JCO INTERVIEWS
Craig Andreiko, DDS, MS, on the Elan and Orthos Systems
DR. WHITE What are Elan and Orthos?
DR. ANDREIKO They are two new appliance systems that represent the first time modern CAD/CAM [computer-aided design/computer-aided manufacturing] technology has been applied to both human anatomy and appliance design in the orthodontic field.
DR. WHITE Could you describe Elan more completely?
DR. ANDREIKO Elan* is a new dimension in treatment planning. Over the years, treatment planning and appliances have evolved to more completely address the individuality of the patient. Computers now aid in the cephalometric evaluation of the patient and in previewing the anticipated results. Appliances exist that are designed for extraction, nonextraction, expansion, etc. Elan is the first system to integrate the treatment plan and the appliance for a specific patient.
Elan begins with digitizing the skeletal and dental entity of the patient. The system then proceeds to design an occlusion, based on the practitioner's treatment plan and on algorithms developed to mate the three-dimensional positioning of the dentition to the skeletal framework. Next, the system designs and fabricates brackets, wires, and bracket-positioning devices that are essentially reverse-engineered from the desired final results for that individual patient.
Similar articles from the archive:
It is an evolution of preadjusted appliances. Since the system can capture the "personality" of the practitioner and match this to the individual patient, it is essentially the same appliance he or she is now using, with much more of the guesswork eliminated. This system allows the practitioner to concentrate more on treatment planning and less on adjusting for the mismatch between the appliance and the patient. As Ricketts said, "Begin with the end in mind."
DR. WHITE And Orthos?
DR. ANDREIKO [Orthos* is a new average prescription and appliance design based on computer analysis of more than 100 cases derived from the Elan technology. It is a coordinated system of brackets, buccal tubes, and wires.
DR. WHITE With the Elan system, how do you establish individual treatment needs such as tip, torque, and in-out positioning for patients?
DR. ANDREIKO The Elan system begins with an analysis to determine the medullary center of the mandibular bone. This is converted to a mathematical equation we call Mantrough (Fig. 1)--the keystone of the analysis.
Next, the mandibular teeth are placed on the curve such that the crown long axes are at specified inclinations, as opposed to the facial inclinations that have been used to date. The centric stops (buccal cusps) of these teeth are aligned on another smooth equation derived from Mantrough, such that the roots of the teeth are centered in the bone. The maxillary teeth are then placed in occlusion with the already-set mandibular teeth. Maxillary posterior teeth are placed with respect to centric stops and calculations for molar rotation (Fig. 2). The maxillary anterior teeth are placed from calculations to provide either group function or cuspid rise parameters. Other calculations regarding tooth-size discrepancies, depth of bite, etc., are also done at this time. Essentially, the system does an ideal setup for each case.
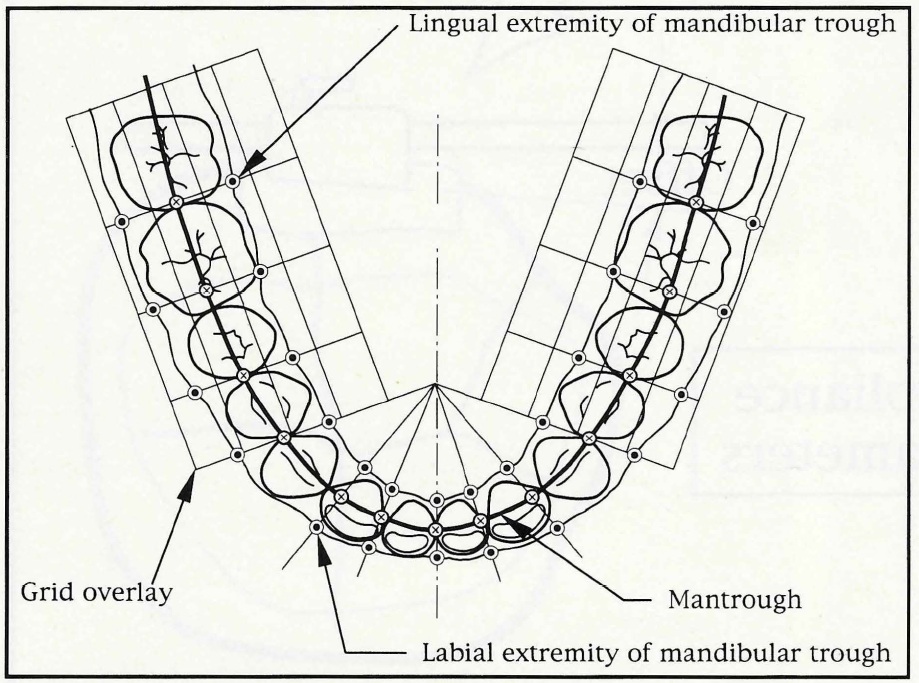
Fig. 1 Development of Mantrough, with grid overlay used for selection of lingual and labial limits.
