1986 JCO Study of Orthodontic Diagnosis and Treatment Procedures Part 1 - Overall Results
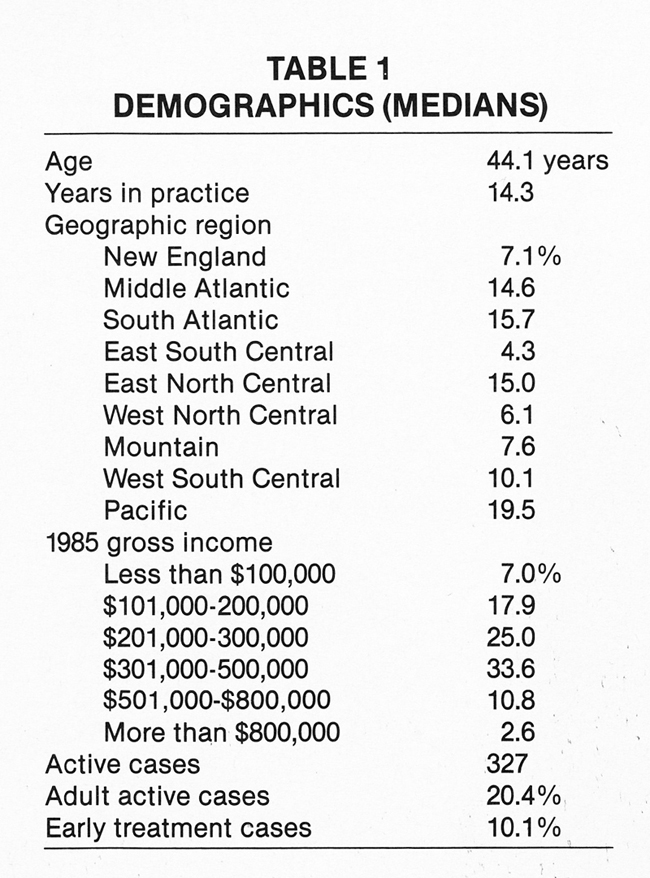
This study is the first comprehensive nationwide survey of current orthodontic diagnosis and treatment procedures. A questionnaire was mailed in February 1986 to all identifiable orthodontic specialists in the United States. A total of 1,486 usable questionnaires were returned, representing about 18% of practicing orthodontists. The size of the response and the similarity of demographic data (Table 1) to those of the 1981, 1983, and 1985 JCO Orthodontic Practice Studies confirm the validity of the results.
Data analysis was performed with the Statistical Package for the Social Sciences at the University of Colorado Computing Center. This article presents frequency responses to the items on the questionnaire for the entire sample. Next month's article will break down selected items by categories such as geographic region and years in practice.
Similar articles from the archive:
- 1985 JCO Orthodontic Practice Study, Part 1: Trends November 1985
- 1983 JCO Orthodontic Practice Study, Part 1: Trends March 1984
- JCO Orthodontic Practice Study: Practice Activity September 1981
Most responses are shown as percentages of the 1,486 orthodontists who responded in each category. In some instances (number of photographs taken, wire sizes, and TMJ treatment methods), the percentages shown are not of the entire sample, but only of those respondents who used a particular item or procedure.
For numerical data (e.g., age, years in practice, number of active cases, percentage of adult cases), the results shown are medians, which are less likely than means to be influenced by extreme responses. It should be noted that a column of median percentages (as in percentage of extraction cases and patient distribution in surgical-orthodontic cases) will not necessarily add up to 100%.
Demographics
The demographic data of the Study sample (Table 1) show that the median number of early treatment cases in 1985 was 10.1 %. The median number of adult active treatment cases was 20.4%, almost identical with the result in the 1985 JCO Orthodontic Practice Study.
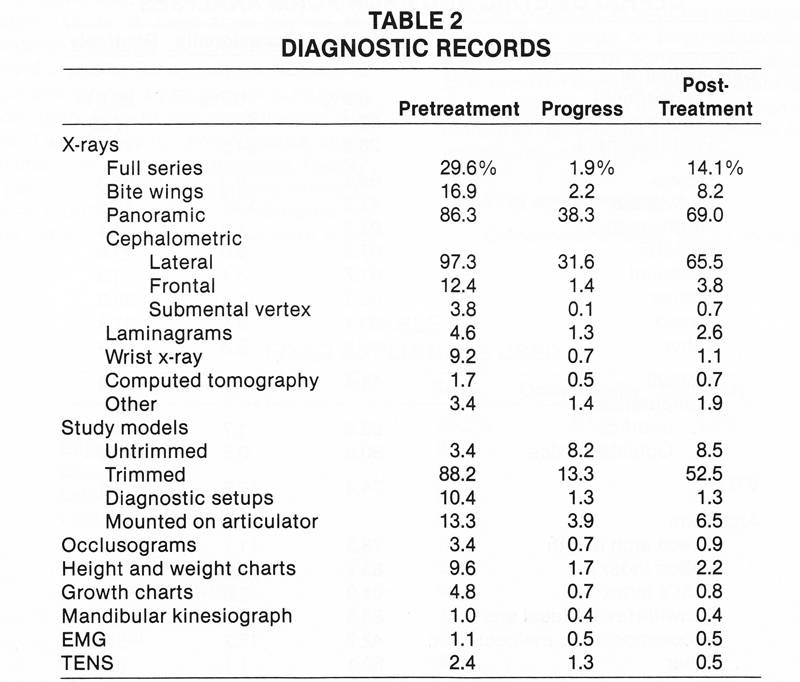
Diagnostic Records
More than 85% of the sample used pretreatment panoramic and lateral cephalometric x-rays and pretreatment trimmed study models; more than half routinely took the same records after treatment (Table 2). Only 12.4% of the respondents reported taking pretreatment frontal cephalometric x-rays.
