JCO Interviews Dr Junji Sugawara on the Skeletal Anchorage System
DR. WHITE When and how did you develop the idea for the Skeletal Anchorage System (SAS)?
DR. SUGAWARA In 1992, we had a patient with a severe anterior crossbite and no molars for anchorage in the mandibular dentition (Fig. 1). She had an average-size mandible, so orthognathic surgery was not an option. We decided to apply an anchorage system that we had read about and was similar to dental implants. Her alveolar bone was not thick enough to contain permanent implants. We didn't know which of two systems would be the more comfortable for the patient, so we used a simple titanium screw on one side and a titanium miniplate on the other.
DR. WHITE Was one more comfortable than the other?
DR. SUGAWARA She had significant pain with the screw, but no discomfort with the miniplate. The mechanics of the miniplate are simpler, in that the screw alone requires a lead wire that must go through the mucosa, and that is uncomfortable. With the miniplate, there is minimal discomfort--much less than for something like a tooth extraction. The placement of the miniplates is done under local anesthetic and requires only about 10 minutes for each plate. Sometimes there is a little swelling in the face, but it is accompanied by minimal pain.
Similar articles from the archive:
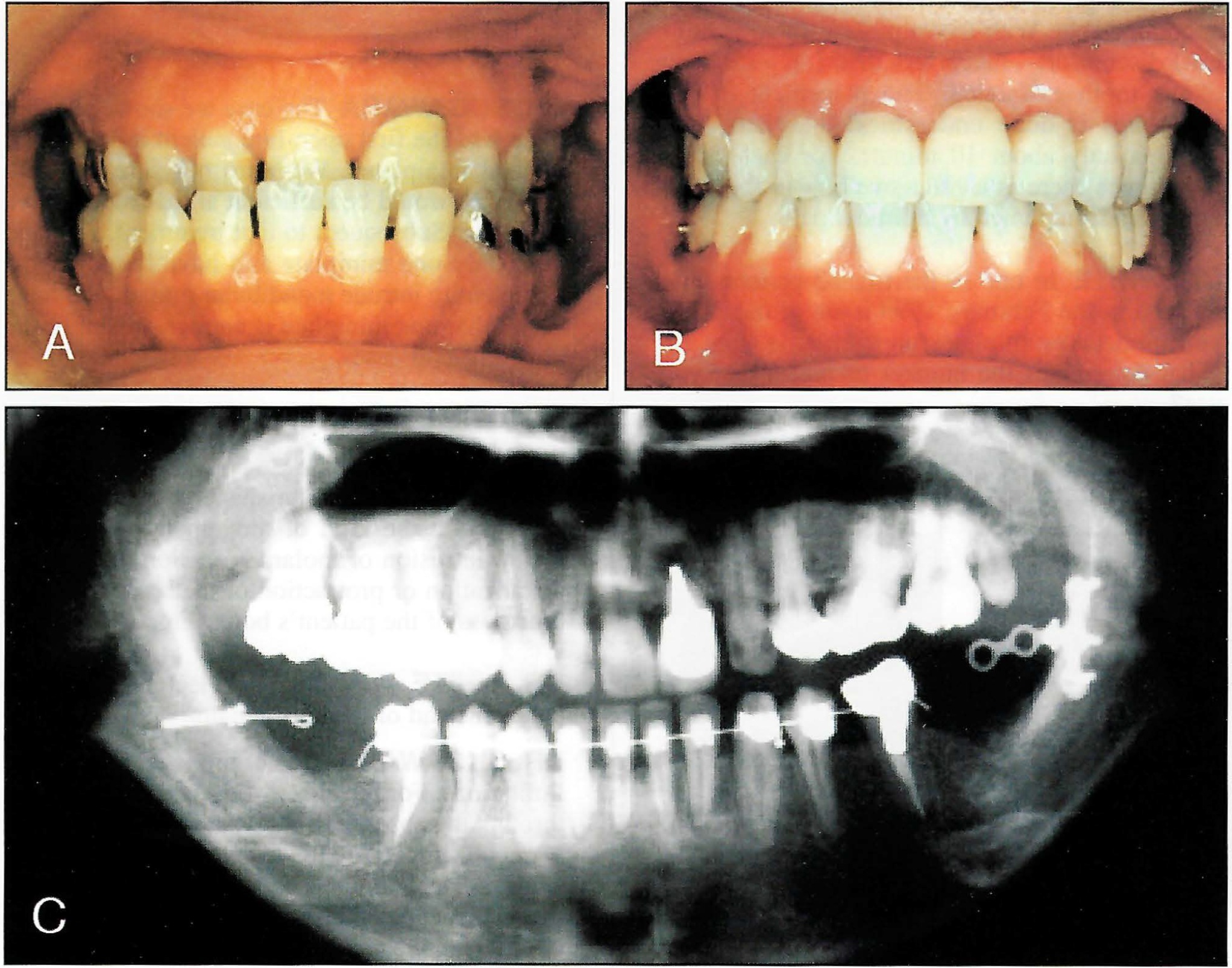
Fig. 1 First SAS patient (1992). A. Before treatment. B. Three years after debonding. C. Panoramic x-ray taken during treatment, with titanium screw on patient's right and titanium miniplate on patient's left.
