JCO INTERVIEWS
Dr. Anthony Gianelly on Current Issues in Orthodontics
DR. WHITE Tony, you once said that orthodontics is a "six-millimeter profession". What did you mean by that?
DR. GIANELLY Under normal circumstances, the most severe problems we treat are full-cusp Class II malocclusions--indicating that the maxillary molar is approximately 5-6mm anterior to the Class I position. This means that a 5-6mm change in occlusal relations is the maximum change we produce. In this context, the results of some of the "orthopedic" studies done on monkeys, which are useful to document that orthopedic change is possible in the craniofacial complex, can't be directly applied to clinical situations for a number of reasons. One is the "end point" of the study. For example, in one monkey study, the maxillary teeth and maxilla were moved distally three premolar widths, or in human terms, 21mm. Clinically, our limit is 5-6mm; otherwise we would create an anterior crossbite. And the only changes that are relevant are those that occur in the first 5-6mm of movement.
DR. WHITE There has been a resurgence of interest lately in "orthopedic" movements for orthodontic correction. How much orthopedic adaptation is ordinarily available, and how can orthodontists rely on it for corrections?
Similar articles from the archive:
DR. GIANELLY In the transverse plane, the orthopedic change noted with rapid palatal expansion in young patients is on the order of 50% of the entire increase in arch width. In the anteroposterior direction, my view is that there is relatively little orthopedic change that occurs with conventional appliances. In the maxilla, the orthopedic change we produce with headgears or maxillary protraction appliances is at best 1-2mm--rarely more. We once placed implants in eight children who wore a headgear to the anterior part of the maxillary arch for at least 14-16 hours a day for five months. All experienced complete overjet reduction, but the implants moved in only one subject.1
Except for RPE, I don't believe that orthodontists can rely on the "orthopedic" response for correction. There's too much individual variation. An anteroposterior orthopedic response won't systematically happen because a specific stimulus is placed. If it does happen, treatment is probably simpler because there will be less dependence on tooth movement.
DR. WHITE Can functional appliances produce an orthopedic response?
DR. GIANELLY The use of functional appliances, in some studies, has produced an increase in mandibular growth on the order of 1-2mm per year. Since most clinicians use these appliances for approximately 12-16 months, any increase in total mandibular growth is small. More important, the reduction in facial convexity due to increased growth of the mandible generally doesn't exceed 1mm. For example, in the randomized clinical trial at the University of North Carolina, the SNB angle increased .5° in the control sample and 1° in the group wearing the functional appliances.2
There is an emerging view that the temporomandibular articulation can be transposed anteriorly with the use of functional appliances. The extent of this movement, its contribution to Class II correction, and its stability are not clear.
DR. WHITE Do you favor the use of appliances that require less patient cooperation, such as the Herbst*, Jasper Jumper**, Hilgers Pendulum***, Jones Jig,** and Mandibular Protrusion Appliance?
DR. GIANELLY I absolutely favor the use of these appliances, particularly those that move the maxillary molars distally. They've increased my success rate in treating patients with Class II malocclusions. If a patient with a Class II is in the late mixed dentition stage of development and conditions are favorable for a nonextraction approach, the success rate can routinely exceed 90-95%. I've had much less experience with appliances such as the Herbst and Jasper Jumper because my focus has been on moving the maxillary molars distally.
DR. WHITE Much has been said about how traditional orthodontic therapies such as the retraction of incisors, the extraction of bicuspids, and the use of headgears may cause TMD in orthodontic patients. What have you and your colleagues discovered regarding these allegations?
DR. GIANELLY My view is that orthodontic treatment of any kind is not a significant risk factor for developing TMD. In this debate, our focus has been on condylar position, since a presumed pathogenesis of TMD in extraction treatment is "distal repositioning" of the condyles due to maxillary incisor retraction during space closure. We didn't find any relationship between any type of extraction or nonextraction orthodontic treatment and condylar position. And our results have been confirmed by others. This may help explain why almost no one has been able to identify any relationship between TMD and orthodontic treatment.
DR. WHITE Treatment of TMD often seems to be governed by what Jim Ackerman called "therapeutic diagnosis"--trying a number of therapies until something works, which is not diagnosis at all. How do you feel about the way TMD complaints are routinely handled?