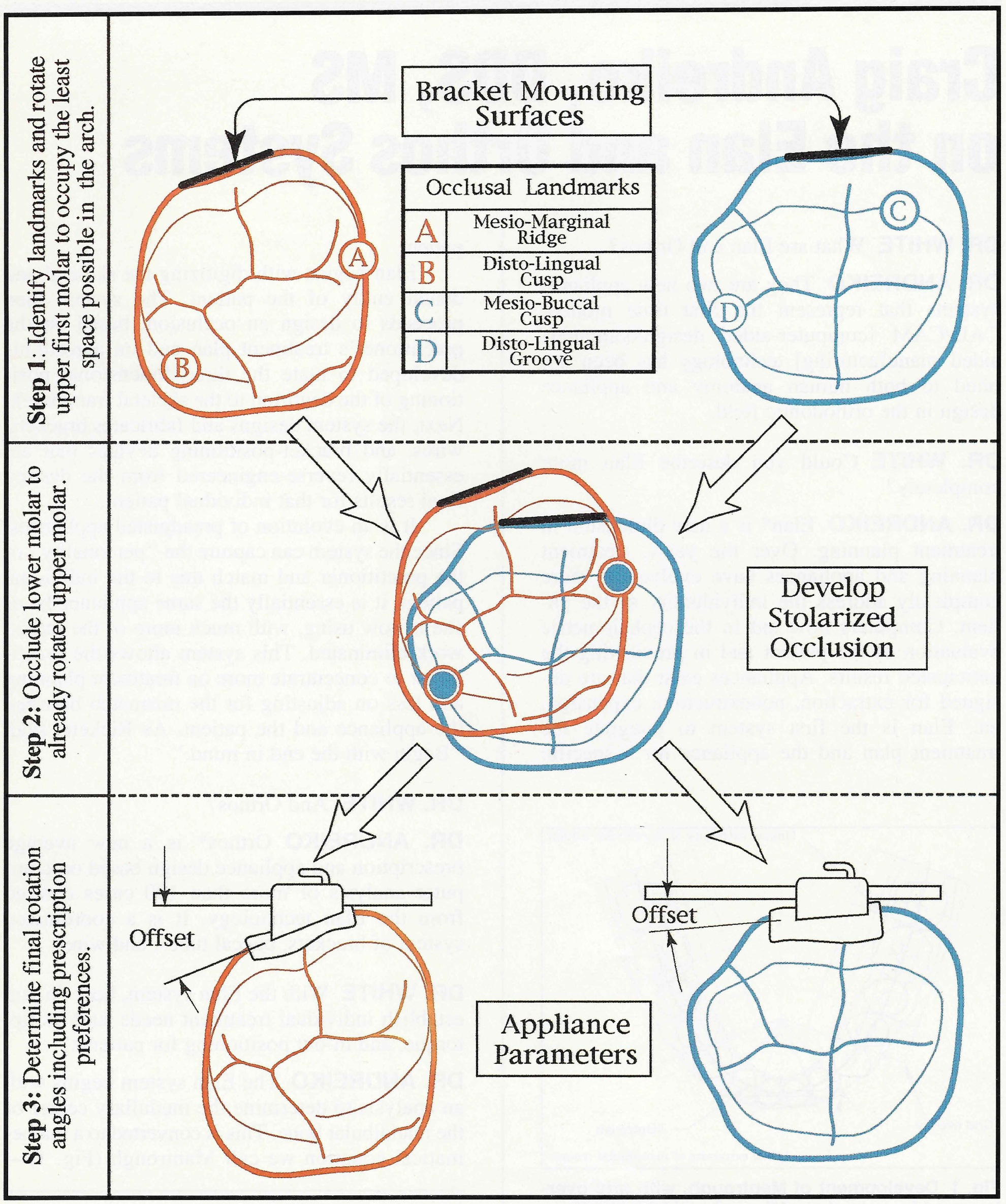
Fig. 2 Explanation of logic used to determine molar rotation angles.
