Removal of White Spot Lesions by Controlled Acid-Pumice Abrasion
Decalcification and white spot lesions can occur in as many as 25-30% of orthodontic patients, even with the use of fluoride, and as early as one month after beginning treatment.1-5 Fewer than 1% of these cases, however, show cavitation.4
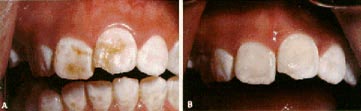
White, yellow, or brown stains can be removed with a controlled acid-pumice abrasion technique as long as the defect is confined to the superficials layer of enamel.6 The enamel discoloration gradually disappears with repeated applications of the acid-pumice solution.7 After polishing and remineralization, the exposed enamel returns to normal color and surface conditions (Fig. 1).8,9 Most patients demonstrate improvement over time because of ongoing remineralization.10,11
Technique
Be sure to protect the eyes of the patient, clinician, and assistant before beginning the technique. Isolate the teeth with a rubber dam to prevent acid from contacting soft tissues (Fig. 2A). Wear rubber gloves and follow normal infection-control procedures. Keep a water spray and high-speed suction at hand in case of any acid spillage.
Add a 30-40% aqueous solution or gel of phosphoric acid to fine flour of pumice to make a thick paste. Apply the paste to the enamel surfaces with a wooden stick, or use a rubber cup at slow speed and with extreme caution to prevent splashing of the acid solution.
Rub the paste gently into the enamel for 10 to 30 seconds, then rinse for 10 seconds with a copious water spray. Reapply the mixture as necessary to achieve the desired color, but do not exceed 20 minutes at one sitting.
Use a fine, aluminum oxide, composite resin polishing disc to restore the normal enamel luster after removal of the stain. Neutral sodium fluoride can be used as the lubricant. After each appointment, treat the teeth with neutral sodium fluoride for a minimum of four minutes.
Tooth color will improve in most patients (Fig. 2,Fig. 3). If no distinct improvement occurs by the fifth appointment, abandon the technique.
Discussion
The mineral content of saliva will often cause a white spot lesion to disappear within weeks of debanding.12 Saliva remineralization seems to be more effective in nonfluoridated patients than in those who have been rinsing with fluoride. Rinsing the lesion with a concentrated-fluoride solution can cause rapid remineralization of the surface layer, thus preventing fluoride penetration to the subsurface enamel. Without remineralization of the subsurface layer, the discoloration will not be resolved.
Therefore, lesions visible upon appliance removal should be treated conservatively, using normal oral hygiene and not concentrated-fluoride agents. The natural remineralizing effect of saliva will resolve many white spot lesions within weeks. Any remaining discoloration can then be removed with controlled acid-pumice abrasion, as long as the defect is confined to the superficial enamel.
Acid-pumice abrasion was originally used to treat enamel fluorosis.13 Several chemical techniques have been described, including concentrated hydrogen peroxide with heat,14-16 hydrochloric acid,17-24 diethyl ether,16-25 sodium hypochlorite,15,19-21 or combinations of these agents. The advantages of a phosphoric acid etching solution are that it is readily available in a dental office, is less caustic than other acid solutions, and provides esthetic results comparable to those of stronger solutions.
The chief concerns with this technique are whether the amount of enamel sacrificed is clinically significant and whether there is any danger of pulpal irritation. The acid-pumice technique removes enamel both by chemical erosion and mechanical abrasion, but the loss of about 6 microns of enamel per application6 is similar to that after prophylaxis with a rubber cup.26 One study reported .1mm of enamel loss during a 20-minute acid-pumice treatment.19 The actual amount lost will vary depending on the amount of time the acid is in contact with the tooth surface and the pressure on the handpiece. Extensive application might cause a noticeable loss of the mesiodistal curvature of the labial surface,24 but generally the amount of enamel lost is not clinically significant when compared to the esthetic results.
The acid-pumice technique does remove the fluoride-rich superficial layer of enamel.27-29 Therefore, fluoride must be topically applied for four minutes to restore fluoride levels after the abrasion.
This technique has not resulted in any noticeable pulpal hypersensitivity.19,22-24 An investigation of the permeability of enamel to 16 percent hydrochloric acid found the acid did not penetrate the enamel surface of extracted teeth into the pulpal chamber.30
The patient should be advised that the acid-pumice technique might not work, especially if the decalcification is not confined to the superficial enamel or there is evidence of cavitation. It is not always possible to clinically judge the depth of the enamel defect before treatment.6
Conclusion
Despite the increasing use of fluoride and emphasis on oral hygiene, some patients will still have white spot lesions following orthodontic treatment. The acid-pumice technique provides permanent removal of discoloration with insignificant enamel loss and no damage to the pulp or periodontal tissues. The procedure is easy to perform, requires minimum clinical time, and is well tolerated by patients.