Overhead Reduction: Is Bigger Always Better?
Businesses all over the world, and especially in the United States, are attempting to downsize, streamline, and reduce the number of their employees and the size of their plants. One company after another has redesigned its tasks and carefully examined its operations to become more productive and profitable--"lean and mean". It's time for orthodontists to re-evaluate their practices and consider applying some of these same principles. There are many factors that affect your overhead, and most of these factors are under your control.
Practice Analysis
A good first step is to carefully analyze your fees, inventory and materials expenses, fixed costs such as rent or mortgage payments, and total staff expenses--including salaries, all benefits, and the number of employees. The ideal changes to increase profitability are the ones that positively affect all these areas. For example, your analysis will probably show that it is difficult to increase profitability by lowering your fees to try to increase your volume of patients. Therefore, periodic fee increases should be considered.
A less obvious area to examine is how many patients you see each day and what effect the number of patients has on your expenses. Do you have to have a bigger office, bigger staff, and bigger inventory if you see 100 patients per day or if you see 60 patients per day? Can you give each patient more tender, loving care, more positive motivation, and faster treatment when you see 100 patients per day or when you see 60 patients per day? Is a practice that sees 100 patients per day necessarily more profitable than the one that sees 60 patients per day? Is bigger always better?
Reducing the Number of Daily Patients
If you could reduce the number of patients seen daily without reducing the number of paying patients in your practice or increasing the number of days you work, you could have a smaller office, less inventory, and a smaller staff (or work fewer days each year--it's your decision). Here are some ways to achieve this goal:
1. Constantly try to improve your skills as an orthodontist. Strive for excellence in all your cases. Demand the best from yourself, your staff, and your patients; don't settle for less. There is no substitute for a beautifully treated case, happy patient, and satisfied parents. The better job you do with your diagnosis, treatment plan, appliance design and placement, positive patient motivation, and management of the case, the quicker you can finish and the better the final result will be.
2. Reduce the number of emergency office visits. Identify and eliminate as many problems with your mechanotherapy as possible. Train and manage your staff to reduce mistakes. Keep an emergency log to help you spot and correct the most common situations. The doctor should personally check each patient at the end of each appointment.
3. Reduce the number of missed or rescheduled appointments through communication. Call and confirm all appointments. Try to adjust your schedule to be as convenient as possible for your patients and their parents. They will then be more likely to keep appointments. Patients who frequently miss appointments tend to have extended treatment times.
4. Carefully examine your early treatment plans and fees. Early treatment can require three to four years of patient visits with little more fee collected than for full treatment alone. Be sure you are really accomplishing something to justify early treatment.
5. Charge for retainer check visits after a certain period of time. In my office, I include the first three months of retention appointments in the overall fee, then charge an office visit fee. You can't afford to see patients for free.
6. Don't short-cycle your patients. Carefully examine the way you appoint your patients. With certain procedures it is advantageous to see the patient every four weeks, but with other procedures five to six weeks would be more effective. Take advantage of new technology, and keep your treatment simple. Don't throw away your appointment time with wasted visits or unnecessary three-to-four-week appointment cycles.
If you see patients four days per week and you have 500 active patients (not counting recalls, new patients, and retainer checks), you will see 31.2 patients per day on a four-week appointment cycle. With a 5.5-week appointment cycle, you would see only 22.7 patients per day.
7. Reduce the number of Past End of Treatment (PET) patients. PETs are paid in full and should be finished with treatment, yet they are seen each visit for free. Some of these patients will have had difficult problems and will require extended treatment despite their best efforts and yours. These patients, of course, should be finished with no additional charges. A significant number of PETs, however, are due to lack of cooperation.
Compare two practices with different percentages of PETs and different appointment cycles, but the same number of paying patients (450). Practice No. 1 has 30% PET patients; with 450 paying patients, this means the practice has 643 active patients. On a four-week appointment cycle, the practice would see 40.2 patients per day. Practice No. 2 has a 10% PET rate, which means 500 active patients. On a 5.5-week cycle, the practice sees only 22.7 patients per day.
Develop Your Own PET Program
My practice goal is to finish 90-95% of our patients on time (or convert them to a monthly charge until complete, or remove the appliances at their request with a signed AAO legal release), and have 90-95% of our daily patients paying for our services through regular monthly charges, office visit charges, or retainer check charges. During the past seven years, my staff and I have set up a PET program that has helped us keep the number of PET patients between 5% and 10% each month. I feel this system has significantly contributed to keeping my overhead between 40% and 45%.
How can you accomplish such goals? You must first design treatment plans that will achieve the best possible result and require the least effort and compliance by the patients. Identify in advance the cases that will require more time, effort, and cost to complete their treatment, and charge a higher fee to those patients. Such cases might include adults, surgical-orthodontic cases, transfer-in patients, early treatment, patients with impacted teeth, cases with severe skeletal problems, and patients and families who demonstrate less-than-ideal attitudes at initial examinations.
The doctor and staff must develop a system of communication with patients and parents that will monitor each patient's progress and compliance. A secondary benefit of such a program of documenting and dealing with potential problems is improved risk management.
The PET system must begin with the conference appointment and extend from that point until treatment is completed. Frequently patients do not fully cooperate in the first six months of treatment, yet we are too busy and don't want to confront the problem until they reach 24 months or more. We then wonder why they don' t finish on time and why we have 30% or higher PET rates.
An effective, friendly, and timely communication policy allows you to set a limit on the number of months treatment can extend before the patient and parents have to decide to have appliances removed by signing a legal release, or to restart the monthly charge at 60-100% of their original monthly charge. Our PET system includes the following steps:
1. New patient examination: I stress the importance of patient cooperation and teamwork. "The orthodontist straightens the teeth, and the patient makes them fit."