DR. WHITE How does the crown long axis differ from the system of measurements Andrews gave us 30 years ago?
DR. ANDREIKO The crown long axis is a line that passes through points of bisection of the incisal edge and the cervix of the tooth, as seen from a mesiodistal profile (Fig. 3). The system works more off the body of the tooth, essentially, but also utilizes specific occlusal landmarks to more accurately control root positioning. Until something like computed tomography or magnetic resonance imaging becomes practical and accurate, I think this is the best that can be done.
DR. WHITE How precise must the appliance be to achieve clinical accuracy?
DR. ANDREIKO The system resolves to about .002" fundamentally, but tolerances can accumulate, and so our goal is to produce occlusions that the practitioner has no desire to adjust through bending the archwire. I think that our advantage here is that the system can view the occlusion from the lingual as well as the labial.
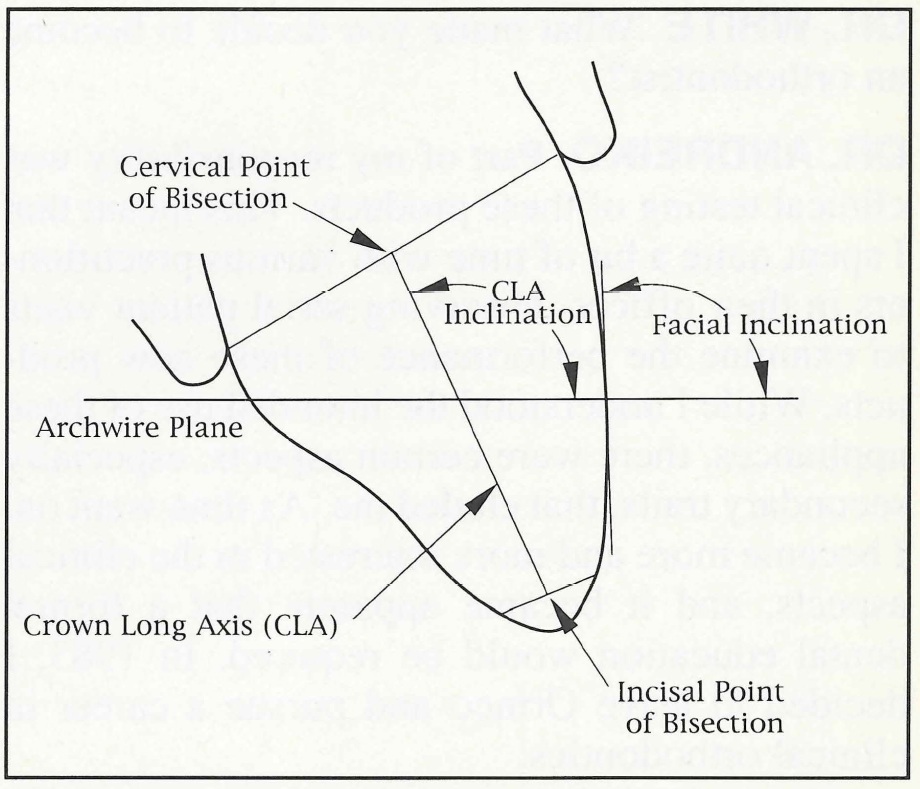
Fig. 3 Derivation of crown long axis, and its relationship to facial inclination.
DR. WHITE Where do you place the brackets in the Elan system?
DR. ANDREIKO Mandibular brackets are placed as occlusally as possible for hygiene while assuring clearance from the buccal cusps of the maxillary teeth in the final occlusion. The maxillary brackets are placed fairly centrally, due to the absence of interferences.
