The Cervical Vertebrae as Maturational Indicators
Because of individual variation, physiological and anatomical maturity cannot be accurately assessed by age alone. Other parameters, such as growth velocity, secondary sex changes, dental development, and skeletal ossification, have proven of more value.1,2
The early hope of those who championed the idea of accurately determining the skeletal age of patients was to coordinate this information with orthodontic treatment so as to maximize the therapeutic effect. Unfortunately, a low correlation has been found between general skeletal maturity and facial growth as measured by common parameters.3,4
Since the presence, magnitude, and timing of facial growth have proven so unpredictable, clinicians have generally lost interest in trying to coordinate the pubertal growth spurt with orthodontic therapy. Nevertheless, the current interest in nonextraction treatment involving modification of skeletal growth seems to demand as much information as possible about patients' growth potential. Orthodontic appliances such as the Mandibular Protraction Appliance, Herbst, Frankel, bionator, and twin block, as well as cervical and high-pull headgears and protraction facemasks, will only have the desired effect in patients who have growth capability.
Similar articles from the archive:
Orthodontists do not necessarily need to know the exact skeletal age of a patient, or how much individual facial bones may grow during treatment, or even when that growth is likely to occur. They simply need to know whether the patient will grow at all during a one- or two-year treatment period and what percentage of growth can reasonably be expected during that time.
The standard method of evaluating skeletal maturity has been to use a hand-wrist x-ray to compare the bones of an individual's hand with those in published atlases.5-16 To avoid taking an additional x-ray, however, some researchers have sought to relate maturation with dental and skeletal features other than the bones in the hand and wrist.7,17-21
The use of cervical vertebrae to determine skeletal maturity is not new. In 1972, Lamparski concluded that the cervical vertebrae, as seen on routine lateral cephalograms, were as statistically and clinically reliable in assessing skeletal age as the hand-wrist technique.7 He found that the cervical vertebral indicators were the same for females and males, but that females developed the changes earlier. Other researchers have confirmed the validity of Lamparski's method of evaluating the skeletal maturity of orthodontic patients.17-19
The purpose of the present study was to determine whether the maturation of cervical vertebrae would correlate with the maturation indicated by hand-wrist x-rays in a Mexican population.
Materials and Methods
The study sample was taken from patient files of the Orthodontic Graduate Program, Universidad Autnoma de Nuevo Len, Mexico. A total of 113 patients (50 males and 63 females), age 9 to 18, had cephalometric and hand-wrist radiographs taken on the same day. None of these patients presented with congenital or acquired malformations of the cervical vertebrae or hand-wrist, nor did they have any developmental alterations due to medical syndromes or hormonal disorders.
All the radiographs were taken with the same x-ray equipment at the same distance and intensity, traced and evaluated by the same operator (Dr. Garca-Fernandez), and verified with an intra-operator error test that assessed each x-ray twice on different days.
The hand-wrist radiographs were evaluated with a system developed by Fishman,6 which uses four stages of bone maturation found at six sites located on the thumb, third finger, fifth finger, and radius (Fig. 1A). Eleven adolescent skeletal maturation indicators (SMI) are found on these six sites (Fig. 1B). The sequence of four ossification stages includes epiphyseal widening, ossification of the sesamoid of the thumb, capping of selected epiphyses over their diaphyses, and fusion of selected epiphyses and diaphyses (Fig. 1C).