2. Conference/case presentation: The treatment plan sets the length of treatment in writing. The "Truth In Lending Form" states that there will be additional monthly charges if treatment is extended past the projected time due to poor patient cooperation.
3. Letters are sent throughout treatment as needed to let the patient and parents know about any problems with patient cooperation. We have developed a series of computer-generated letters, increasing in concern and intensity, for oral hygiene, elastic wear, headgear wear, broken appliances, and missed appointments (Figs. 1,2,3). Every attempt should be made to create caring, positive, friendly, non-threatening letters that attempt to enlist the patient's and parents' help with the problem. We frequently revise our letters to make them more friendly; you can't be too nice, especially in the early stages. All letters are signed by the doctor, copied for the treatment record, and mailed within two days of the visit.
4. Brief verbal progress reports are given by the doctor to the parents after appointments as needed. I typically talk to the parents of problem patients once or twice before we schedule a longer progress conference.
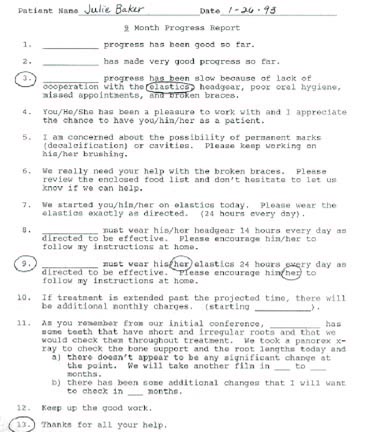
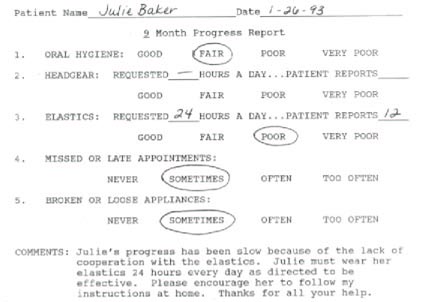
5. Nine-month progress report and panorex: Eight months into treatment, the treatment coordinator notes in green ink on the chart that the patient is due for a nine-month progress report. At the next appointment, a panorex is taken and evaluated. The orthodontist circles the numbered statements that apply to that patient on the progress report form (Fig. 4). The treatment coordinator selects the responses on the computer and prints out the progress report (Fig. 5). She fills in the appropriate responses for oral hygiene, headgear, elastics, missed or late appointments, and broken or loose appliances. She then attaches a computer-generated cover letter (Fig. 6). The doctor reviews and signs the letter, and it is copied for the chart and mailed.
6. 18-month progress report and panorex: The same procedure is followed as with the nine-month progress report, but we use slightly different wording in the comments section and cover letter.
7. Scheduled progress conference: A conference should be scheduled as soon as the doctor realizes that the patient's cooperation is affecting the case and could result in extended treatment time. This might be after the 18-month progress report or even earlier.
At the progress conference, the doctor discusses the problem areas with the parent and patient, and the treatment coordinator circles the topics discussed on the report form (Fig. 7). A date for initiating additional monthly charges or for removing the appliances and signing a legal release is set. The disadvantages of removing appliances before an ideal result can be achieved are discussed. The parents are told that the treatment coordinator will contact them at that point to see what their decision is.
I tell the parents that I'll do anything they want me to do, but I just want to get the teeth straight and the bite as good as I possibly can. They still have a chance to get their child to cooperate 100% and possibly finish on time. In most cases, I am able to say that I really like Susie or John, and in spite of our problems, she or he really is a good kid we have enjoyed having in our practice.
8. Estimated end of treatment: In the vast majority of cases, we are able to remove the appliances on time with a high-quality result and a happy patient and family. In cases that haven't finished on time, the family is contacted by the treatment coordinator and is either placed on a monthly charge or scheduled to have the appliances removed after signing a legal release. In some cases, where cooperation was at times acceptable or I didn't document the lack of cooperation early enough, I will give the patient from two to six extra months before starting additional monthly charges.
We try hard to remain friends with the PET patients and their families, and in most cases we are successful. My practice has a high percentage of second and third children in families--even when previous children were PET.
9. PET list: A list is printed by the treatment coordinator at the beginning of every month and posted in the clinic area. Each patient is categorized by the doctor as difficult, adult, surgery, close to finished, on monthly charges, limited (to go to a monthly charge at a specified date), or scheduled to have appliances removed (Fig. 8).
The purpose of our PET program is to give the parents, who are ultimately responsible, the chance to try to get their child to cooperate so they can finish on time with a good result. If we address the problems when they are small, and do so tactfully, we do not lose any good will.
How many times have you heard a parent say, after "finally" hearing the bad news at 24 months, "I wish you had told me"? Whose problem is it if the orthodontist doesn't keep them informed? Do the parents, patients, yourself, and your staff a favor by communicating the first and every time you have a problem--poor oral hygiene, poor elastic wear, poor headgear wear, broken appliances, or missed appointments.
Conclusion
Is bigger always better? Not necessarily. We tend to associate activity with productivity, and productivity with profitability. By streamlining your practice to reduce the number of emergency visits, missed appointments, short-cycle appointments, and PET patients, you can significantly reduce the number of patients you see every day.
The combined effects of seeing fewer patients, improving your risk management, and having a system to deal with patients who won't cooperate should reduce stress for you and your staff. The changes won't happen overnight, but in time can improve your profitability by reducing your overhead and making your practice more fun.