DR. WHITE Presuming you can manufacture such accurate brackets and archwires, how can you assure correct placement on the teeth?
DR. ANDREIKO We have developed a single-tooth indirect procedure that will reliably allow the bracket or tube to be placed in the design location. The locating device is constructed on numerically controlled machinery and is not a laboratory procedure.
DR. WHITE I know from our previous conversations that you have a unique background for an orthodontist. Would you describe your experience for our readers?
DR. ANDREIKO I was introduced to orthodontics as an apprentice tool and die maker at Ormco in 1971. Over the next five years, I progressed through a series of engineering and R&D positions. In 1975, working as a senior project engineer at Ormco, I began designing orthodontic appliances. I developed many products that are now familiar to most orthodontists. Among these are the foil-mesh bonding pads now used by most, as well as braided rectangular wires, brazing technology for assembly of appliances, the metallurgy responsible for today's down-sized appliances, and Ormco's lingual orthodontic system.
DR. WHITE What made you decide to become an orthodontist?
DR. ANDREIKO Part of my responsibility was clinical testing of these products. This meant that I spent quite a bit of time with various practitioners in their offices, observing serial patient visits to examine the performance of these new products. While I understood the intended use of these appliances, there were certain aspects, especially secondary traits, that eluded me. As time went on, I became more and more interested in the clinical aspects, and it became apparent that a formal dental education would be required. In 1983, I decided to leave Ormco and pursue a career in clinical orthodontics.
I graduated from the Loma Linda University general dental program in 1988 and from the orthodontic specialty program in 1991. I will shortly begin treating a limited number of patients as soon as Ormco completes an operatory on the premises. I am also a part-time clinical and didactic instructor at Loma Linda University.
DR. WHITE Was your introduction to orthodontic mechanotherapy via preadjusted appliances, classical edgewise appliances, or a combination of techniques?
DR. ANDREIKO Because of my position at Ormco, I had experience with almost every technique, including Begg. However, the bulk of my experience was with banded Tweed mechanics and later with bonded preadjusted appliance techniques. Of course, the training I received at Loma Linda was based on Bioprogressive principles.
DR. WHITE What were some of the problems you saw with the preadjusted orthodontic appliance?
DR. ANDREIKO In studying dental anatomy to design various appliances, I was impressed with the human variability relative to the geometry required in the appliances. I think this was compounded by the fact that the appliances had to be positioned on the faces of the teeth, which, from an engineer's point of view, is a limitation. Archform and coordination of the mandibular and maxillary archwires was also a difficult parameter to manage.
Positioning of the brackets and tubes was more of an art than a science. In particular, mandibular appliances are often placed more gingivally than the design location, due to a combination of maxillary cusp interference and appliance size. This causes excessive lingual tipping of the crowns and discrepancies in the 1st-order relationships.
The precision of a high-quality finished occlusion relative to the variation found in the patient population was incongruous with a "one size fits all" approach. I believe that this is a key reason many orthodontists do not use full-size wires. It would seem that a full-size wire is a requirement for the bracket prescription to express its geometry on the occlusion.
DR. WHITE If present preadjusted appliances are so inaccurate, how do you explain the excellent results so many orthodontists achieve?
DR. ANDREIKO Excellent results have been the hallmark of orthodontics. What has happened is that the time and effort required to produce quality results have been reduced. This can be seen in the increased availability of treatment to the public. I also believe that the number of people receiving treatment is going to grow more than just significantly in the ensuing years, and that the orthodontic community must prepare for these increased caseloads.
DR. WHITE With the Elan system, will it be necessary to fill the bracket with wire throughout treatment to fully exploit its potential?
DR. ANDREIKO In certain malocclusions, treatment can be accomplished with round wires. These cases could be treated with undersize wires, just as is now possible. However, filling the slot will provide better detail. In reality, filling the slot should become the preferred mode of treatment with the "accurized" appliance and the newer wire alloys. It seems that the finishing phase may utilize a full-size archwire initially, but the final phase might be done with a smaller wire to facilitate minor detailing and settling of the occlusion.
DR. WHITE If few orthodontists using preadjusted appliances today completely fill the brackets with wire, why would you expect them to use full-size wires with the Elan system?