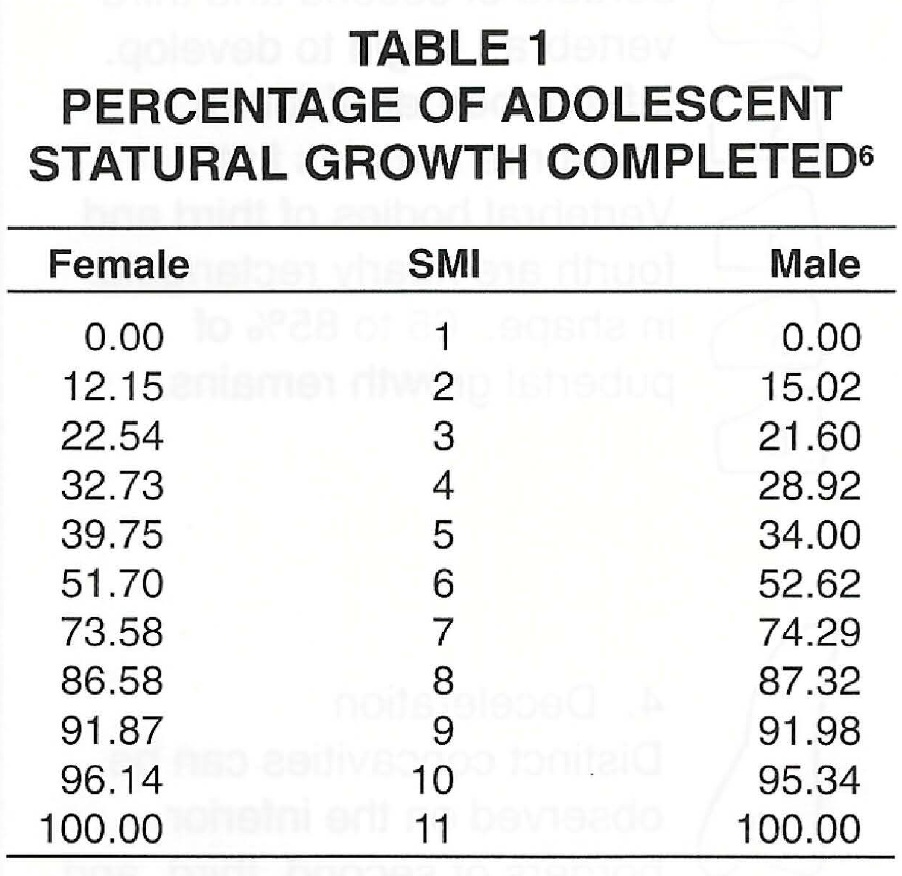
The percentage of adolescent growth completed provides a basis for interpreting the amount of skeletal growth that has occurred and for predicting future growth (Table 1). Although statural and facial growth show wide individual variations and do not proceed equally or simultaneously, there remains a direct association between the two, so that SMI have significant clinical relevance.22-24
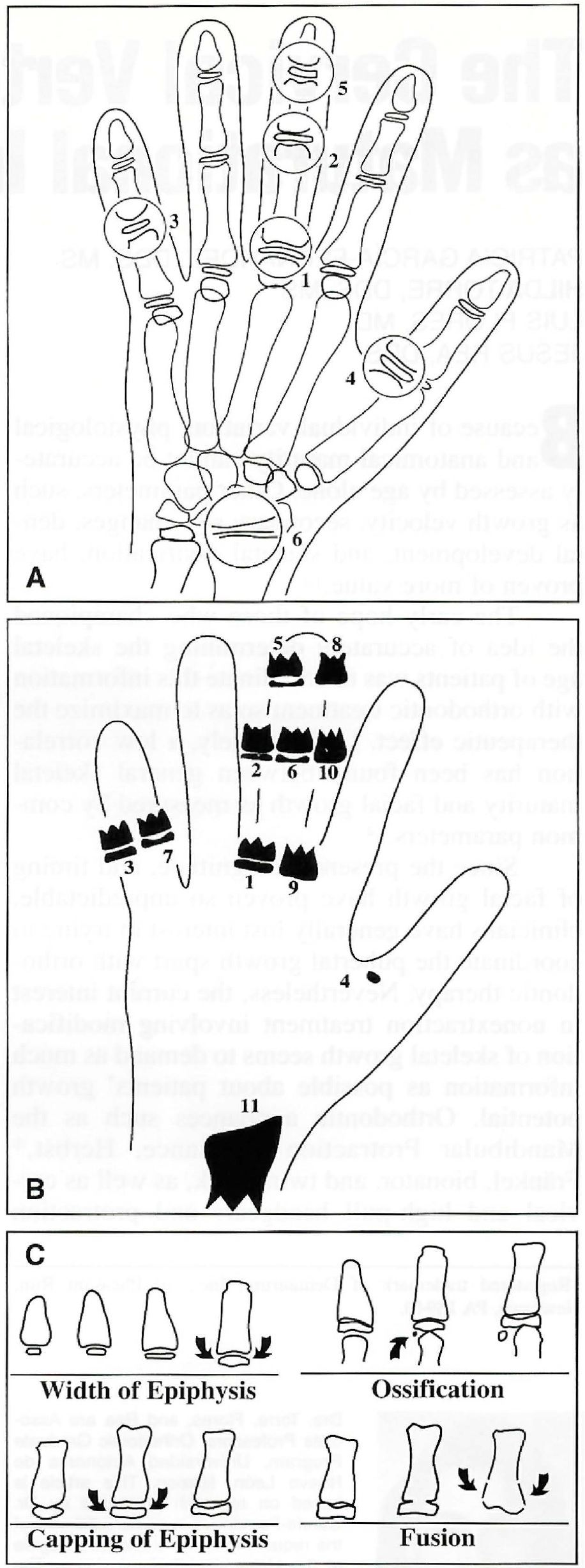
Fig. 1 A. Sites of bone maturation. B. Skeletal maturation indicators. C. Stages of ossification. (From Fishman, L.: Radiographic evaluation of skeletal maturation, a clinically oriented study based on hand-wrist films, Angle Orthod. 52:88- 112, 1982. Reprinted by permission.)
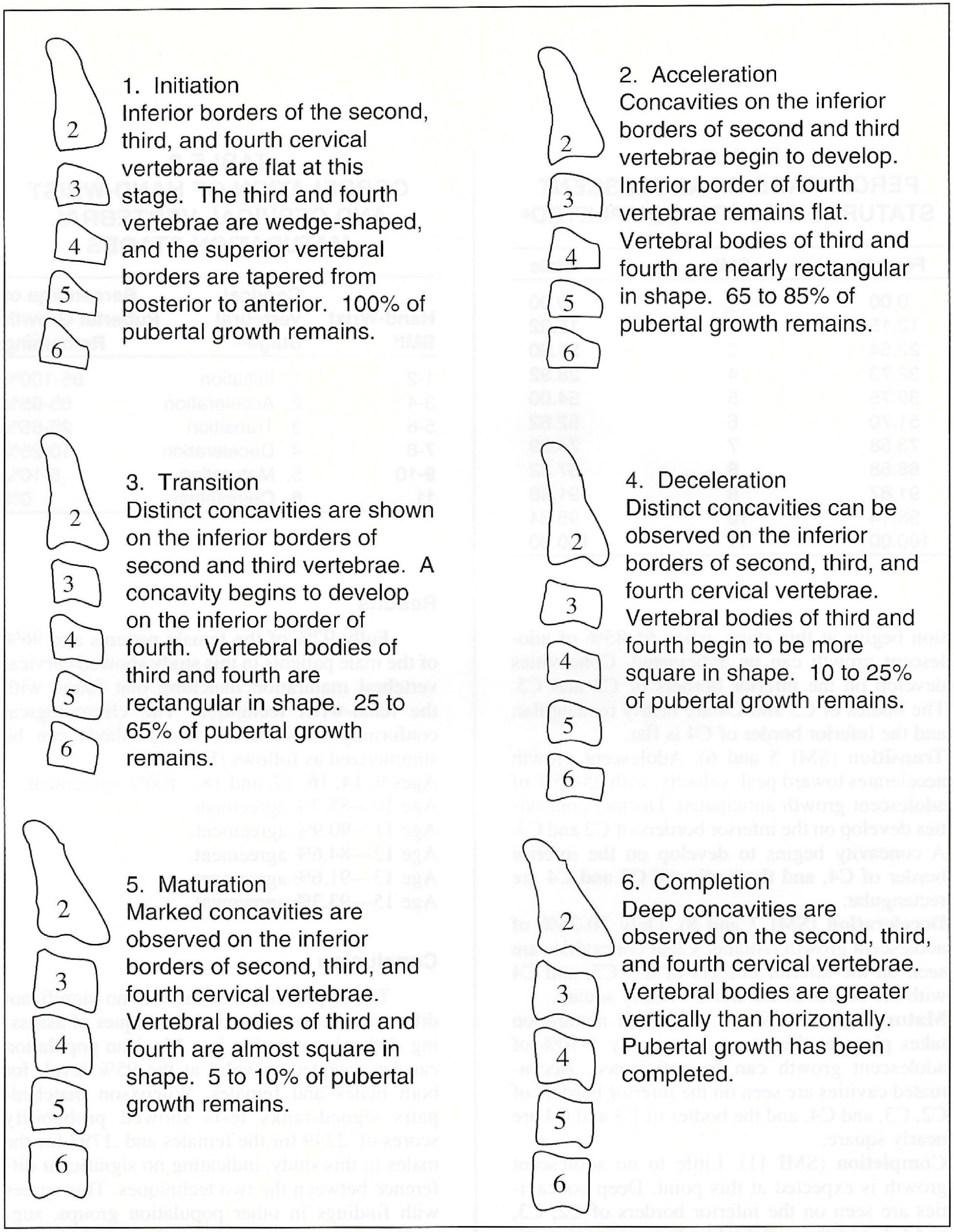
Cervical vertebral development of the sample was evaluated by the Hassel and Farman modification of Lamparski's criteria, which assesses maturational changes on the second, third, and fourth cervical vertebrae.25 Six distinct stages of growth can be related to the SMI developed by Fishman (Fig. 2, Table 2):