DR. WHITE In one of the treated patients you showed in the February 1999 issue of the AJO,1 you used two miniplates on each side (Fig. 2). What determines the number of plates that you use?
DR. SUGAWARA The case we showed in that issue was the first open-bite patient in which we applied miniplates. We were not sure that one miniplate would be sufficient at that time, so we used two. Subsequent to that treatment, we have used only one miniplate and have found that is sufficient to intrude mandibular molars. We have found that one miniplate is enough--even in the most difficult cases.
DR. WHITE How do you decide what shape of miniplate to use?
DR. SUGAWARA The shape of the miniplate depends on the kind of movement we want to attain: intrusion of molars, intrusion of incisors, distalization or protraction of teeth, etc., and the thickness of the patient's bone (Fig. 3).
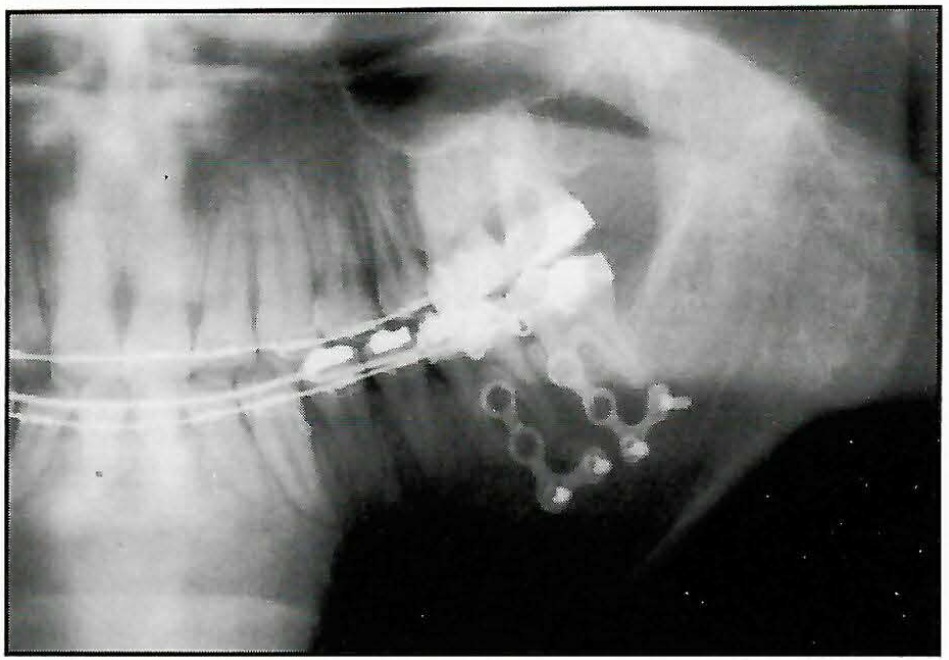
Fig. 2 SAS using two titanium miniplates on one side.