DR. GIANELLY I feel that most TMD complaints are handled as well as possible with today's information. Since the pathogenesis is not clear in most instances, our options are limited to trying the treatments that seem to work most often--such as discluding the teeth to relieve pain.
DR. WHITE What would you suggest to improve training in this discipline?
DR. GIANELLY More emphasis on immunology--in other words, an autoimmune possibility--and on neurology, to try to understand the basis of pain and headache better.
DR. WHITE For years, orthodontists have debated the extraction-nonextraction question without a resolution. Haven't we learned enough over the past 100 years to offer clinicians some reasonable guidance?
DR. GIANELLY This is an important question. My opinions are guided by the results of studies that I feel support the following views. One is that extraction treatment provides a better solution for crowding. A second is that lower arch dimensions are relatively inviolable. The mandibular intercanine dimension shouldn't be expanded, and arch length, including "arch development" done in the mixed dentition, shouldn't be increased more than 1mm.
DR. WHITE How do these views affect treatment strategies?
DR. GIANELLY The treatment differs depending on the developmental stage of the patient. If crowding is the chief concern, the vast majority of patients in the mixed dentition stage of development--probably 85%--can be treated by a nonextraction protocol. The space necessary to resolve the crowding can be easily gained by the preservation of the "E" space plus an increase in arch length of 1mm. Most often only "E" space preservation is necessary.
If profile considerations are superimposed on crowding conditions, extractions may be necessary. However, the tendency today is to place less emphasis on profile reduction. One reason may be that were more aware that the profile tends to flatten with age and that a slightly convex profile at 12 may be a straight profile at 21.
When crowding is present in the permanent dentition in either Class I or Class II malocclusions, extraction treatment is preferable, unless contraindicated by facial pattern and/or bite depth. Also, in treating Class II malocclusions with acceptable lower arch conditions, I may start treatment on a nonextraction basis with the intent to move molars distally. If little progress is noted, the maxillary first premolars are removed--again, unless contraindicated by facial pattern and/or bite depth.
DR. WHITE What percentage of cases do you treat with extractions?
DR. GIANELLY My percentage of extractions in the mixed dentition is low--generally no more than 10-15%--reflecting the fact that I place less emphasis on profile reduction than I did years ago. My percentage of extractions in the permanent dentition exceeds 50-60%.
DR. WHITE What factors do you feel contribute to greater stability of orthodontic treatments?
DR. GIANELLY I would list five factors: maintenance of the original lower arch dimensions, use of the original archform as the template for the final archform, long-term retention, fiberotomies for rotation corrections (particularly in the maxillary arch), and slight interproximal reduction of the lower incisors.
DR. WHITE You said that arch length shouldn't be increased by more than 1mm, yet orthodontics once again seems to be entering an era where clinicians are advocating the aggressive expansion of maxillary and mandibular arches. How do you feel about this?
DR. GIANELLY The only routine expansion I support is maxillary arch expansion in a posterior direction by moving the molars distally. I also expand the maxillary arch laterally when there is a crossbite. The lateral expansion of the maxillary arch in the mixed dentition when there is no crossbite is an enigma to me. It seems to be irrelevant, because I do not understand how it solves any problems. Take the resolution of crowding as an example. If we accept the usual convention that the lower arch is the "diagnostic" arch, lower arch crowding can be resolved in most people simply by "E" space preservation. If this is true, then crowding in the maxillary arch can also be resolved by "E" space preservation, if the molars are in a Class I position. If they are not, some distal movement of the molars, which is simple to do, can gain the space to solve the crowding. Where is the need to expand the maxilla laterally when there is no crossbite?
Mandibular arch intercanine expansion, as demonstrated many times, is not stable. Also, lower arch expansion in an anterior direction has been associated with loss of supporting tissues.3 In addition, I have not been successful moving the mandibular molars distally more than 1-2mm. With these factors in mind, I consider the dimensions of the lower arch as resistant to change and do not expand the lower arch.
DR. WHITE Currently, a lot of emphasis is being given to "first-phase treatment" or interceptive orthodontics. When do you feel orthodontists need to intervene early?