Initiation (SMI 1 and 2). The vertebrae are wedge-shaped, with the superior vertebral borders tapering from posterior to anterior. Eighty to 100 percent of adolescent growth can be anticipated at this stage.
Acceleration (SMI 3 and 4). Growth acceleration begins at this stage, when 65-85% of adolescent growth can be anticipated. Concavities develop on the inferior borders of C2 and C3. The bodies of C3 and C4 are nearly rectangular, and the inferior border of C4 is flat.
Transition (SMI 5 and 6). Adolescent growth accelerates toward peak velocity, with 25-65% of adolescent growth anticipated. Distinct concavities develop on the inferior borders of C2 and C3. A concavity begins to develop on the inferior border of C4, and the bodies of C3 and C4 are rectangular.
Deceleration (SMI 7 and 8). Only 10-25% of adolescent growth remains. Clear concavities are seen on the inferior borders of C2, C3, and C4 with the bodies of C3 and C4 nearly square.
Maturation (SMI 9 and 10). Final maturation takes place at this stage, when only 5-10% of adolescent growth can be anticipated. Accentuated cavities are seen on the inferior borders of C2, C3, and C4, and the bodies of C3 and C4 are nearly square.
Completion (SMI 11). Little to no adolescent growth is expected at this point. Deep concavities are seen on the inferior borders of C2, C3, and C4, and the vertebral bodies are more vertical than horizontal.
Results
Fully 92% of the female patients and 96% of the male patients in this study showed cervical vertebral maturation matching that found with the hand-wrist technique. The chronological conformity between the two methods can be summarized as follows (Fig. 3):
Ages 9, 14, 16, 17, and 18--100% agreement.
Age 10--85.7% agreement.
Age 11--90.9% agreement.
Age 12--84.6% agreement.
Age 13--91.6% agreement.
Age 15--93.3% agreement.