Fewer than 10% of the respondents reported progress procedures other than panoramic and cephalometric x-rays and trimmed study models, and fewer than 10% reported post-treatment procedures other than those three plus a full x-ray series.
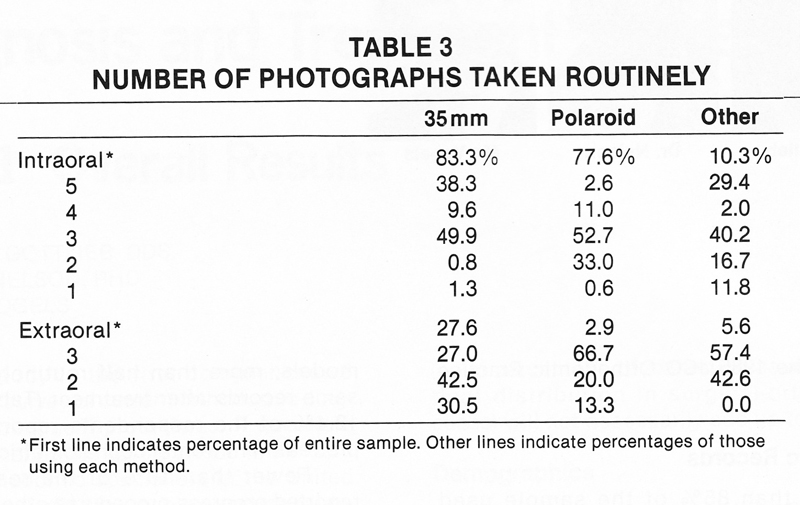
More orthodontists reported using 35mm photography than used Polaroid photography (Table 3). Only a minority of the sample took any kind of extraoral photographs. A majority of those who used photography in their diagnostic records took three intraoral photos per patient and either two or three extraoral photos. Of the 6% of respondents who mentioned other photographic techniques, almost half used color prints other than 35mm, and less than one-quarter used black-and-white prints.
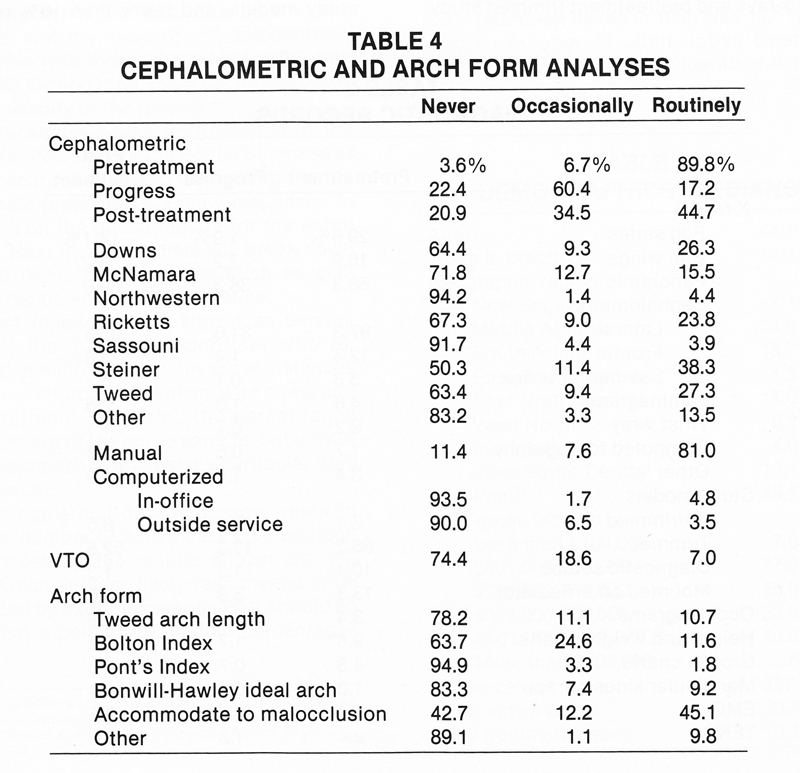
Cephalometric and Arch Form Analyses
Pretreatment cephalometric analysis was used either routinely or occasionally by all but 3.6% (Table 4). Less than half of the respondents routinely did progress or post-treatment cephalometric analysis. No particular cephalometric analysis was used routinely by more than 40% of the respondents. The Steiner, Tweed, Downs, and Ricketts analyses, in that order, were used the most. Twenty three percent listed other analyses; one-third of these reported using a combination of various types, while lesser numbers mentioned Jarabak, Holdaway, and WITS. Less than 10% of the sample routinely used computerized tracings, and these were fairly evenly divided between in-office and outside service. About three-quarters of the sample said they never used a VTO.
The only arch form analysis used routinely by more than 12% was one accommodated to the malocclusion. Other arch form analyses, listed by 3% or less of the respondents, included Brader, Roth, and a combination.
