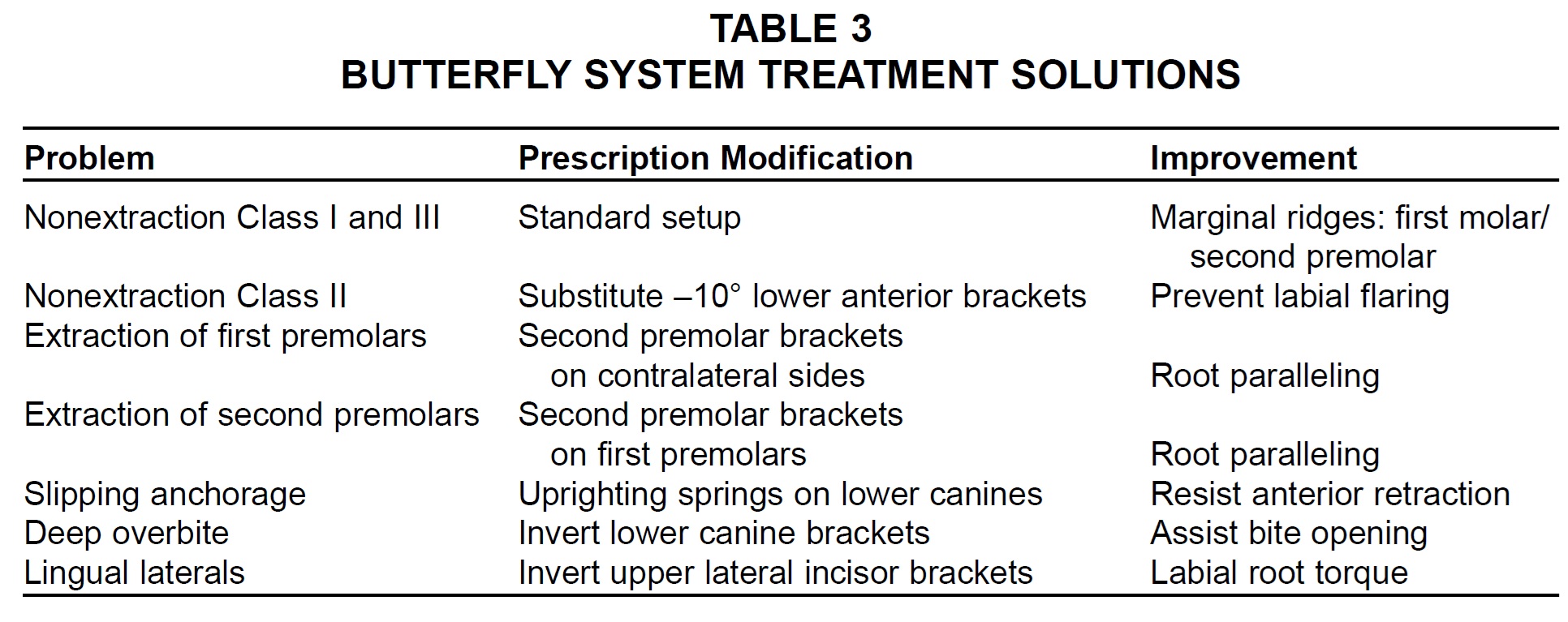
The Butterfly System prescription was based on modifications to the second-generation preadjusted appliance, in response to case completion errors documented by the ABO1,7 (Table 3). The intent was to take the best from the past while avoiding common problems, thus producing more efficient treatment and more favorable results for our patients.
FOOTNOTES
- *Trademark of Ormco/“A” Company, 1717 W. Collins Ave., Orange, CA 92867.
- **Trademark of American Orthodontics, Inc., 1714 Cambridge Ave., Sheboygan, MI 53082.
- ***TP Orthodontics, Inc., 100 Center Plaza, La Porte, IN 45350.
- †Registered trademark of Dentaurum, Inc., 10 Pheasant Run, Newtown, PA 18940.
REFERENCES
- 1. American Board of Orthodontics: Why case reports do not pass the ABO Phase III clinical examination, Am. J. Orthod. 110:559-560, 1996.
- 2. Creekmore, T.D. and Kunik, R.L.: Straight wire: The next generation, Am. J. Orthod. 104:8-20, 1993.
- 3. Roth, R.H.: Treatment mechanics for the straight wire appliance, in Orthodontics: Current Principles and Techniques, ed. T.M. Graber and R.L. Vanarsdall, Jr., 2nd ed., Mosby, St. Louis, 1985.
- 4. Creekmore, T.D.: Vertical dimension is a compounding problem, Readers' Forum, Am. J. Orthod. 117:12A-13A, 2000.
- 5. Bennett, J.C. and McLaughlin, R.P.: Orthodontic Management of the Dentition with the Preadjusted Appliance, Isis Medical Media, Oxford, England, 1997.
