The DigiGraph Work Station, Part 2: Clinical Management
Editor's note: Parts 1 and 3 of this series are published in the June and August 1990 issues of JCO.
The DigiGraph Work Station (Fig. 23) is a unique device that allows the clinician to perform non-radiographic cephalometric tracings and analyses, video imaging, and treatment planning, including manipulation of the patient's tracing overlaid on the video image. It also takes facial, intraoral, and model photographs (see Part 1, JCO, June 1990).
Location of the Equipment
The DigiGraph performs many record-taking functions, so the orthodontist's first inclination is usually to place it in the same room as the cephalostat and/or photographic equipment. This seems to work well when the practice also has one or more DigiGraph Consultation Stations.
In this situation, record-taking procedures require little modification. The patient is sent to the records area to have the DigiGraph records taken (Fig. 24). These records, stored on 3½" disks, are immediately transferred to the Consultation Station in the consultation room (Fig. 25).
If only one consultation unit is available, it can be kept in the operatory for on-the-spot progress and post-treatment consultations. It can easily be rolled into the consultation room if required for a case presentation.
If the main DigiGraph Work Station is the only unit in the office, the best location may not be the traditional records or x-ray area. Because the DigiGraph makes it possible to see records in the operatory and to use the records for consultations with the patient before, during, and following treatment, a popular site for offices with only one station is the consultation room or doctor's private office.
Actually, the DigiGraph may be placed in any open area of the office. Since there are no x-ray emissions, the machine can be placed almost anywhere there is space. Patients appreciate it as a symbol of the high level of technology involved in their care, and so we suggest that it be visible.
Information Storage
Another decision related to the DigiGraph is where to store the patient information. As discussed in Part 1, each patient has two 3½" disks (one a backup) on which all recorded DigiGraph data are stored. The first time records are taken for a patient, two blank disks are loaded into the DigiGraph. At the end of this initial session, when the information is recorded, the operator labels both disks with the patient's name and number.
It is advisable to have the two disks together only while DigiGraph records are being taken. Otherwise, they should be stored separately to minimize the chance of both disks being destroyed.
One successful approach is to keep one disk in the patient folder, and the other in a box of disks on top of or near the main DigiGraph unit. Whenever records are taken during treatment, the patient folder is brought with the patient to the DigiGraph, and both the disk in the folder and the disk stored near the DigiGraph are loaded into the machine.
The disk from the patient folder can also be used at any Consultation Station. However, records are taken at the main Work Station only and cannot be taken at the Consultation Station.
Paper, Photographic, and Slide Records
The DigiGraph can produce "hard copy" output of any screen image on three devices: a Sony video imager for 5"X7" color prints; a Polaroid freeze-frame camera (with an optional 35mm slide back for making slides); and a Hewlett Packard PaintJet printer for paper color copies.
If the office has at least one Consultation Station, there is no need to go to the time and expense of making photos, slides, or other printed copies of every patient record routinely; Sometimes, however, the orthodontist may wish to print specific pictures or slides for the patient or referring dentist.
If there is only a main DigiGraph unit in the office, it may be desirable to make hard copies of all records as they are taken. These can be stored in the patient folder along with one of the patient disks, and they can then be viewed anywhere in the office, or used for consultations, without the need for the Consultation Station.
The Initial Appointment
An important benefit of the DigiGraph is the ability to obtain and analyze diagnostic records at the first appointment, complete the consultation at the same appointment, and even initiate treatment at that same appointment. Patients and their parents want to receive as much information as possible at the initial exam. In our experience, practices that seek a commitment to treatment at the first visit have a higher rate of case acceptance than those following the more traditional scheme of two to three appointments before case presentation.
One schedule for this all-inclusive first appointment that we have found successful is as follows:
The patient and parent are first taken to the consultation room. The customary short description of the office and orthodontic treatment is provided by the staff or orthodontist. The patient is then taken to the DigiGraph Work Station, where an assistant takes complete records. It will take about 10 minutes to enter all cephalometric data using the sonic digitizer, take all facial and intraoral video images, and store all records onto the floppy disks. Meanwhile, the parent can be completing forms such as the patient history and credit information.
The patient is then returned to the consultation area to receive additional information about treatment, or returned to the reception room. During this period (10 to 15 minutes), the orthodontist can analyze the records, perform Visual Treatment Objectives, and prepare the presentation.
