Bonded Pontics in Orthodontics
During the last decade, new esthetic materials and innovative bonding techniques have made it possible for orthodontists to use bonded replacements for missing teeth instead of removable partial dentures. These bonded pontics can also fill extraction sites temporarily when extraction treatment is necessary. The ability to provide esthetic tooth replacements with minimal time and financial commitment can be especially reassuring to the socially conscious adult patient.
This series of case reports shows how various extracoronal bonding procedures can be used for space opening, space closing, and space maintenance.
Prefabricated Acrylic Denture Teeth
A prefabricated acrylic denture tooth can provide a simple bonded replacement for a missing tooth.
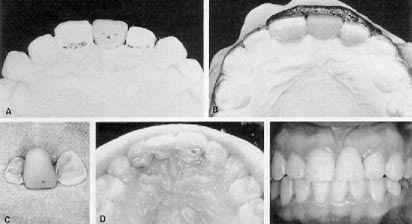
Grind in the appropriate acrylic tooth on a study model (Fig. 1). Because the acrylic tooth will not bond well to composite, it is a potential weak link in the restoration. Drill multiple undercut holes in the pontic with an inverted cone bur to provide a mechanical lock and avoid fracture from occlusal stress.
For maximum strength and minimum thickness, the acrylic tooth must be supported by a wire in the composite adhesive. Form a heat-treatable .028" round wire to contact the lingual surfaces of the abutment teeth and the pontic. Bend the ends of the wire so they will be retained within the composite. A straight wire (even a rectangular one) will fail to hold the pontic when subjected to functional stress (Fig. 2).
Coat the surfaces of the abutment teeth with a separating medium. Apply composite to all lingual surfaces, taking special care to fill the retention holes. Remove the completed bridge from the model, and trim away any gingival excess with a safe-sided disc.
Bond the restoration to the lingual surfaces of the abutment teeth using the acidetch technique. Make the composite less viscous by adding a drop of sealant to the mixture. Remove any excess gingival and interproximal composite.
Special considerations:
1. Maxillary anterior restorations require interincisal clearance because of the bulk of the composite and reinforcing wire.
2. If the involved teeth are to be moved during treatment, construct the bonded restoration as a cantilever, thus permitting complete freedom of movement (Fig. 3).
3. Adequate space is required to use a prefabricated acrylic tooth.
4. When bonding the restoration to the abutment teeth, cover the lingual aspect of the incisal edge with composite to minimize functional stress and avoid displacement.
5. Articulate study models as needed to avoid incisal interference with the pontic.
Custom Processed Acrylic Teeth
Custom-made acrylic pontics offer greater flexibility in design and eliminate the problem of the weak bond of composite to acrylic, but they require more laboratory work.
On a study model, bend a soft, heat-treatable .028" wire to conform to the lingual surfaces of the abutment tooth or teeth (Fig. 4). Extend the wire into the edentulous area and bend loops to support the tooth or teeth to be formed. Harden the completed wire in a brush flame.
Coat the lingual surfaces of the abutment teeth with a separating medium. Flow composite onto these surfaces to secure the wire in position. Wax up the replacement tooth or teeth, engaging the wire anchor loops. Remove the waxup and bonded onlay and invest, flask, and process them in acrylic of the appropriate shade.
Bond the completed bridge to the abutment teeth using the acid-etch technique. Remove any gingival excess composite.
Special considerations:
1. For increased strength, process the acrylic to surround the wire anchor loops.
2. Custom processing can produce excellent shade and form.
3. In a long span (two or more pontics), an .030" or .032" wire may be desirable.
4. Cover the incisal edge of the abutment tooth with a thin coating of composite to minimize functional stress.
5. Articulate study models as needed to avoid incisal interference with the pontic.
Discussion
The replacement of missing teeth with removable appliances has long been a problem in orthodontics. "Flipper" appliances are unstable. If clasps are added for retention, both the clasps and acrylic interfere with the usual tooth movement procedures. Constant modifications and compromises as the dentition changes result in appliances that are ill-fitting and unesthetic.
The bonded replacement can be constructed in the traditional manner, with abutments at each end, or it can be made as a cantilever when necessary, such as in space closure (Fig. 5).
If one or more teeth must be extracted, a bonded replacement can be placed as an immediate restoration. This is particularly useful with adult patients (Fig. 6). In a bicuspid extraction case, take care to leave a slight space between the pontic and the gingiva to avoid impingement as the canine tips distally! Also, the loop of the reinforcing wire should be as close to the abutment tooth as possible; this allows the pontic to be reduced as the space is closed without cutting the reinforcing wire.
The fixed replacement avoids the gingival impingement and inflammation commonly associated with the settling of tissue-supported removable appliances. Patients will maintain good oral hygiene if they are encouraged to use floss threaders and irrigating devices.
We have had excellent results for many years with these techniques. Bonds on the abutment teeth rarely fail during orthodontic therapy. Even cantilevered pontics in the anterior and bicuspid areas have usually survived the full term of orthodontic treatment.