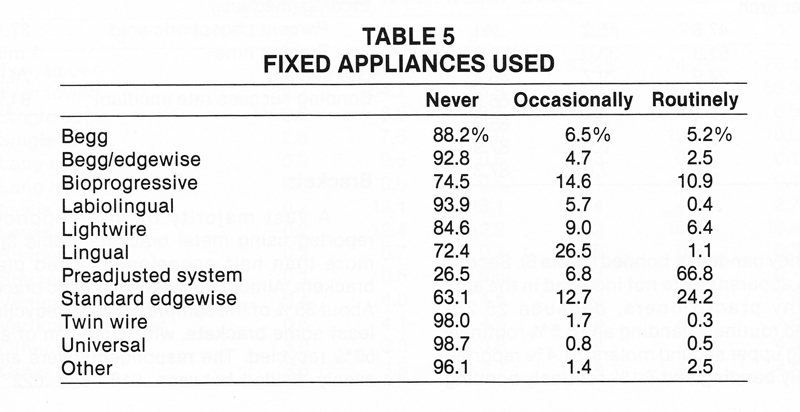
Fixed Appliances
The most popular fixed appliance system by far was a preadjusted system, with standard edgewise a distant second (Table 5). Lingual appliances were used occasionally by 26.5% of the respondents, but routinely by only 1.1 %. About 19% of the sample reported using either Begg or Begg/edgewise appliances routinely or occasionally, and about 25% used the Bioprogressive system routinely or occasionally. The median duration of treatment was reported as 24 months for all appliances except lingual (27 months).
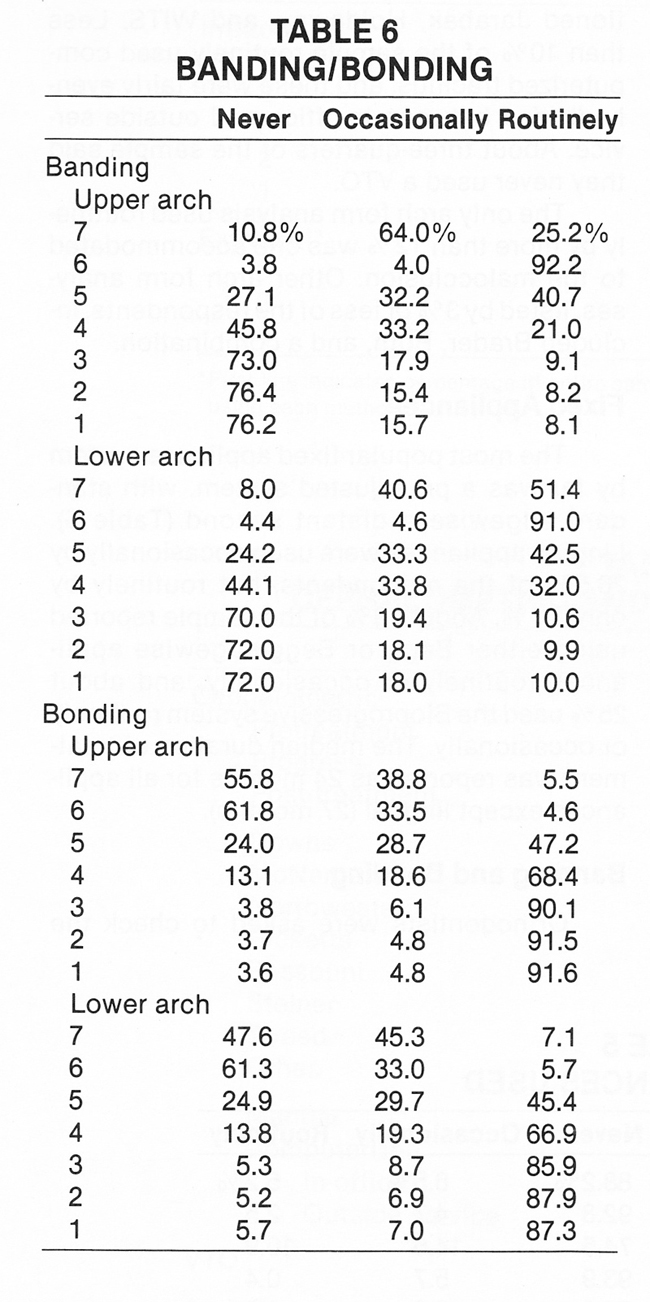
Banding and Bonding
Orthodontists were asked to check the teeth they banded or bonded (Table 6). Second molars apparently are not included in the arch by many practitioners, because 25.2% reported routinely banding and 5.5% routinely bonding upper second molars; 51.4% reported routinely banding and 7.1 % routinely bonding lower second molars. While more than 90% reported banding upper and lower first molars, only about 5% said they were routinely bonding upper or lower first molars. More than half the respondents reported banding bicuspids either routinely or occasionally, but greater numbers favored bonding. Only about 10% or fewer were routinely banding incisors or cuspids. Still, about one-quarter of the respondents were banding anterior teeth at least occasionally.
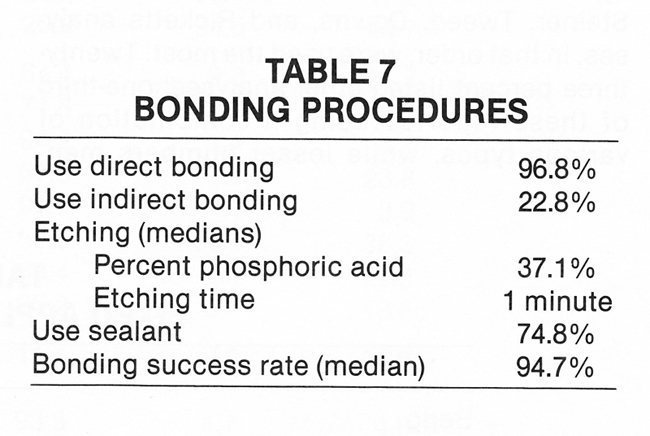
Almost all orthodontists reported using direct bonding, but less than one-quarter used indirect bonding (Table 7). About 90% of the sample reported etching; about two-thirds of these etched for one minute, about 20% for 1½ minutes, and about 10% for two minutes. While the median concentration of phosphoric acid was 37%, 24% of the respondents favored a concentration of 50%. Three-quarters of the sample said they used a sealant, and the median bonding success rate was reported to be about 95%.