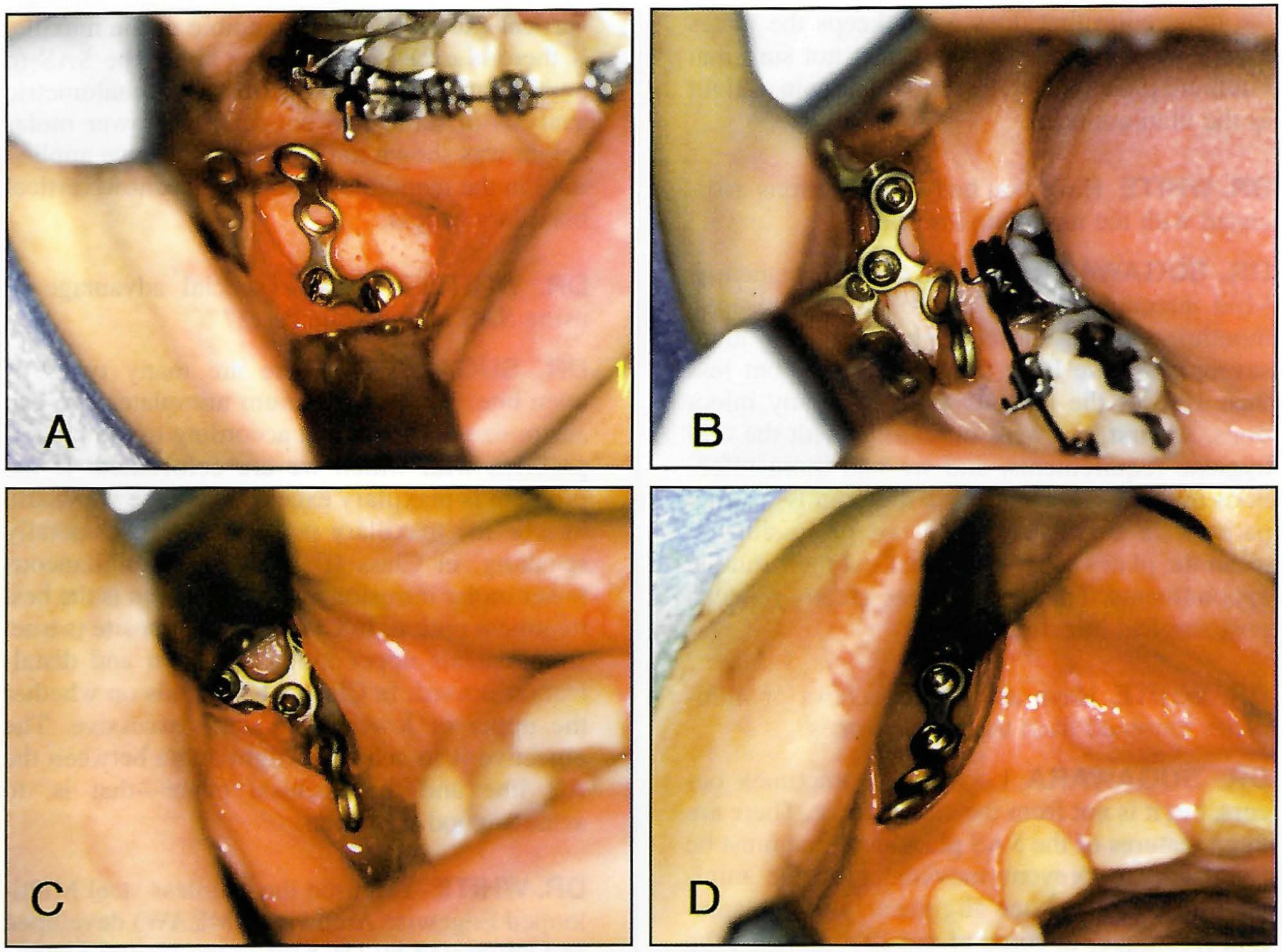
Fig. 3 A. L-shaped titanium miniplate for intrusion of mandibular molars (mandibular body). B. L-shaped titanium miniplate for distal movement of mandibular molars (retromolar pad). C. Y-shaped titanium miniplate for intrusion and distalization of maxillary molars (key ridge). D. Straight titanium miniplate for intrusion of maxillary incisors (anterior ridge of piriform opening). (Reprinted by permission.5)
DR. WHITE Why did you elect to use miniplates instead of dental implants?
DR. SUGAWARA Dental implants have many limitations. For instance, when space is available through the absence of a molar, it is easy to place a dental implant. However, in full dentitions where space is limited, there are few if any areas that can accept the typical dental implant. On the other hand, we can use our miniplates just about anywhere without worrying about destroying teeth or bone.
DR. WHITE Could you simply place the screws directly through the gingiva and into the bone, as Creekmore did in 19832?
DR. SUGAWARA We are aware of Creekmore's work, but screws alone have limitations because of their shape and because the bone is not thick enough in some areas. Also, after insertion, screws cannot be adjusted. The miniplates allow the clinician to adjust their positions for each patient's needs and to place them for best mechanical advantage. The disadvantage, obviously, is that the clinician must make a mucoperiosteal flap.
DR. WHITE Could the SAS miniplates and screws be made of vitallium instead of titanium?
DR. SUGAWARA Titanium miniplates and screws are frequently used in orthognathic surgery, so we were familiar with them. Although we have never used vitallium, I imagine this material could be effective. Titanium does have the character of osseointegration, and while there is limited osseointegration in the temporary period when the plates and screws are applied, the integration that does occur keeps the plates tightly against the bone. I am just not sure that vitallium plates and screws would remain as tight as the titanium ones.