DR. GIANELLY My view is simple: except for crossbites with a shift and selected Class III malocclusions and maxillary incisor protrusions that exceed 5-6mm, I believe most problems can be treated readily in the late mixed dentition stage of development, after the eruption of the first premolars. For protrusive incisors, I retract them with a Hawley appliance for two to three months, then retain with the same Hawley. There is no evidence that early treatment provides a "better" solution.
DR. WHITE Does early treatment contribute to a shorter second phase of treatment?
DR. GIANELLY Compared to what? One-phase treatment has only one phase. In two-phase treatment, total treatment time is longer.
DR. WHITE How important and how accurate do you find cephalometric growth forecasting?
DR. GIANELLY The accuracy of cephalometric forecasting may depend on the point of view. Scientifically, it appears to be no more accurate than adding the average increment to most dimensions as they move along selected directions, because the variability of the growth change is often bigger than the change itself. Some grow more than anticipated; others grow less. On the other hand, it can present a general view of the future, since the patient's facial pattern--which reflects the previous growth of the patient--is the template, and only the last part of growth is the forecast. The forecast may be more important for the patient to obtain a general view of a possible outcome. For example, incisor retraction is most often followed by upper lip retraction, and this would be a graphic way to demonstrate that to a patient. The precise location of the lip would be difficult to forecast.
DR. WHITE How do you see the future role of magnets in Class II treatment?
DR. GIANELLY Our experience with magnets was in moving molars distally, and in this area, they worked very well. However, they have been supplanted by NiTi coils and wires. At present, my view is that magnets will be used mainly to intrude posterior teeth in vertical dysplasias.
DR. WHITE You also did some early studies with thermal titanium wires. What advantages do these have compared with ordinary titanium wires?
DR. GIANELLY The thermal titanium wires, particularly if cooled, are easier to insert and have a greater range of action. In my experience, patients seem more comfortable.
DR. WHITE What role do you see for implantology in orthodontics?
DR. GIANELLY Implantology will have an important role. My focus is on the "onplants" developed by Block and Hoffman,4 which are presumably simple to place and recover (Fig. 1). They will expand our horizons to allow us to produce pure orthopedics (such as maxillary protraction) and will serve as anchorage. Success rates in Class II nonextraction treatment can then approach 100%.
DR. WHITE Along with Schudy, you have advocated the use of different-size brackets within the same arch. What clinical advantages have you found with this approach?
DR. GIANELLY The reason I did this was to combine precision with practicality. For example, one movement that requires torque control is the retraction of the maxillary incisors. In the edgewise technique, full engagement of the wire in the incisor brackets is generally necessary to control the axial inclination of the incisors during retraction. I use an .018" X .025" vertically slotted, programmed bracket on the central and lateral incisors and an .022" X .028" vertically slotted bracket posteriorly (Fig. 2). For retraction, I simply insert an .018" X .022" wire for full engagement of the incisor brackets and retract the incisors bodily by means of sliding mechanics, because the wire is "undersized" in the buccal segments. According to a New York University study, only 7% of wires "fill the slots".5 My percentage during incisor retraction approaches 100%. The undersized posterior part of the wire also relieves me of the technical burden of adjusting the torque to the posterior brackets. My chairtime is reduced, and I don't have to contend with loops that may impinge on the tissues.
To cite another example, one of the more difficult conditions to solve in everyday orthodontics is preservation of lower incisor anchorage during space closure in extraction treatment. The only intra-arch system that I know is to apply a moment to the incisors. We place an .018" X .022" wire with labial crown torque in the incisor brackets (Fig. 3). This is technically simple, since the undersized wire in the buccal segments is "detorqued" to its neutral orientation because there is no need to adjust the torque in the wire to the brackets. A closing coil or elastic will slide the posterior teeth forward on the undersized wire while the torque on the incisors controls incisor position. I also insert uprighting springs in the vertical slots on the canine brackets to enhance the incisor anchorage. With the use of Class II elastics, lingual crown torque is placed on the lower incisor region for anchorage control. When torque control is required in the buccal segments, the .018" X .022" wire is rotated 90° to create an .022" X .018" section for full bracket engagement (Fig. 4).