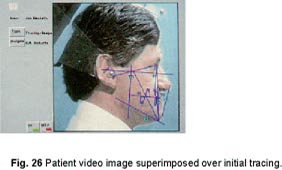
Finally, in the consultation room (if a Consultation Station is present), or at the main DigiGraph, the doctor presents the proposed treatment plan. The patient's images, superimposed over the initial tracings, are shown to help explain the malocclusion and the need for elastics, headgear, extractions, etc. (Fig. 26). The orthodontist may choose to show a modified facial image depicting what the patient might look like following treatment. Similar cases and patients with similar appliances can also be shown.
The fee is presented, and if the patient or parent accepts, any required radiographs and impressions are taken. If time has been reserved, the initial clinical appointment can be started.
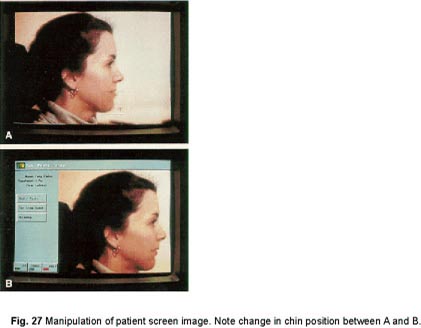
If the patient initially appears uncertain about the need for treatment, it may be helpful to take a frontal or lateral video image of the patient with the DigiGraph rather than the entire diagnostic series. Then the doctor can discuss the screen image and manipulate it so the patient can more easily see the potential benefits of orthodontic treatment (Fig. 27). After this discussion, the patient may elect to have full DigiGraph records taken.
Monitoring Progress and Cooperation
An operatory station is especially valuable during treatment. The DigiGraph provides the ability to recall intraoral images from previous appointments for comparison to what the clinician observes in the patient's mouth at that moment (Fig. 28). It's easier to remember what went on at the last visit when one can visually demonstrate dental changes.
Since there is no radiation exposure from the DigiGraph, an updated cephalometric analysis can be performed as often as desired. This allows the orthodontist to monitor the patient more thoroughly, to gain more control over treatment, and to intercept potential problems earlier. The DigiGraph appeals to those who have been in practice a number of years and have stopped taking progress cephalograms in the interest of radiation hygiene.
Progress records can be taken in a few minutes at any appointment. The patient is escorted, along with the treatment folder, to the DigiGraph Work Station, and the desired records are taken. The patient returns with the folder to the operatory. If there is a Consultation Station in the operatory, the disk is loaded from the folder into the DigiGraph, and the clinician can call up the old and new records for viewing. If the office has only one unit, hard copies of the new records are put into the patient folder along with the disk.
Post-Treatment Records
Most orthodontists take post-treatment records, often with the underlying motive of protection against any future legal procedures. However, an important positive use of records is to evaluate post-orthodontic needs, while increasing patient and parent appreciation of the high quality of care received.
How many doctors have collected posttreatment records over the years intending to see how specific mechanics affected certain malocclusions, but never had time to follow through? One would have to go through hundreds of radiographs, tracings, models, and photos to collect the sample. Then one would have to compare measurements manually and do some sort of analysis. Very few of us have that much time.
The DigiGraph stores a set of summary data for each patient on the unit's hard disk. Such information as patient name, number, age, race, sex, and malocclusion classification can be retrieved simply by turning on the DigiGraph. (It is not possible to store complete patient data on the hard disk, because the video images would quickly fill up the disk.) To find cases with specific pretreatment characteristics, one merely runs a "sort" on the complete list of patients . The names of all patients matching these characteristics will appear on the monitor. At that point, the appropriate patient disks can be loaded into the machine to begin analyzing the data. This makes it easier to see if that new technique really speeds up treatment time, or produces more consistent results.
Post-Treatment Consultation
Because orthodontics is a gradual process, many patients forget how much their appearance changed during treatment. The DigiGraph offers the opportunity to show the patient video images that graphically illustrate improved appearance as a result of orthodontic treatment.
Immediately after debonding, new DigiGraph records can be taken, and the post-treatment consultation can be presented by the doctor or staff member.
One of the highlights of the consultation is the presentation of "before and after" images on the screen (Fig. 29). A printed copy of this image can be made immediately and given to the patient and family to take home. This is an outstanding marketing tool, as happy patients will show the pictures to friends and relatives while discussing their orthodontic treatment and orthodontist.