DR. WHITE Have you had any infections associated with the miniplate insertions?
DR. SUGAWARA Yes, but only infrequently. Mild infections can be controlled by antiseptic mouthrinses and thorough brushing. In more severe cases we have used antibiotics, but less than 10% of the patients experience any infections. At first, we were unfamiliar with the oral hygiene requirements, and we had more infections than now. Presently, we thoroughly instruct patients in home care, and we professionally clean the plates every four weeks at their routine appointments. This regimen has greatly reduced post-surgical infections.
DR. WHITE Have any of the screws or miniplates loosened from the elastic forces?
DR. SUGAWARA Loosening sometimes occurs, but it is not from the elastic force. There are three features of the SAS placement that must be controlled to prevent movement of the miniplates: bite force, bone alignment, and implantation technique. In some of our first patients, the occlusion interfered with the miniplates, and that caused some loosening. But now we are careful to keep them separated. Also, when the bone and the miniplates have good alignment, there are fewer problems. Of course, the screws must have correct placement against the bone, but if these three requirements are met, loosening of screws will not be a problem.
DR. WHITE Most surgical procedures that correct open bites rely on intrusion of the maxillary posterior areas. Why did you elect to intrude the mandibular posterior teeth?
DR. SUGAWARA I presume you are referring to the AJO-DO article. In those illustrations, both patients exhibited skeletal Class I. There are two ways to treat Class I, depending on whether the vertical excess is in the mandible or the maxilla. If there is excess in both, we apply the SAS to both the mandible and maxilla. In cephalometric analysis of these two patients, the lower molar height was shown to be excessive, so we applied SAS in the mandible. They did not show vertical maxillary excess.
DR. WHITE Is there a special advantage to using SAS in open-bite cases?
DR. SUGAWARA There are many types of open bite. By using titanium miniplates, we can customize our treatment according to the type of problem with which we are confronted. If the problem is maxillary excess, of course we would intrude the maxillary posterior areas. Generally speaking, in Class III open bite, simultaneous lower molar intrusion and distalization is the best treatment option. In Class II, the opposite is true: simultaneous upper molar intrusion and distalization is used. In Class I, it depends on whether the upper or lower molars are excessive. The objective is to achieve a right angle between the AB line and the occlusal plane--that is, to achieve good occlusion.
DR. WHITE You used the stainless steel Multi-looped Edgewise Archwires (MEAW) developed and advocated by Dr. Kim in the United States.3 Do you use MEAW routinely in SAS cases?
DR. SUGAWARA The patient featured in the AJO article of February 1999 was a treatment we did six years ago. We were uncertain about the effectiveness of the force associated with the SAS, and we decided to use the MEAW to ensure we had maximum intrusion on the molars. We soon decided that by combining the SAS and the MEAW we had made it difficult to evaluate the SAS, so we discontinued using the MEAW after three months. We have since switched to more rigid wires and no longer use the MEAW.
DR. WHITE What size wire do you typically use now with the SAS?
DR. SUGAWARA We use .019" × .022" stainless steel wire or heat-treated Elgiloy* wire.
DR. WHITE Have you tried to intrude the posterior teeth without the benefit of a complete archwire?
DR. SUGAWARA No, because we have found it easier to control the side effects of buccal flaring by using complete wires that enable us to deliver torque to the posterior teeth.
DR. WHITE The amount of anterior bite closure you have shown with the SAS is nothing short of spectacular. What type and how much elastic intrusive force do you use to achieve this quantity of movement?
DR. SUGAWARA Measuring the magnitude of force is hard to do accurately because the distance between the circle on the miniplate and the archwire is so short. We tie an elastic thread as tightly as possible and don't concern ourselves too much with the exact magnitude of force. It could be as high as 500g at the time we place it, but that is apparently insignificant, since the force decays rapidly over the first few days and the teeth move in a predictable manner.
DR. WHITE What length of time are the elastic forces used?
DR. SUGAWARA Anywhere from six to nine months of intrusive force is enough to position the molars where they need to be. The first patient in the AJO article was treated for five months, and the molars intruded 3.5mm. The second patient achieved 5mm of molar intrusion in nine months. Treatments usually last for 18 to 24 months, and that gives a chance for the movement to stabilize, the intercuspal relationship to solidify, and the detailing and finishing procedures to be completed.
DR. WHITE How often is the elastic changed?
DR. SUGAWARA Ordinarily, we change the elastic thread every three to four weeks.
DR. WHITE How long do you leave the miniplates in after you stop using them as anchorage?