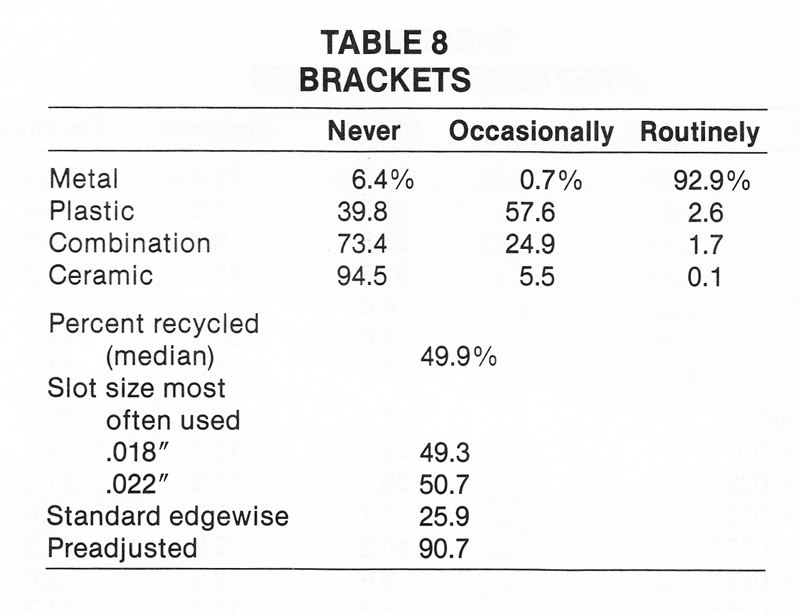
Brackets
A vast majority of the respondents reported using metal brackets (Table 8), but more than half occasionally used plastic brackets. Almost none used ceramic brackets. About 35% of the sample reported recycling at least some brackets, with a median of about 50% recycled. The respondents were almost evenly divided between .018" and .022" slot size. Far more orthodontists reported using preadjusted than standard edgewise brackets.
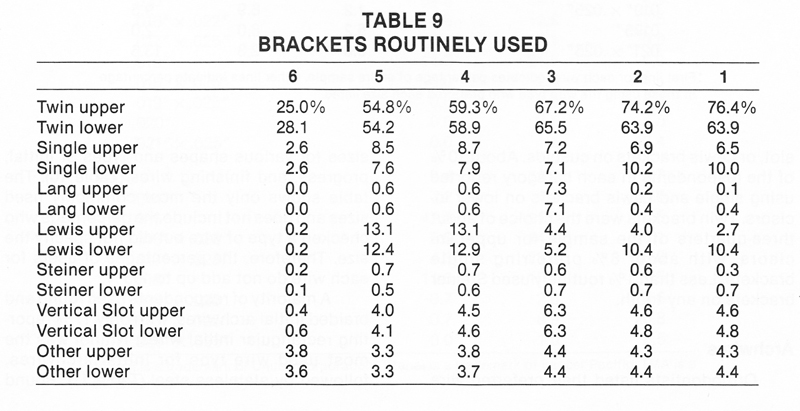
Respondents were asked to circle the teeth on which they routinely used each type of bracket (Table 9). Twin brackets were favored for all teeth, although only a minority of orthodontists said they routinely used any brackets on first molars. Single brackets were used routinely by 10% or less for each tooth. Lewis brackets were the second most popular for bicuspids, with 12-13% using them routinely. Lang brackets were the second most popular for cuspids, though only slightly fewer orthodontists routinely used single, vertical slot, or Lewis brackets on cuspids. About 10% of the respondents in each category reported using single and Lewis brackets on lower incisors. Twin brackets were the choice of about three-quarters of the sample for upper incisors, with about 6% preferring single brackets. Less than 1% routinely used Steiner brackets on any tooth.
Archwires
Orthodontists listed their preferred wire sizes for various shapes and types of initial, progress, and finishing wires (Table 10). The table shows only the most commonly used sizes and does not include the percentage who checked a type of wire but did not specify the size. Therefore, the percentages of users for each wire do not add up to 100%.