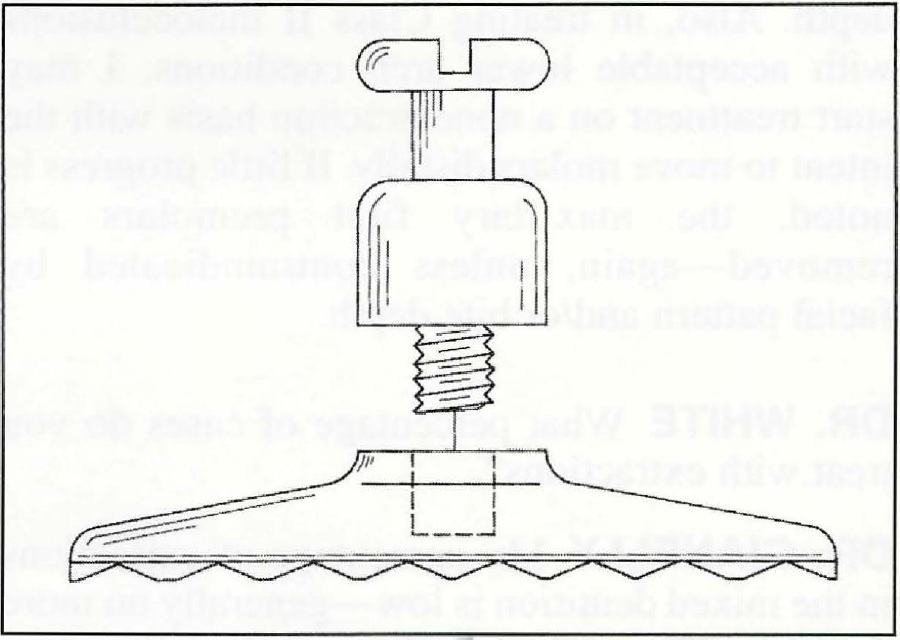
Fig. 1 Onplant with internal thread for placement of transgingival abutment. Abutment shown is designed to receive .051" wire (reprinted by permission4).
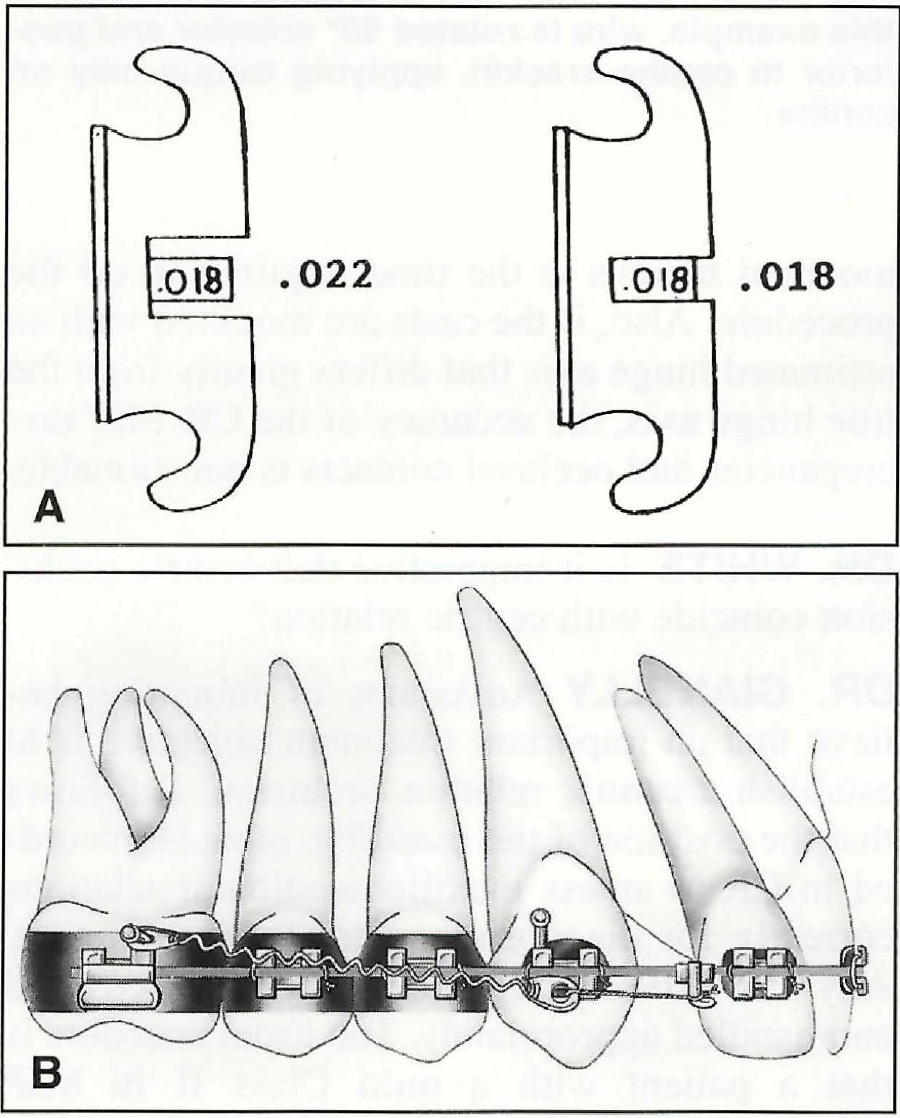
Fig. 2 A. On central and lateral incisors {right), vertically slotted brackets are .018" x .025". On canines, bicuspids, and molars (left), vertically slotted brackets are .022" x .028". The .018" x .022" rectangular wire "fills" slots of incisor brackets, but is undersized in canine and bicuspid brackets and molar tubes. B. Sliding mechanics using .018" x .022" stainless steel wire. Since rectangular wire "fills" slots of incisor brackets, they are retracted bodily as undersized wire slides through brackets and tubes in buccal segments.
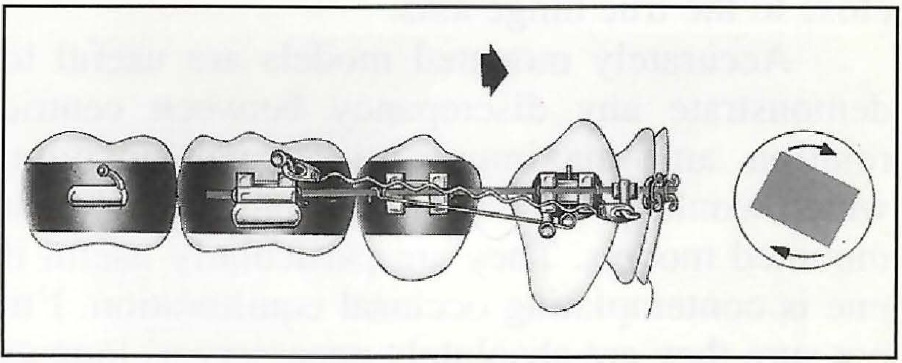
Fig. 3 Lower incisor anchorage maintained using .018" x .022" stainless steel wire with labial crown torque in incisor segment and uprighting springs in vertical slots of canines. Since wire is undersized in buccal segments, posterior teeth slide anteriorly.