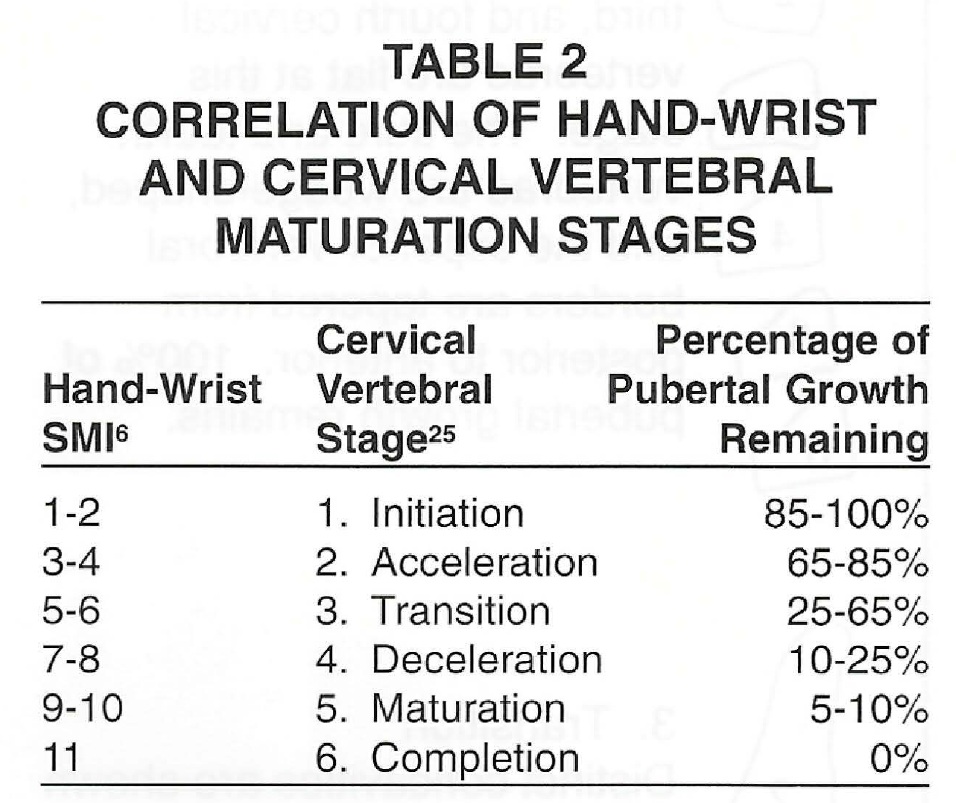
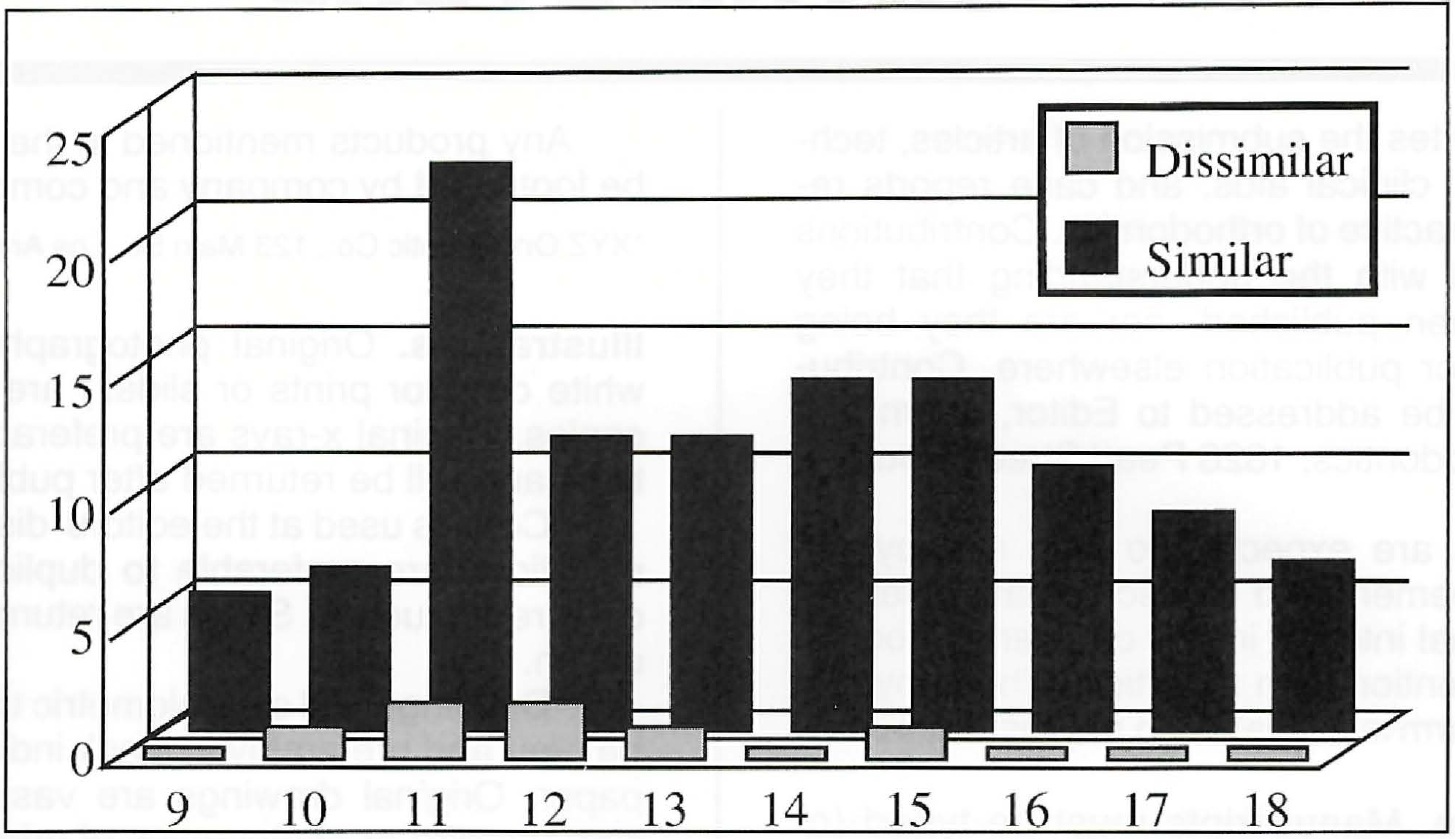
Fig. 3 Number of similar and dissimilar assessments using the hand-wrist and cervical vertebrae techniques, by patient age.
Conclusion
The hypothesis that there is no significant difference between the two techniques of assessing skeletal maturation in a Mexican population can be accepted as valid at the 95% level, for both males and females. Wilcoxson matched-pairs signed-ranks tests showed probability scores of .2249 for the females and .1797 for the males in this study, indicating no significant difference between the two techniques. This agrees with findings in other population groups, suggesting that the cervical vertebrae technique is race-neutral.
The ability to accurately appraise skeletal maturity from the cervical vertebrae, without the need for additional radiographs, has the potential to improve orthodontic diagnostic and therapeutic decisions. The technique's simplicity and ease of use should encourage more orthodontists to use this method to assess skeletal maturation.
REFERENCES
- 1. Moore, R.; Moyer, B.; and Dubois, L.: Skeletal maturation and craniofacial growth, Am. J. Orthod. 98:33-40, 1990.
- 2. Demirjian, A.; Buschang, R.; Tanguay, R.; and Patterson, K.: Interrelationships among measures of somatic, skeletal, dental and sexual maturity, Am. J. Orthod. 88:433-438, 1985.
- 3. Jamison, J.E. et al.: Longitudinal changes in the maxilla and the maxillary-mandibular relationship between 8 and 17 years of age, Am. J. Orthod. 82:217-230, 1982.
- 4. Bishara, S. et al.: Longitudinal changes in standing height and mandibular parameters between 8 and 17 years of age, Am. J. Orthod. 80:115-135, 1981.