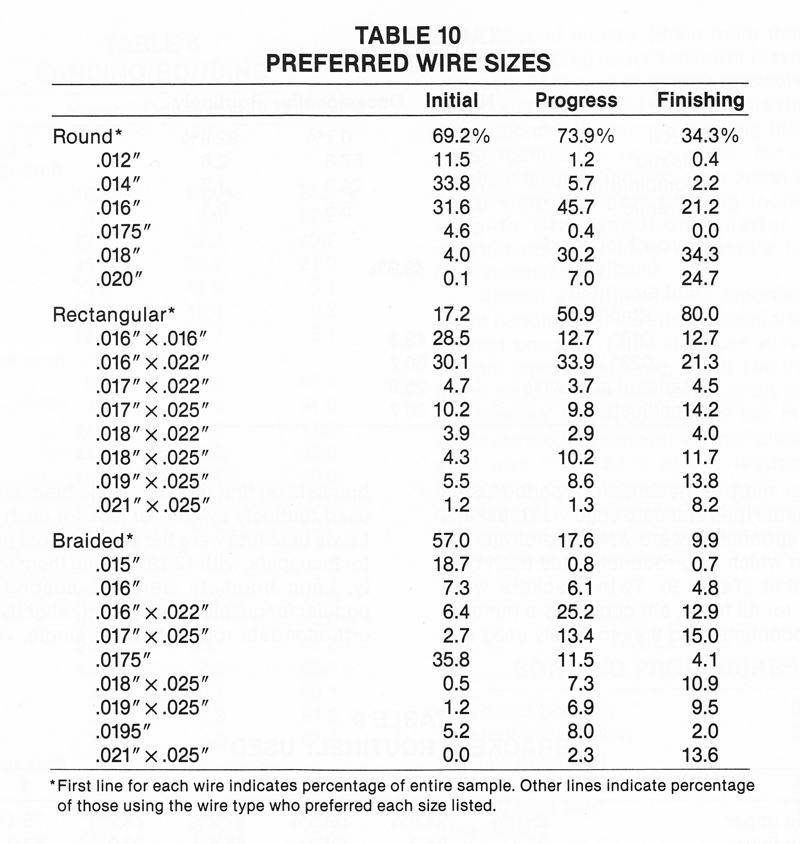
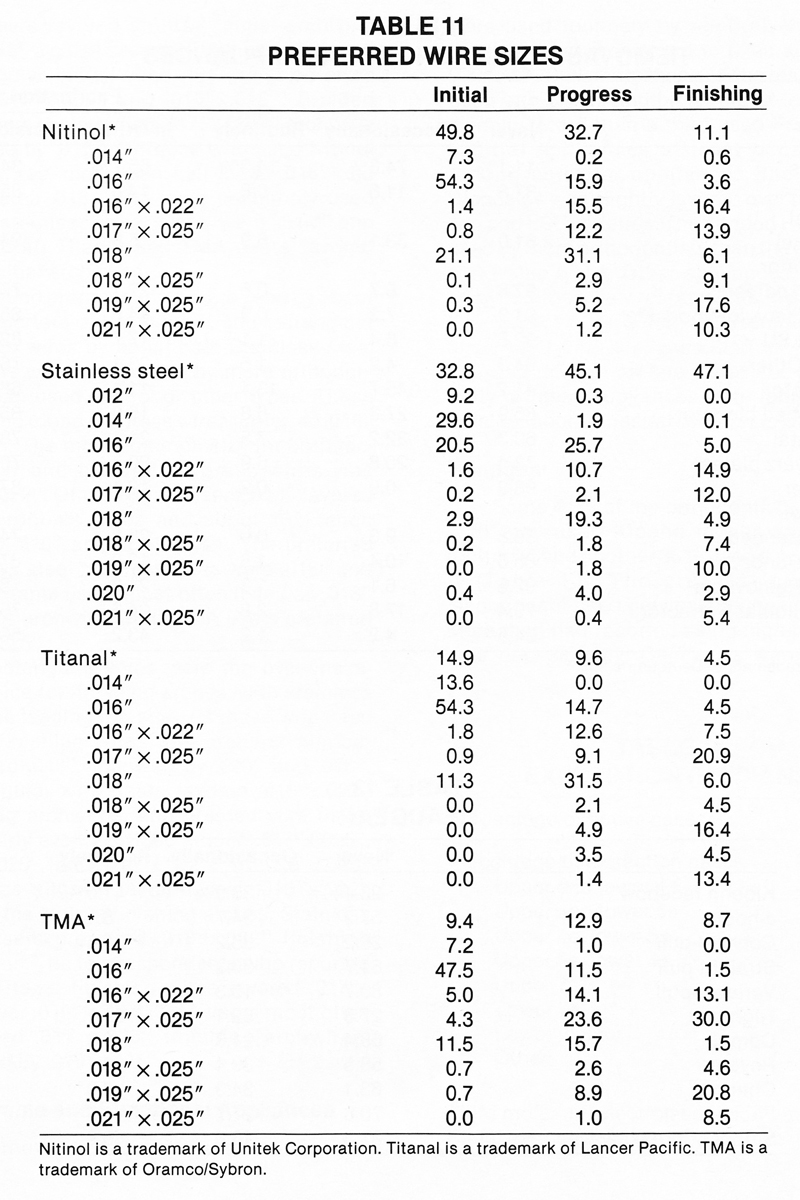
A majority of respondents used round and braided initial archwires, with only 17% reporting rectangular initial wires. Nitinol was the most used wire type for initial archwires, followed by stainless steel (Table 11). Round wire users favored an .014" initial archwire, with .016" a close second. For those who used rectangular initial wires, the preferred sizes were .016"X.022" and .016"X.016". Braided wire users preferred an .0175" initial archwire, followed by .015". Of those who used Nitinol initial wires, more than half listed .016" and 21% listed .018". The most commonly used initial stainless steel sizes were .014" and .016". Both Titanal and TMA users favored .016" initial archwires.
Round progress wires were used by about three-quarters of the sample, and rectangular progress wires by about half. Stainless steel progress wires were used by more orthodontists than used Nitinol or other types. Those who used round progress wires preferred .016" or .018". The most common size for both rectangular and braided progress wires was .016"X.022". Of the Nitinol users, 31% favored .018" progress wires and about 16% each favored .016" and .016"X.022". The preferred stainless steel progress sizes were .016" and .018". Titanal users most often listed an .018" progress archwire, while TMA users preferred .017"X.025".