DR. SUGAWARA We leave them in place for a few months as retentive devices, and instead of elastics we attach ligatures from the teeth to the miniplates to maintain the corrected positions. Later, after retention is secure, we remove the miniplates and the screws.
DR. WHITE Although the anterior open bite closed dramatically, the anterior face height was not greatly diminished in the cases you showed. Is this a significant determinant of when and where you use the SAS?
DR. SUGAWARA Most of the patients that have a long face with a large interlabial gap have a significant reduction in anterior face height. This is not only desirable from an esthetic standpoint, but it often helps us achieve a Class I occlusion. One of the great advantages of the SAS is that it allows improvement in the anterior face height.
DR. WHITE In the second patient you showed in the AJO article, you decided not to remove the enlarged adenoids and tonsils until after orthodontic therapy. Then you decided not to do it at all because the occlusion was so good. In retrospect, do you think it would have been a good idea to remove them before treatment, just to make sure it was done?
DR. SUGAWARA Yes, the patient would have benefited from that surgery, and also from a glossectomy, since she had a large tongue. But she refused our surgical suggestions and consequently had some relapse.
DR. WHITE Have any patients experienced significant relapse with molar intrusion, anterior open bite, and/or mandibular clockwise rotation after SAS procedures?
DR. SUGAWARA There have been some modest relapses, but in our experience the SAS ordinarily produces optimal results. Remember, even surgical patients experience significant relapse from time to time. The etiology of anterior open bite is multifactorial, and the SAS treats the symptoms, not the causes. Those patients who previously displayed aberrant muscle behaviors may need myofunctional therapy.
DR. WHITE As the mandible rotates counterclockwise in response to the mandibular molar intrusion, how much mandibular incisor extrusion occurs?
DR. SUGAWARA Actually, none, but we sometimes want incisor extrusion, which we can attain by using up-and-down elastics. This also can help us achieve a firm Class I occlusion.
DR. WHITE Have you used the miniplate as anchorage for Class I or Class II elastics while retracting anterior teeth?
DR. SUGAWARA Yes, we have, and with good results.
DR. WHITE Have you used the SAS technique for intruding the maxillary molars, or for moving the molars mesially or distally?
DR. SUGAWARA Yes; I would refer you to some of the results we previously published in the Orthodontics Year Book 19974 (Figs. 4 and 5).
DR. WHITE Have you tried to simultaneously intrude maxillary and mandibular molars with the SAS?
DR. SUGAWARA Yes, we have intruded molars in both arches simultaneously, but it depends on what treatment goals we have selected for the patient.
DR. WHITE Have you tried to attach the miniplate to the zygomatic arch to obtain anchorage for movement of maxillary teeth?
DR. SUGAWARA No, because the bone of the zygomatic arch is not strong enough or large enough to sustain miniplates, and it is also too deep. We typically use the key ridge area (the zygomatic process of the maxilla) when working in the maxilla, because the bone is thick enough to carry the screws for the miniplates.
DR. WHITE Have you ever combined the SAS with extractions to treat bimaxillary protrusions?
DR. SUGAWARA No, we haven't, but it sounds like a good way to achieve maximum intraoral anchorage.
DR. WHITE Has the SAS been used to correct the horizontal discrepancies that are often found in Class II or Class III malocclusions?