DR. ANDREIKO Appliances have been designed in the past to allow the practitioner to overcorrect or overcome the clinical side effects of treatment by utilizing the wire size as a tool. Elan systems can provide any overcorrections or clinical side effects, such as additional inclination of incisors in extraction cases, in the slot geometry. Secondly, the smaller wire has allowed the teeth to find an occlusal position through the forces of occlusion when the appliance would have done otherwise. This is less of a concern with individualized appliances.
DR. WHITE As with any preadjusted system, you expect the brackets to effect rotations and vertical positions of the teeth, but what effect does the appliance have on the horizontal relationship between the jaws?
DR. ANDREIKO By more accurately controlling the axial positioning of the mandibular posterior teeth with fill-the-slot mechanics, the width of the arch is more precisely regulated. So while there are no inherent changes in arch width, the cases tend to have more upright mandibular posterior segments, and this leads to a slightly wider arch in some cases.
DR. WHITE What modifications must be made for bicuspid extraction patients or for those with mutilated dentitions?
DR. ANDREIKO This system can help in extraction decisions by accurately determining crowding and tooth-size discrepancies. TSD calculations have lacked reliability due to many factors that are not currently included in other calculations, such as arch form and tooth thickness. The system can, for instance, give additional input to the clinician regarding minimizing tooth-size discrepancies based on which teeth are to be extracted before an irreversible treatment plan is instituted. The archwire sequence would depend on the amount of space to close and the practitioner's preference, but I really don't see Elan changing the retraction wire selection very much.
Mutilated occlusions can be analyzed with respect to anticipated restorative dentistry or made to fit as well as can be done within the existing anatomy and software. To be honest, most of our cases have involved minimal restorative work to date.
DR. WHITE What types of wires do you envision using with the Elan system?
DR. ANDREIKO Virtually all types, with an emphasis on the new alloys.
DR. WHITE Can any generic archwire be used?
DR. ANDREIKO That would be a poor use of the system, since the brackets and archwires are an integral design to produce truly coordinated dental arches for that one patient. The appliances are like snowflakes in that they appear similar, yet no two have ever been the same. The system coordinates literally hundreds of parameters in each case.
DR. WHITE How do you plan to make the wires available to the orthodontist? Will you supply a full series of archwires at the beginning of treatment, or ship them on an as-needed basis?
DR. ANDREIKO Archwires will be ordered according to treatment plan when the case is sent in, but wires can be fabricated from the data base at any time (templates would be included anyway). Of course, finishing archwires would be provided with every case. I believe that coordinated archforms should be a part of treatment from the beginning, but I also think that they are indispensable at the finishing stage.
DR. WHITE Could you use the custom-made archwires with an ordinary set of preadjusted brackets?
DR. ANDREIKO I think not, for the same reason as above.
DR. WHITE Will the Elan brackets be available in twin, single, or both?
DR. ANDREIKO Currently, the system is available only in the twin configuration, but we have longer-term plans to encompass all techniques, including ceramic and plastic appliances.
DR. WHITE Isn't a twin-bracket system less efficient than a single-bracket system that offers greater interbracket distance?
DR. ANDREIKO Practitioners have devised treatment mechanics that function well with both bracket systems. With the new wires, the difference is blurred slightly in some aspects, and the twin bracket systems are still the most popular today.
DR. WHITE What will the slot size be?
DR. ANDREIKO Both .018" and .022" slots are supported currently. I have to say that I gave considerable thought to building only an .020" appliance for ease of manufacture.
DR. WHITE How will this system work for orthodontists who want to use bands on molars?
DR. ANDREIKO Elan will use no bands or convertible tubes. Since the slot geometries of Elan are such that no bends are required, the need for a convertible is gone with today's wire alloys. With the departure of the convertible feature, the tube becomes the smallest bracket in the system, with the greatest pad area. It seems that with the exception of headgear, we may finally see routine fully bonded orthodontics. Of course, the Orthos appliances are designed for banded molars, similar to existing appliances.
DR. WHITE What about hooks?