Rectangular wires were the overwhelming choice for finishing arches, with stainless steel the leading material. Of those who used round finishing wires, the greatest number preferred .018", followed by .020" and .016". Rectangular wire users favored .016"X.022" finishing archwires, and braided wire users were fairly evenly divided among .017"X.025", .021"X.025", and .016"X.022". An .019"X.025" wire was slightly favored over .016"X.022" among the Nitinol finishing arches. Stainless steel users preferred .016"X.022" finishing archwires. The few respondents who reported using Titanal finishing wires favored .017"X.025" over .019"X.025". TMA users most often specified .017"X.025" finishing archwires, followed by .019"X.025".
Removable and Functional Appliances
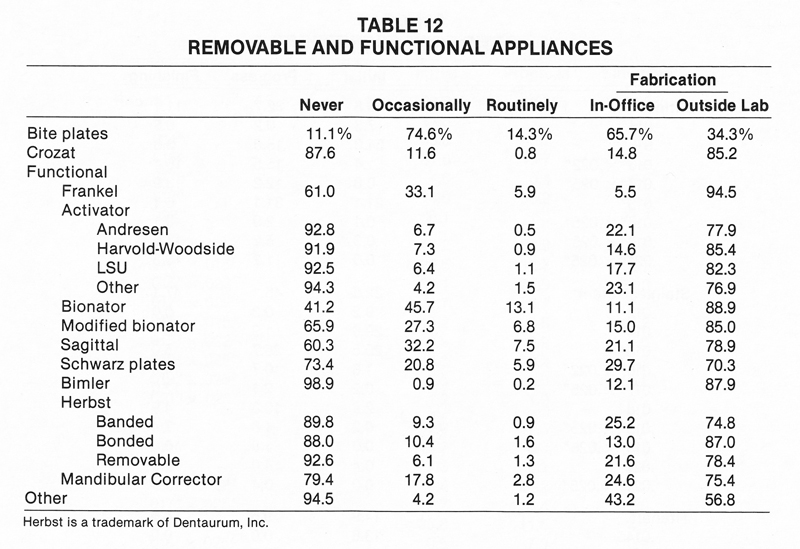
Removable and functional appliances were used routinely by relatively few orthodontists when compared to fixed appliances (Table 12). Still, more than half the respondents used bite plates and bionators at least occasionally. More than a third used Frankel and sagittal appliances at least occasionally. Among activator appliances, the Harvold-Woodside was slightly favored over the Andresen and LSU varieties. The bonded Herbst was used by more orthodontists than the banded or removable types. Other appliances, mentioned by relatively few respondents, were the Active Vertical Corrector, the Hamilton appliance, the LARS appliance, and the Teuscher activator. Except for bite plates, the great majority of these appliances were fabricated by outside laboratories rather than in-office.
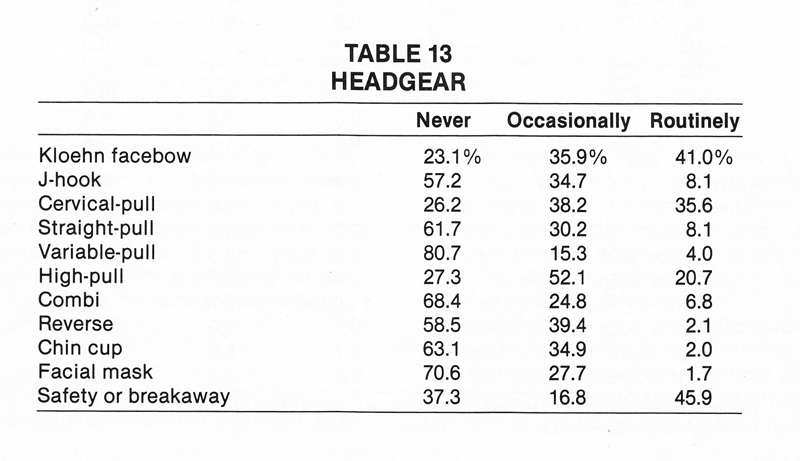
Headgear
Some 41% of the orthodontists surveyed said they used Kloehn facebow headgear routinely, and another 36% used it occasionally (Table 13). The greatest number of respondents used cervical-pull headgear, but more than half reported using high-pull headgear occasionally. Chin cups were used at least occasionally by about 37% of the respondents, and facial masks by about 29%. More than one-third of the sample said they never used headgear with a safety or breakaway feature.