Patient Reactions
Based on our early use of the DigiGraph, patients and parents tend to be impressed by several aspects of the system:
1. Patients can see more clearly their present dentofacial status. It becomes apparent after using the DigiGraph that most patients never completely understood the significance of radiographs, tracings, and models. In fact, many are put off by the records. This is especially evident in consultations with parents whose older children were given a more traditional presentation. Many comments have been made about how the DigiGraph approach is much easier to understand. Now, when the orthodontist begins the diagnostic portion of the consultation by showing the lateral image with the tracing superimposed and says, "This is you", the patient knows exactly what the doctor means.
2. Patients and parents understand more about what treatment can accomplish. It is surprising how often patients, even those with severe maxillomandibular imbalances, do not know that orthodontics can change facial appearance dramatically. Most people think that orthodontics is simply for straightening teeth. It is surprising how often a patient, upon seeing the proposed improved facial appearance in photographic form, becomes more enthusiastic and ready to start treatment.
On the other hand, there are times when compromises in the facial balance are required to treat the case without orthognathic surgery or extractions. It is important for the patient to be aware prior to treatment of the limitations involved. From a legal standpoint, clearly informing the patient and parent of the treatment alternatives and limitations is the most important part of a case presentation.
3. Patients are more accepting of headgear, elastics, extractions, and orthognathic surgery. The two most common questions asked by patients and parents in consultations involve extractions and the need for headgear. If the orthodontist can demonstrate visually how extractions would improve the patient's appearance, the patient can assume a more active role in the treatment decisions. After seeing how the headgear will improve the profile, the patient will be more highly motivated to wear it diligently. Many cooperation problems are the result of not understanding the benefits of following the treatment plan.
4. X-ray exposure can be eliminated or reduced, even if a panoramic x-ray and perhaps an initial cephalogram are still taken. Many patients and parents have heard about the dangers associated with radiation exposure. Explanations about grids, screens, and the minimal dosage associated with cephalograms do not completely assuage the fears. Have you ever asked prospective patients whether they are concerned about x-rays? You might be surprised at the results of an informal survey.
5. Patients like the DigiGraph's up-to-date image. Many patients are aware of similar developments in the fields of facial reconstruction, aerospace design, diagnostic imaging, cosmetology, optometry, hair styling, and other fields. People are ever more impressed with video displays and computers. Patients talk about "this new video machine at the orthodontist's office" to their friends. When given photographic output from the machine, they almost always show the pictures to others.
Orthodontist Reactions
Orthodontists who have used the DigiGraph cite several benefits beyond patient acceptance:
1. Treatment can be initiated as soon as desired, even at the first appointment. There's no need to "best guess" a preliminary treatment plan to satisfy initial patient curiosity and then change plans at the consultation appointment. Moreover, because of the clear and understandable presentation at the initial appointment, more patients are willing to accept treatment. Beginning treatment at the initial appointment insures highly motivated patients. Waiting three or four weeks invites wavering in the decision to commit to treatment.
2. Diagnostic records can be taken more easily, reliably, and quickly. There are never any cephalograms that don't come out or intraoral photos that were not taken properly. As the clinician or assistant takes the records, the outcome is visible on the monitor. Therefore, there is never a need to call a patient back to retake records. There is no gap of several days or weeks while film is being developed, and film-processing costs are greatly decreased or eliminated.
3. Storage space can be reduced considerably. Many offices are filled with dental casts and diagnostic-record folders. The 3½" disks occupy much less space. Tracings, photos, and other records can be printed in paper or photographic form only as needed. Even headfilms can be recorded on the DigiGraph by attaching a light box to the head holder and taking video images. According to the American Dental Association, in many states it is now legal to save video images of models rather than the models themselves.
4. Aside from the potential increase in patient starts, a number of clinicians have found DigiGraph usage to increase per-case income. Many assess an additional fee for DigiGraph records, and some of these offer the patient the choice of whether to have DigiGraph or conventional records taken. Some orthodontists who use x-ray labs or diagnostic services have reduced expenses in those areas; fees that used to go to the lab or service are being retained in the practice.
Conclusion
The DigiGraph Work Station allows the patient to understand thoroughly, prior to treatment, what can and cannot be expected, increasing the desire for treatment and willingness to cooperate. It provides information for the orthodontist to plan treatment during the initial appointment, and to start treatment immediately if desired. It offers comprehensive treatment-monitoring information without exposing patients to additional radiation.
It allows all of a patient's radiographs, tracings, cephalograms, photos, and models to be stored on one small disk, thereby reducing storage requirements. Most of all, it is a valuable tool for improving communication among orthodontists, patients, and staff.