DR. WHITE You have written about an indirect bonding technique. Do you normally rely on this method?
DR. GIANELLY I am a definite advocate of an indirect technique. One of the most common and universal problems that I've seen is incorrect appliance placement, with consequences such as the creation of lateral open bites and marginal-ridge discrepancies. The main advantage of an indirect technique is that it reduces errors in appliance placement. The disadvantage is that it is more time-consuming.
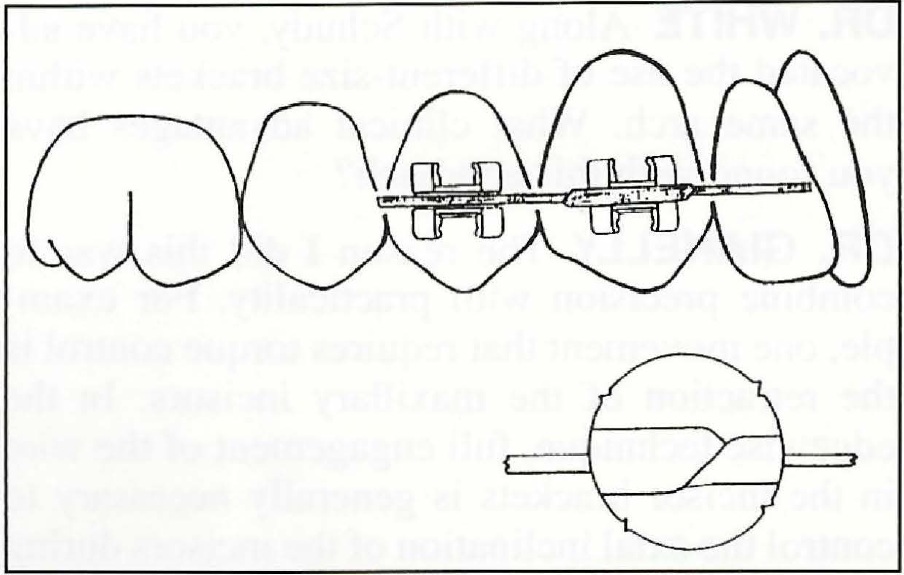
Fig. 4 To place torque on posterior teeth, .018" x .022" stainless steel wire is rotated 90 degrees where torque is needed, thus creating an area of .022" x .018" wire that "fills" slot of posterior bracket. In this example, wire is rotated 90 degrees anterior and posterior to canine bracket, applying torque only on canine.