DR. ANDREIKO Elan will require a master prescription to be on file regarding hooks, slot sizes, etc. However, a mini-prescription sent in with the case could add hooks for surgery or delete them for simple Class I with mild crowding, or anything in between. Hook availability for Orthos will be the same as with current products.
DR. WHITE How viable has the Elan system of brackets and archwires proven in vivo?
DR. ANDREIKO Good question. I should say that we are in our seventh software revision and somewhere in the same vicinity with mechanical upgrades. I think that the analogy of chess-playing computers is a good one. The early programs were slow and could be beaten by many players. Currently, these machines play at the grandmaster level, and I think we are somewhere in this same growth curve. In the beginning, we found weaknesses and, as usual, they took longer to resolve than we had anticipated. So while we have cases in clinical testing, many of them are not of the most recent software and hardware. We need time to evaluate these results and assess the true performance of the current system. But I would like to say that most of the weaknesses identified have been dealt with, and the current cases appear to be progressing quite well.
DR. WHITE How have you been able to measure the Elan's efficacy, efficiency, and cost benefit?
DR. ANDREIKO Of course, you have just defined our goal. We anticipate significant increases in efficiency of treatment. For example, there should be a reduction in the repositioning of appliances, less upsetting of already-acceptable parts of the occlusion, and fewer appointments to finish the case. The system will allow the clinician to spend more time designing treatment plans and less time bending wires. This is a continuation in the shift from an art to a science. Realistically, though, these are undoubtedly the most expensive appliances ever built, and the answers are not in yet.
DR. WHITE How will the Elan system compare in price to the ordinary preadjusted appliance?
DR. ANDREIKO We don't really have a firm price yet. We are trying to keep the cost to a minimum so that it can be used more frequently.
DR. WHITE It seems from your description of the Elan system that the loss of a bracket will offer an unusual problem for the orthodontist and patient. How do you plan to remedy this?
DR. ANDREIKO Currently we are providing two complete sets of appliances with each case. In the future, the placement jigs will be reusable with Elan brackets, and I think brackets can be rebondable with the sandblast technique. This is really like most indirect techniques, where the bond is to already-cured adhesive. Worst case would be to reorder.
DR. WHITE What are some of the other problems this sophisticated system may have?
DR. ANDREIKO First, let me say that we greatly underestimated the complexity of this project from the beginning, and we have had many problems/opportunities along the way. And because the system is evolving, it is still possible for software glitches to provide less-than-optimal results, especially in cases like lower incisor extraction, or basically anything we have not written specific code for yet.
Since we work primarily from models, the rule is "garbage in, garbage out". The impression must be pretty good, although the system can repair small voids with the software.
As with anything that is new, there will undoubtedly be a learning curve for the clinician.
Lastly, the appliance won't wear its rubber bands any better than now.
DR. WHITE Can you tell me more about the Orthos project?
DR. ANDREIKO While Elan is a totally customized appliance based on the individual patient's skeletal and dental anatomy, Orthos is an appliance based on norms and averages derived from hundreds of Elan analyses. It contains refinements and upgraded logic from the other currently available prescriptions. The computer logic written to solve functional and static occlusal puzzles and the appliance design software developed for Elan are being used to design the Orthos average appliances. Elan is still under development, but Orthos should be introduced this year.
DR. WHITE How did you determine the significant dimensions necessary for making a more accurate preadjusted appliance?
DR. ANDREIKO This was a difficult task. I think the answer lies in the basic concepts of mechanical engineering, mixed with generally accepted orthodontic principles of occlusion. The six keys from Andrews were the starting point, but they were not really suited for digital calculations in three dimensions. Basically, the landmarks are chosen to satisfy centric occlusion requirements, as are familiar to your readers, with the addition of skeletal and functional criteria.
DR. WHITE How do these anatomical averages derived from Elan research affect Orthos appliance design?
DR. ANDREIKO We have found several things that affect appliance design and performance:
- By utilizing new rotation-in-slot technology, the lower anterior brackets have been reduced in the faciolingual dimension while, at the same time, the 1st-order relationship between lower cuspids and anteriors has been corrected.
- Mandibular posterior segments have less negative torque than prior designs to keep these teeth from being inclined lingually.
- Orthos archwire forms are taken from skeletal studies and are also "coordinated" mathematically for the first time.