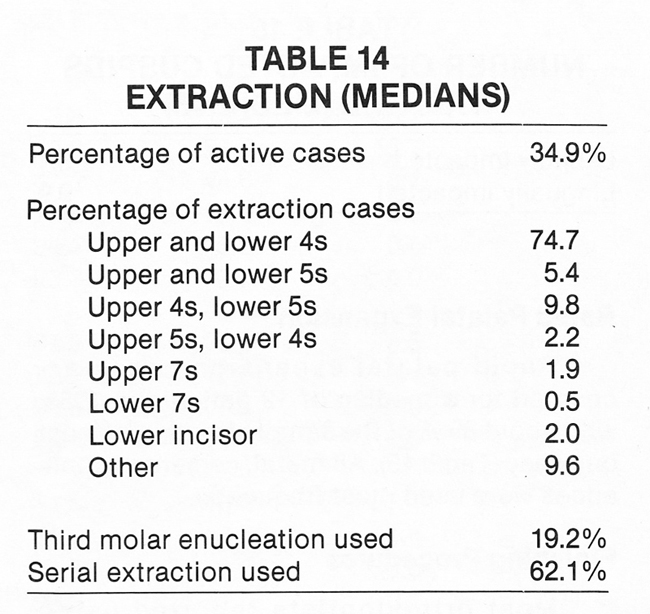
Extraction
About 95% of the respondents reported treating some extraction cases, with the median percentage of active cases about 35% (Table 14). Upper and lower first bicuspids were removed in about three-quarters of the extraction cases. Other extraction combinations mentioned included upper first bicuspids only, and upper and lower first molars. About 19% of the respondents reported using third molar enucleation, and about 62% serial extraction.
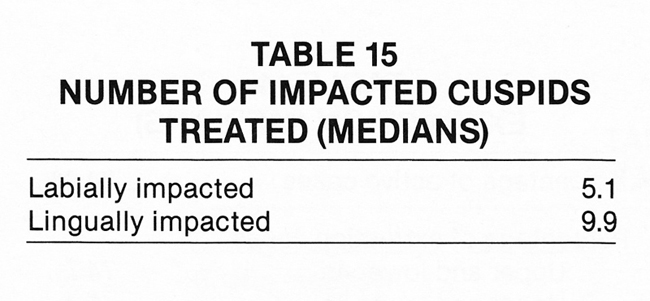
Impacted Cuspids
Labially impacted cuspids were reported by 71% of the sample, with a median of 5.1 treated (Table 15). About 82% of the respondents reported lingually impacted cuspids, with a median of 9.9 treated.
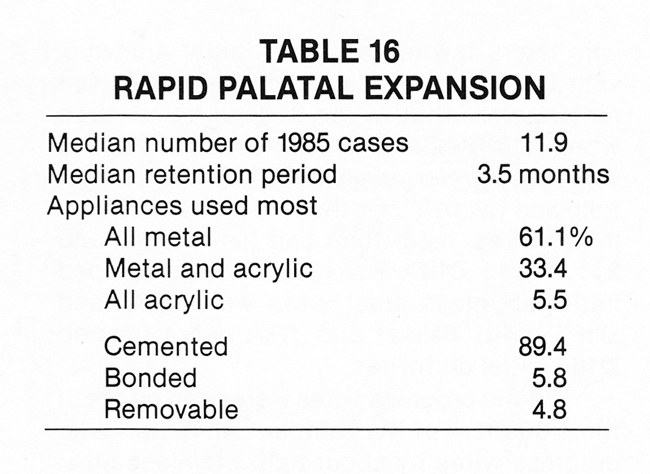
Rapid Palatal Expansion
Rapid palatal expansion cases accounted for a median of 12 patients in 1985, with about 89% of the sample treating at least one case (Table 16). All-metal, cemented appliances were used most frequently.
Finishing Procedures
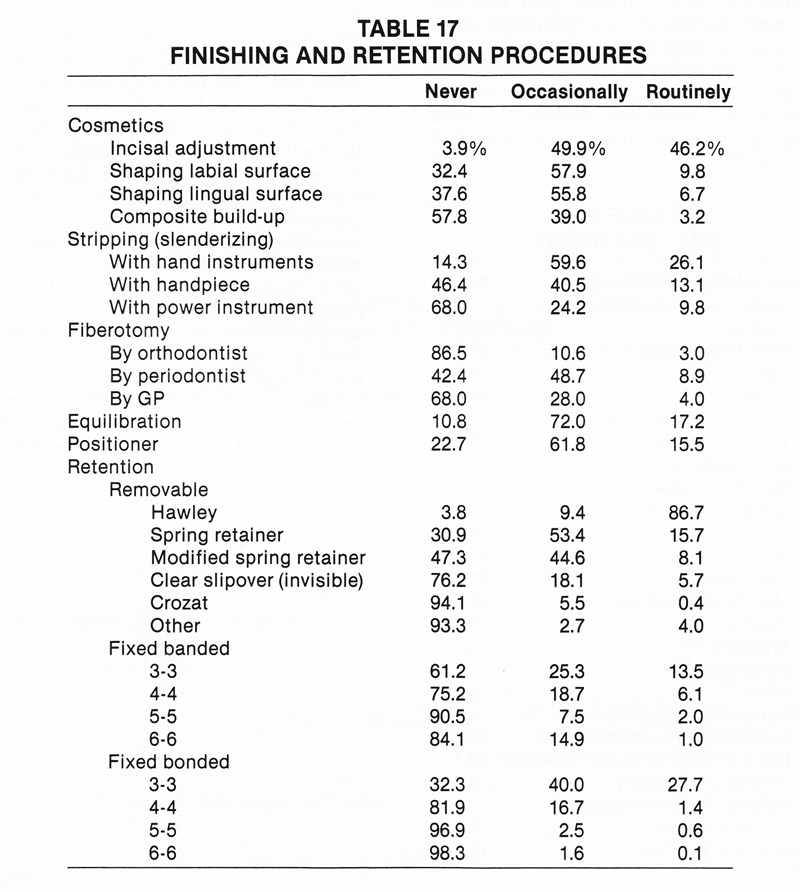
Most orthodontists reported using cosmetic finishing techniques only occasionally (Table 17). About 96% did incisal adjustments at least occasionally, and a majority shaped labial or lingual surfaces at least occasionally. Most respondents never used composite build-ups.