- 6. Alexander, R.G.: Alexander Discipline: Contemporary Concepts and Philosophies, Ormco, Glendora, CA, 1986.
- 7. Bowman, S.J.: Addressing concerns for finished cases: The development of the Butterfly bracket system, J. Ind. Orthod. Soc. 36:73-75, 2003.
- 8. Andrews, L.F.: Straight Wire: The Concept and Appliance, L.A. Wells, San Diego, CA., 1989.
- 9. Ricketts, R.M.; Bench, R.W.; Gugino, C.F.; Hilgers, J.J.; and Schulhof, R.J.: Bioprogressive Therapy, Rocky Mountain Orthodontics, Denver, 1979.
- 10. Sondhi, A.: Sondhi Signature Treatment System, 3M Unitek Orthod. Persp. 9:3-8, 2002.
- 11. Sondhi, A.: An analysis of orthodontic prescriptions: Their strengths and weaknesses, AAO annual session, Honolulu, May 6, 2003.
- 12. McLaughlin, R.P.; Bennett, J.C.; and Trevisi, H.J.: Systemized Orthodontic Treatment Mechanics, Mosby, St. Louis, 2001.
- 13. Bowman, S.J. and Carano, A: Improvements in pre-adjusted appliances: Butterfly brackets, Am. Orthod. Good Pract. 2:5-7, 2001.
- 14. Kesling, P.C.: Begg theory and technique: Past, present, and future, in New Vistas in Orthodontics, ed. L.E. Johnston, Jr., Lea and Febiger, Philadelphia, 1985.
- 15. Yang-Powers, L.C.; Sadowsky, C.; Rosenstein, S.; and BeGole, E.A.: Treatment outcome in a graduate orthodontic clinic using the American Board of Orthodontics grading system, Am. J. Orthod. 122:451-455, 2002.
- 16. Braun, S.; Hnat, W.P.; Leschinsky, R.; and Legan, H.L.: An evaluation of the shape of some popular nickel titanium alloy preformed arch wires, Am. J. Orthod. 116:1-12, 1999.
- 17. McNamara, J.A. Jr. and Brudon, W.L.: Orthodontics and Dentofacial Orthopedics, Needham Press, Ann Arbor, MI, 2001.
- 18. Al Qabandi, A.; Sadowsky, C.; and BeGole, E.: A comparison of the effects of rectangular and round arch wires in leveling the curve of Spee, Am. J. Orthod. 116:522-529, 1999.
- 19. Tahir, E.; Sadowsky, C.; and Schneider, B.J.: An assessment of treatment outcome in American Board of Orthodontics cases, Am. J. Orthod. 111:335-342, 1997.
- 20. Gianelly, T.: Bidimensional Technique: Theory and Practice, GAC International, Islandia, NY, 2000.
- 21. Smith, S.S. and Alexander, R.G.: Orthodontic correction of a Class II division 1 subdivision right open bite malocclusion in an adolescent patient with a cervical pull face-bow headgear, Am. J. Orthod. 116:60-65, 1999.
- 22. Ruf, S.; Hansen, K.; and Pancherz, H.: Does orthodontic proclination of lower incisors in children and adolescents cause gingival recession? Am. J. Orthod. 114:100-106, 1998.
- 23. Bowman, S.J. and Johnston, L.E. Jr.: The esthetic impact of extraction and nonextraction treatments on Caucasian patients, Angle Orthod. 70:3-10, 2000.
- 24. Bowman, S.J. and Johnston, L.E. Jr.: Much ado about facial esthetics, in Treatment Timing: Orthodontics in Four Dimensions, ed. J.A. McNamara Jr. and K. Kelly, vol. 39, Craniofacial Growth Series, University of Michigan, Ann Arbor, 2002.
- 25. Bolla, E.; Muratore, F.; Carano, A.; and Bowman, S.J.: Evaluation of maxillary molar distalization with the Distal Jet:A comparison with other contemporary methods, Angle Orthod. 72:481-494, 2002.
- 26. Bowman, S.J.: Class II combination therapy, J. Clin. Orthod. 32:611-620, 1998.
- 27. Ngantung, V.; Nanda, R.S.; and Bowman, S.J.: Posttreatment evaluation of the Distal Jet appliance, Am. J. Orthod. 120:178-185, 2001.
- 28. Proffit, W.R.: Contemporary Orthodontics, 2nd ed., Mosby, St. Louis, 1993.
-
 DR. BOWMAN
DR. BOWMAN -
 DR. CARANO
DR. CARANO
Dr. Bowman is an Adjunct Associate Professor at St. Louis University and the straightwire instructor at the University of Michigan. He is in the private practice of orthodontics at 1314 W. Milham Ave., Portage, MI 49024; e-mail: drjwyred@aol.com. Dr. Carano is an Adjunct Professor at St. Louis University and a Visiting Professor at the University of Ferrara, and is in the private practice of orthodontics in Taranto, Italy.