DR. WHITE Several clinicians advocate the mounting of orthodontic study models on adjustable articulators. How accurate and useful is this?
DR. GIANELLY We use the SAM II†articulator. With a facebow oriented to the hinge axis to transfer the maxillary cast to the articulator, the mounting procedure is reasonably accurate. We can routinely reproduce the occlusal contacts noted intraorally on the articulated models. However, the ability to simulate the hinge-axis border movement of the patient depends on the ability to capture an estimated hinge axis that is close to the true hinge axis.
Accurately mounted models are useful to demonstrate any discrepancy between centric relation and maximum intercuspal position, which would be difficult to demonstrate without mounted models. They are particularly useful if one is contemplating occlusal equilibration. I'm not sure they are absolutely necessary as long as conventional study models are related according to a CR registration. The main disadvantage to mounted models is the time required to do the procedure. Also, if the casts are mounted with an estimated hinge axis that differs greatly from the true hinge axis, the accuracy of the CR-MIP discrepancies and occlusal contacts is questionable.
DR. WHITE Is it imperative that centric occlusion coincide with centric relation?
DR. GIANELLY Advocates of mounting believe that an important treatment objective is to establish a centric relation occlusion. It follows that the position of the mandible must be recorded in CR to assess maxillomandibular relations correctly for diagnosis and treatment planning. Any CR-MIP discrepancies can be discovered and handled appropriately. The usual anecdote is that a patient with a mild Class II in MIP becomes a surgical patient in CR.
I believe we should try to establish a centric relation occlusion, or at least keep the CR-MIP discrepancy to as little as possible--preferably to less than 1mm--for a number of reasons. The results of one study indicated that large CR-MIP discrepancies (greater than 4mm) substantially increase the risk of developing TMD.6 Also, in an asymptomatic group, no individual had a CR-MIP discrepancy greater than 2mm.6 In addition, a CR-MIP discrepancy has been related to post-treatment lower incisor crowding.7
DR. WHITE How important to the health and function of the stomatognathic system is a cuspid rise?
DR. GIANELLY Pullinger and Seligman reviewed the literature and concluded that an occlusal scheme with a cuspid rise offered no distinct advantage.8 However, I believe that cuspid rise should be a treatment objective, based on Williamson's findings that disclusion of the posterior teeth during excursions reduces the muscle activity of the power muscles.9 It makes sense that the power muscles shouldn't contract too forcefully when the condyle is not in the fossa.
DR. WHITE What is your opinion about the relationship of muscle balance and masticatory function?
DR. GIANELLY Muscle considerations are extremely important. Yet I can't be more precise, because our level of understanding of the relationship between muscle "balance" and masticatory function is not advanced to the point that we can assess muscle function well, except in gross terms. There is no pure muscle "balance"--in other words, lingual and labial forces that are equal, so that the net force is zero. Also, the ability of muscles to adapt to changing conditions--how it occurs, what are the limits--is not well understood.
DR. WHITE As a dental educator, what concepts and techniques have you found most difficult for students to grasp?
DR. GIANELLY The most challenging concepts are those concerning biomechanics--moments, forces, moment-to-force ratios. The most difficult technical exercise is the three-dimensional control of a rectangular wire. The most difficult clinical situation is the grasp of space management in extraction treatment, because teeth are moving in all four quadrants, and reference points to determine what should move are sometimes obscure. The most challenging clinical problem I see for orthodontists in general is the management of vertical dysplasias, particularly hyperdivergent facial patterns associated with an open bite. The margin of error in correcting these problems is, at times, slim to nonexistent.