- Molar rotations are calculated from actual anatomy for the first time.
- The mandibular arch has more progressive tip to aid in root paralleling (Fig. 4).
- Mandibular bicuspids have distal root tip to level marginal ridge contacts.
- Upper second bicuspids have distal tip to level marginal ridges between the second bicuspids and the first molars, and they are thicker than the first bicuspids to reduce the need for bayonet bends.
- Upper posterior segments have more buccal root torque to keep the dangling lingual cusps from causing balancing interferences with the prominence of today's expansion mechanics.
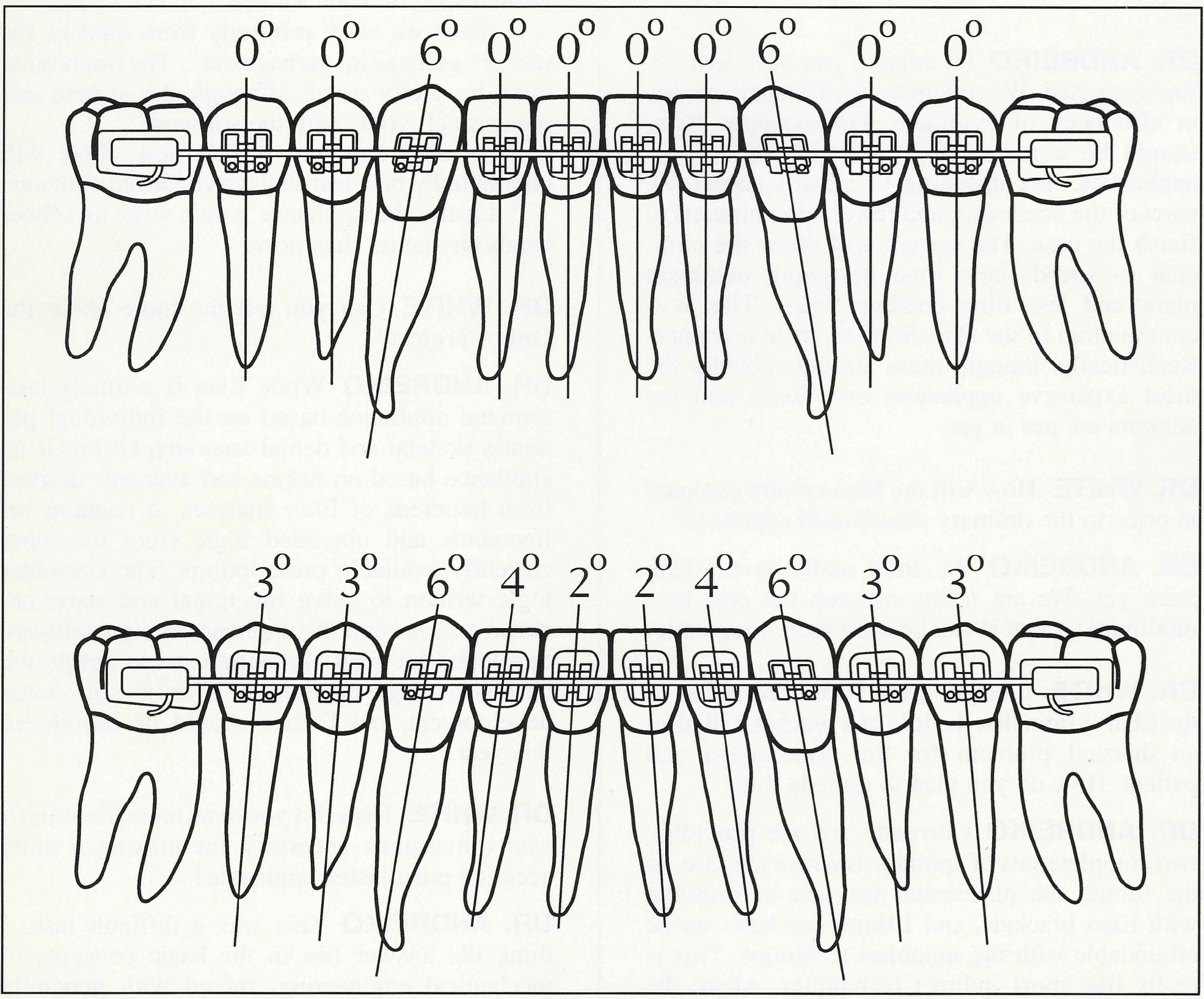
Fig. 4 Effect of progressive tip on root paralleling (top: typical prescription; bottom: Orthos values).