DR. SUGAWARA Yes, and again I would refer you to the article in the Orthodontics Year Book.4
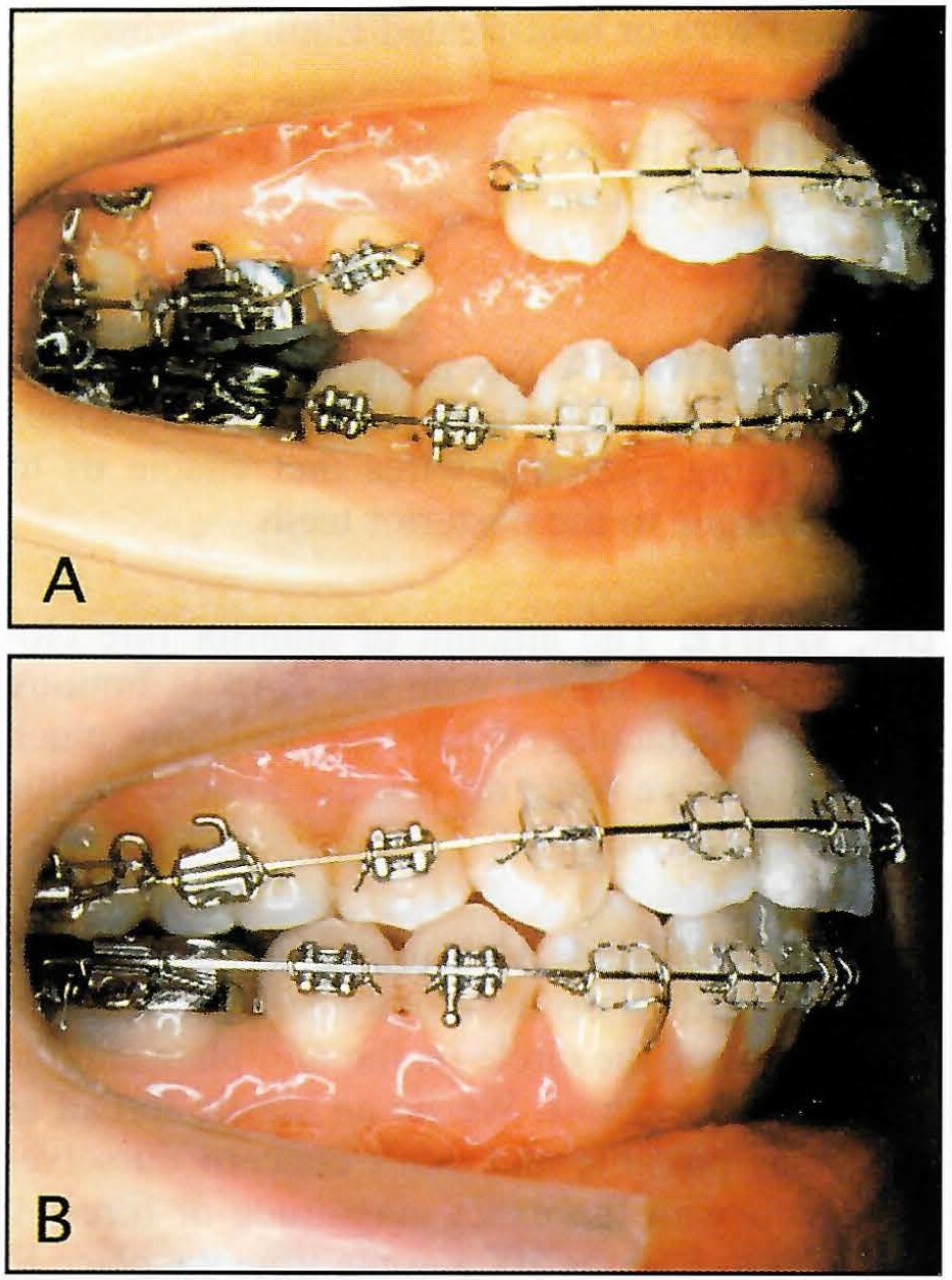
Fig. 4 Intrusion of maxillary molars using SAS. A. During intrusion of maxillary posterior segment. B. After intrusion of molars and retraction of anterior segment. (Reprinted by permission.4)
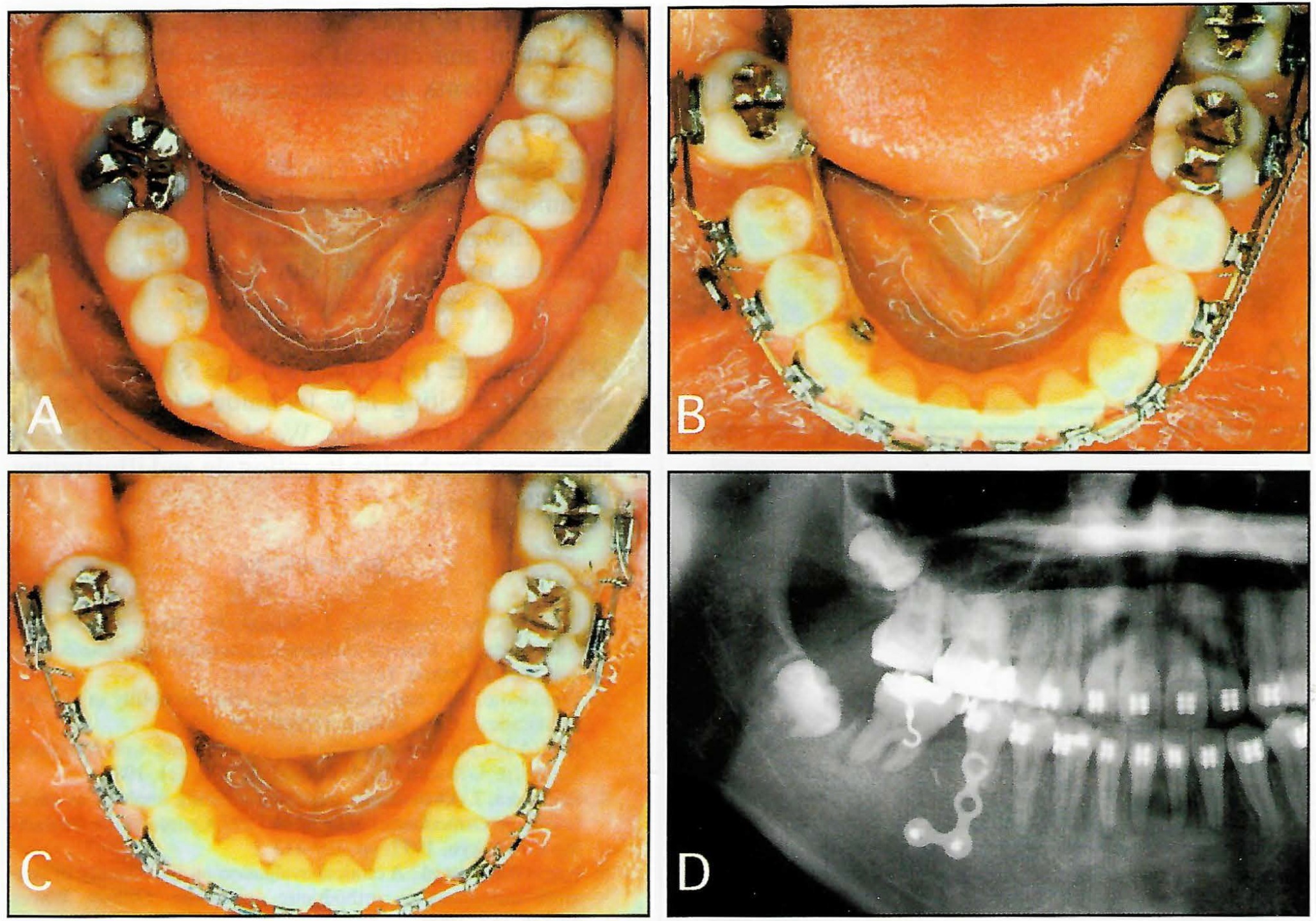
Fig. 5 Mesial movement of mandibular second molar using SAS. A. Mandibular right first molar was extracted due to ankylosis. B,D. During mesial movement of second molar. C. After mesial movement of second molar. (Reprinted by permission.4)
DR. WHITE Have any techniques been developed with the SAS to extrude posterior teeth?
DR. SUGAWARA Ordinarily, extrusion of teeth is relatively easy, but I once extruded a deeply impacted mandibular first molar by attaching a miniplate in the maxilla and using elastic force to the molar. That is the only case I have used this on. The biggest challenge for us is intrusion of molars, and that is primarily what the SAS does.
DR. WHITE Have you ever used the SAS to intrude anterior teeth, as Creekmore did in 19832?
DR. SUGAWARA Yes, we had two patients who had Class II malocclusions with deep bites and short faces. We attached the miniplates to the piriform ridge to intrude and retract the anterior teeth (Fig. 6). With traditional mechanics, extractions are usually necessary to provide space for the retraction, but by using the SAS we will be able to correctly position the dentition without removing any teeth.
DR. WHITE How would you summarize the biological and clinical advantages that the SAS offers patients in comparison to other techniques?
DR. SUGAWARA The SAS has been the only technique we have found that can consistently move molars distally or intrude them in a predictable manner. We don't need to rely on patients to use elastics or headgears.
DR. WHITE Dr. Sugawara, the SAS is one of the most exciting new techniques orthodontists have seen in some time. We at JCO would like to thank you for sharing its rationale and illustrating its multiple uses.
FOOTNOTES
- *Registered trademark of RMO, Inc., P.O. Box 17085, Denver, CO 80217.