DR. WHITE How could dental colleges improve their undergraduate programs in orthodontics?
DR. GIANELLY The main thrust would be more clinical exposure. The didactic level of education appears adequate.
DR. WHITE What about postgraduate orthodontic programs?
DR. GIANELLY I would emphasize more critical thinking--more emphasis on "outcomes-based" information and independent research. I'd also like to see more interdisciplinary contact, residents finishing treatment of patients they have started, and retention clinics.
DR. WHITE Does a three-year postgraduate curriculum offer advantages over two-year programs?
DR. GIANELLY There are definite advantages to a three-year program. One is the ability of residents to finish patients they have started, and this would enhance the education process. A second is that research can be done more carefully and completely. A third is that a resident can participate more fully in an area of interest such as TMD or orthognathic surgery.
DR. WHITE What do you see as the future of orthodontic therapy?
DR. GIANELLY I see a bright future for orthodontic treatment, because success rates for most conditions can be increased. One of the most perplexing problems we face is cooperation. Non-cooperation-based systems, including the use of "onplants" for anchorage control, can and will enhance our capabilities.
We're also learning more about the biology of tooth movement, and this may help us learn to control the tissue reactions to our advantage, to enhance the rates of movements or to control anchorage pharmacologically. This is probably the most promising method to shorten treatment time. Unfortunately, it will be some time before it will be practical. I don't see anything on the immediate horizon that will shorten treatment.
DR. WHITE Tony, thank you for sharing your insights and experience with our readers.
FOOTNOTES
- *Registered trademark of Dentaurum, Inc., 10 Pheasant Run, Newtown, PA 18940.
- **Trademark of American Orthodontics, 1714 Cambridge Ave., Sheboygan, WI 53082.
- ***Ormco, 1717 W. Collins Ave., Orange, CA 92667.
- †Great Lakes Orthodontics, Ltd., 199 Fire Tower Drive, Tonawanda, NY 14150.
REFERENCES
- 1. Bernstein, L.; Ulbrich, R.; and Gianelly, A.A.: Orthopedics versus orthodontics in Class II treatment: An implant study, Am. J. Orthod. 72:549-559, 1977.
- 2. Tulloch, J.F.C. ; Phillips, C.; and Proffit, W.R.: Early versus late treatment of Class II malocclusions: Preliminary results from the UNC clinical trial, in Orthodontic Treatment: Outcomes and Effectiveness, ed. C. Trotman and J.A. McNamara, Jr., Center for Human Growth and Development, University of Michigan, Ann Arbor, 1995, pp. 113-138.
- 3. Artun, J. and Krogstad, 0.: Periodontal status of mandibular incisors following excessive proclination, Am. J. Orthod. 91 :225-232, 1987.
- 4. Block, M.S. and Hoffman, D.R. : A new device for absolute anchorage for orthodontics, Am. J. Orthod. 107:25 l -258, 1995.
- 5. Angelakis, R. : Feasibility and design of the preadjusted appliance, thesis, New York University, 1994.
- 6. Pullinger, A.G.; Seligman, D.A.; and Gornbein, J.A.: A multiple logistic analysis of the risk and relative odds of temporomandibular disorders of common occlusal features, J. Dent. Res. 72:968-979.
- 7. Weiland, F.J.: The role of occlusal discrepancies in the long term stability of the mandibular arch, Eur. J. Orthod. 16:521-529, 1994.
- 8. Seligman, D.A. and Pullinger, A.G.: The role of functional occlusal relationships in temporomandibular disorders: A review, J. Craniomand. Disord. Fae. Oral Pain 5:265-279, 1991.
- 9. Williamson, E.H. : JCO Interviews on occlusion and TMJ dysfunction, J. Clin. Orthod. 15:333-350, 1981.
-
 DR. WHITE
DR. WHITE -
 DR. GIANELLY
DR. GIANELLY
Dr. White is the Editor of the Journal of Clinical Orthodontics. Dr. Gianelly is Professor and Chairman, Department of Orthodontics, Goldman School of Graduate Dentistry, Boston University, 100 E. Newton St., Boston, MA 02118.