DR. WHITE How much difference is there in torque values between Orthos averages and Andrews originals?
DR. ANDREIKO In lower posterior segments the differences exceed 10°, but differences in thickness and angulation are far more significant clinically. For example, clinicians make far more 1st-order bends than 3rd-order bends.
DR. WHITE In the thousands of measurements you've made, have you found any distinct racial differences?
DR. ANDREIKO The Elan system has two basic functions. First is the production of individualized appliances, but the second is equally important. That is to create data bases of these appliances and occlusions that can be analyzed and sorted by many criteria. The first application of this has been studying the difference between races as they relate to appliances. We expect to have an Asian version of Orthos soon.
While there are many differences, the most significant are in the mandibular posterior teeth and the maxillary anterior region. For example, the lower first molars in Asian appliances require mesial rotation, due to the prominent buccal cusp, and increases in the maxillary anterior inclinations, due to a generally recessive midface. I have to mention that every bracket, tube, and archwire form is unique to this appliance, and that in the end, the details can add up to make a significant difference.
DR. WHITE Do you think there is a need for systems that reflect these racial norms?
DR. ANDREIKO I think that when the patient pool is of predominantly a single race, the appliance should be designed to impact the fat part of the bell curve. Practitioners using this type of appliance have no more inventory, and the appliances are no more costly than other appliances.
DR. WHITE Using such racial norms would seem little more than continuing with the "one size fits all" concept inherent in most current preadjusted appliances. How do you plan to avoid this problem?
DR. ANDREIKO Racially adjusted appliances are a continuance of the "one size fits all" concept. There is room for both average and individualized appliances. Obviously, the individualized appliance brings much more precision, but it is also more expensive. Still, the racially adjusted appliances would offer advantages over current prescriptions by adjusting the appliances to the anatomy.
DR. WHITE One final question: Why do you think the profession should endorse these new appliance systems?
DR. ANDREIKO The history of orthodontics has been one of innovation. One need only look at the appliances and treatment plans available today to see that the specialty has carefully but surely adopted much new technology. We hope that these systems will allow increased availability of orthodontic care over the coming years.
I'd like to leave your readers with a couple of interesting quotations:
"Another excellent way of causing the arch to bend within brackets and anchor sheath and, thus, to enlist force for uprighting, a distal tipping of the teeth (posterior teeth), is to change the positions of the brackets on the bands, thus changing the angles of relation of the slots of the brackets to the long axis of the teeth instead of making the vertical bends in the arch. This permits the use of the arch in its simplest form, or that freest from bends, which, of course, has advantages."1
"Theoretically, if all the brackets were to be placed in correct relationships to the respective teeth and if there were to be used a 100 percent elastic arch-bar, ideally formed not only as to gross horizontal form but all of the curvatures, indentations, and fine typal anatomical detail that presents for the case, then if the brackets were to continually fit the arch-bar with absolute accuracy, every tooth would receive such pressure as would tend to carry it to its correct location, not only as to position but to axial inclination as well."2
DR. WHITE Thank you for your thorough explanations.
FOOTNOTES
- *Ormco Corporation, 1332 S. Lone Hill Ave., Glendora, CA 91740.
REFERENCES
- 1. Angle, E.H.: The latest and best in orthodontic mechanism, Dent. Cosmos 71 :260-270, 1929.
- 2. Steiner, C.C.: Is there one best orthodontic appliance? Angle Orthod. 3:277-294, 1933.
-
 DR. WHITE
DR. WHITE -
 DR. ANDREIKO
DR. ANDREIKO
Dr. Andreiko is an orthodontic consultant with Ormco Corporation, 1332 S. Lone Hill Ave., Glendora, CA 91740. Dr. White is the Editor of the Journal of Clinical Orthodontics.