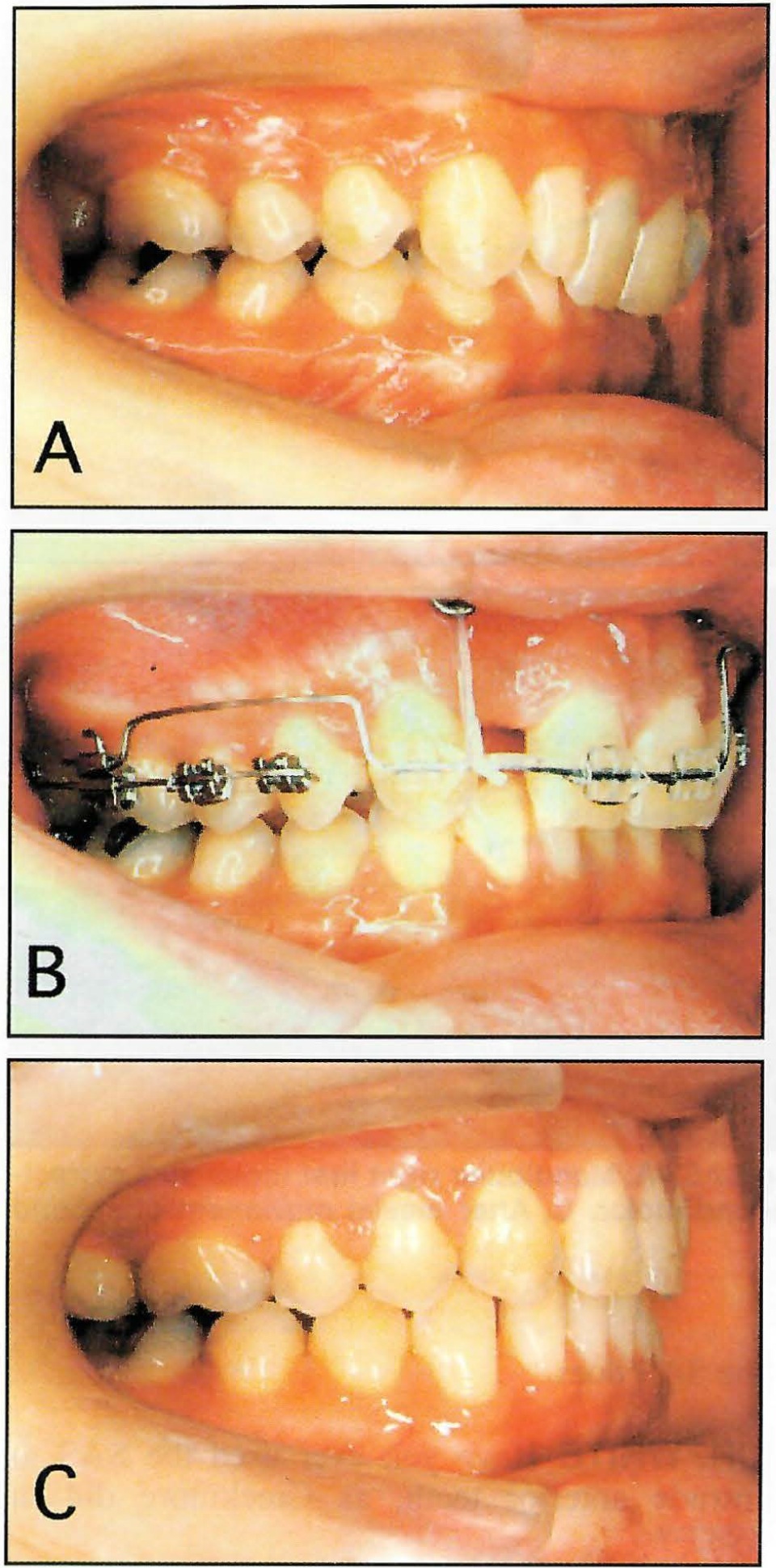
Fig. 6 Intrusion of maxillary anterior teeth using SAS. A. Before treatment. B. Intrusion of maxillary incisors after extraction of lateral incisor. C. After treatment.
REFERENCES
- 1. Umemori, M.; Sugawara, J.; Mitani, H.; Nagasaka, H.; and Kawamura, H.: Skeletal anchorage system for open-bite correction, Am. J. Orthod. 115:166-174, 1999.
- 2. Creekmore, T.D. and Eklund, M.K.: The possibility of skeletal anchorage, J. Clin. Orthod. 17:266-269, 1983.
- 3. Kim, Y.H.: Anterior openbite and its treatment with Multiloop Edgewise Archwire, Angle Orthod. 57:290-321, 1987.
- 4. Sugawara, J.: Orthodontic treatment utilizing implants as anchorages, in Orthodontics Year Book 1997, Quintessence Publishing Co., Tokyo, 1997, pp. 107-113.
- 5. Nagasaka H. et al.: A clinical evaluation on the efficacy of titanium miniplates as orthodontic anchorage, Orthod. Waves 58:136-147, 1999.
-
 DR. WHITE
DR. WHITE -
 DR. SUGAWARA
DR. SUGAWARA
Dr. Sugawara is an Associate Professor, Department of Orthodontics, School of Dentistry, Tohoku University, 4-1 Seiryo-machi, Aoba-ku, Sendai 980-77, Japan.