- 5. Greulich, W. and Pyle, S.: Radiographic ossification and the adolescent growth spurt, Am. J. Orthod. 69:611-619, 1959.
- 6. Fishman, L.: Radiographic evaluation of skeletal maturation, a clinically oriented study based on hand-wrist films, Angle Orthod. 52:88-112, 1982.
- 7. Lamparski, D.: Skeletal age assessment utilizing cervical vertebrae, master's thesis, University of Pittsburgh, 1972.
- 8. Grave, K. and Brown, T.: Skeletal ossification and the adolescent growth spurt, Am. J. Orthod. 69:611-619, 1976.
- 9. Nanda, R.: The rates of growth of several facial components measured from serial cephalometric roentgenograms, Am. J. Orthod. 41:658-673, 1955.
- 10. Pileski, R.: Relationship of the ulnar sesamoid and maximum mandibular growth velocity, Angle Orthod. 43:162-170, 1973.
- 11. Mitani, H.: Comparison of mandibular growth with other variables during puberty, Angle Orthod. 62:217-222, 1992.
- 12. Hellman, M.: Ossification of epiphyseal cartilages in the hand, Am. J. Phys. Anthropol. 11:221, 1928.
- 13. Bergersen, E.: The male adolescent growth spurt: Its prediction and relation to skeletal maturation, Angle Orthod. 42:319-338, 1972.
- 14. Bjork, A. and Helm, S.: Prediction of the age of maximum pubertal growth in body height, Angle Orthod. 37:134-143, 1967.
- 15. Chapman, S.: Ossification of the adductor sesamoid and the adolescent growth spurt, Angle Orthod. 42:236-244, 1972.
- 16. Hgg, U. and Taranger, J.: Maturation indicators and the pubertal growth spurt, Am. J. Orthod. 82:299-308, 1982.
- 17. O'Reilly, M. and Yanniello, G.: Mandibular growth changes and maturation of cervical vertebrae, Angle Orthod. 58:179-184, 1988.
- 18. Hellsing, E.: Cervical vertebral dimension in 8-11 and 15 year old children, Acta Odontol. Scand. 49:207-213, 1991.
- 19. Dhillon, A.: The correlation of cervical vertebrae maturation with hand-wrist maturation and stature increments in adolescent girls, master's thesis, University of Alberta, Canada, 1993.
- 20. Chertkow, S. and Fatti, P.: The relationship between tooth mineralization and early radiographic evidence of the ulnar sesamoid, Angle Orthod. 49:282-288, 1979.
- 21. Sierra, A.: Assessment of dental and skeletal maturity: A new approach, Angle Orthod. 57:194-208, 1987.
- 22. Bambha, J.: Longitudinal cephalometric roentgenographic study of face and cranium in relation to body height, J. Am. Dent. Assoc. 63:776-799, 1971.
- 23. Johnston, F. and Hufham, H.: Skeletal maturation and cephalofacial development, Angle Orthod. 35:1-11, 1965.
- 24. Rose, J.: A cross-sectional study of the relationship of facial areas with several body dimensions, Angle Orthod. 30:6-13, 1960.
- 25. Hassel, B. and Farman, A.: Skeletal maturation evaluation using cervical vertebrae, Am. J. Orthod. 107:58-66, 1995.
-
 DR. GARCÍA-FERNANDEZ
DR. GARCÍA-FERNANDEZ -
 DR. TORRE
DR. TORRE -
DR. FLORES
-
DR. REA
Drs. Torre, Flores, and Rea are Associate Professors , Orthodontic Graduate Program, Universidad Autonoma de Nuevo Leon, Mexico. This article is based on research submitted by Dr. Garcia-Fernandez in partial fulfillment of the requirements for a master's degree at the University of Nuevo Leon. The project was supported by a grant from Consejo Nacional de Ciencia y Technologia and the Universidad Autonoma de Nuevo Leon. Dr. Garcia Fernandez's current address is Cond. Jardines Metropolitanos, Tower 1, Apt. 5E, San Juan, PR 00927.