Stripping was performed routinely by nearly half the sample, with hand instruments preferred over handpieces and power instruments. Very few respondents reported routine fiberotomies, but more than half at least occasionally referred patients to a periodontist for fiberotomy.
Equilibration was reported at least occasionally by about 89% of the orthodontists responding, though only 17% equilibrated routinely. Positioners were used at least occasionally by 77% and routinely by 16%.
The overwhelming choice of retainers was the Hawley, routinely used by 87% of the respondents. A majority used spring retainers, modified spring retainers, and bonded 3-3 retainers at least occasionally. The median duration of retention was 24 months for all types of retainers except the bonded 3-3, which had a median of 30 months.
TMJ Treatment
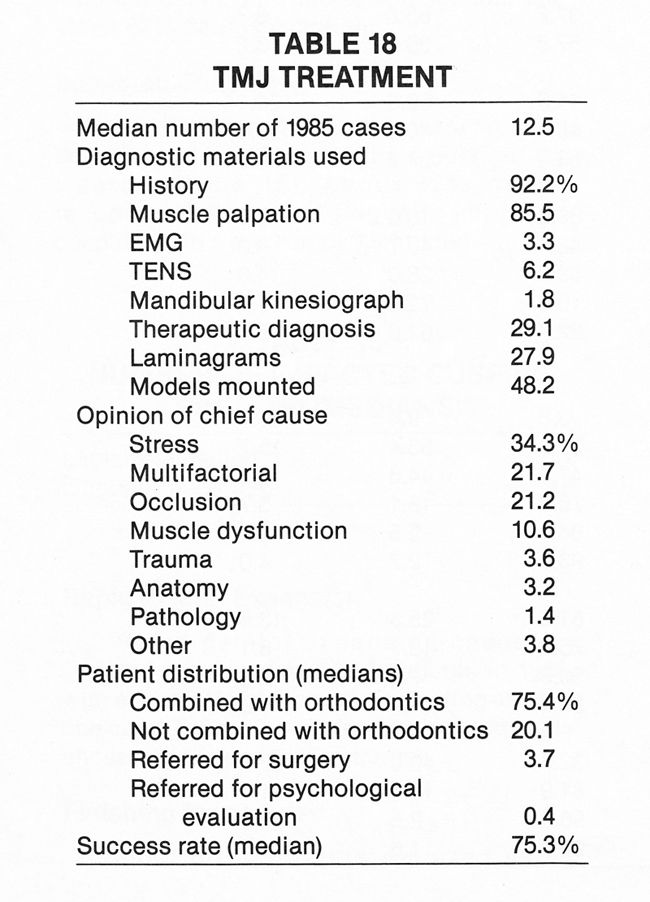
About 70% of the respondents said they treated at least one TMJ case in 1985, with a median of 12.5 cases (Table 18). Most of those who treated TMJ cases used a history and muscle palpation for diagnosis. Nearly half reported mounting models, and more than one-quarter used therapeutic diagnosis and laminagrams. Orthodontists were divided in their opinion of the chief cause of TMJ symptoms. Stress was the leading candidate, but more than 20% of the respondents said symptoms were caused by multiple factors. About 75% of the TMJ patients also had orthodontic treatment. The median success rate was reported as 75%, with success defined as being asymptomatic at least one year after treatment.
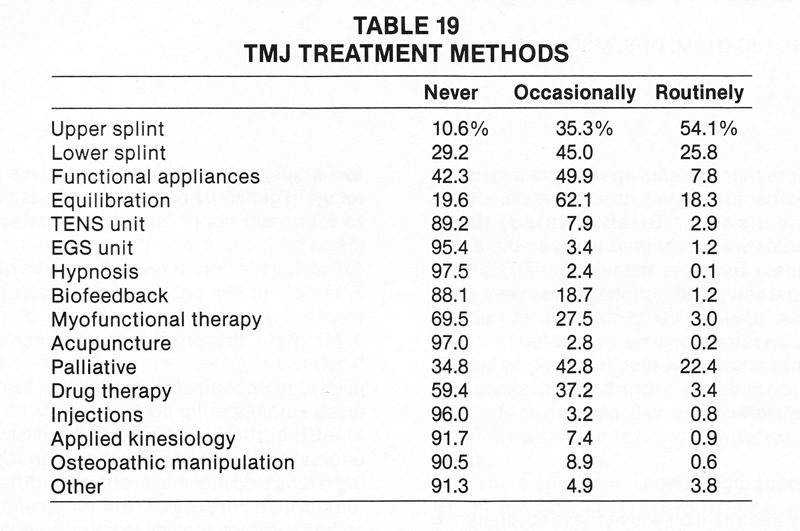
Those who treated TMJ cases used a wide variety of treatment methods (Table 19). Upper splints were used at least occasionally by 89% of the respondents and routinely by 54%. Other methods used at least occasionally by more than half of those responding included lower splints, functional appliances, equilibration, and palliative therapy (reassurance, hot-cold treatment, etc.). Biofeedback, myofunctional therapy, and drug therapy were used at least occasionally by at least 20% of the respondents. Of the orthodontists who prescribed drugs, half specified muscle relaxants, with more than one-third of these listing Valium. Fewer respondents specified anti-inflammatory agents or analgesics. Other TMJ treatment methods mentioned included physical therapy and some form of orthodontics, such as fixed appliances.
Surgical Orthodontic Treatment
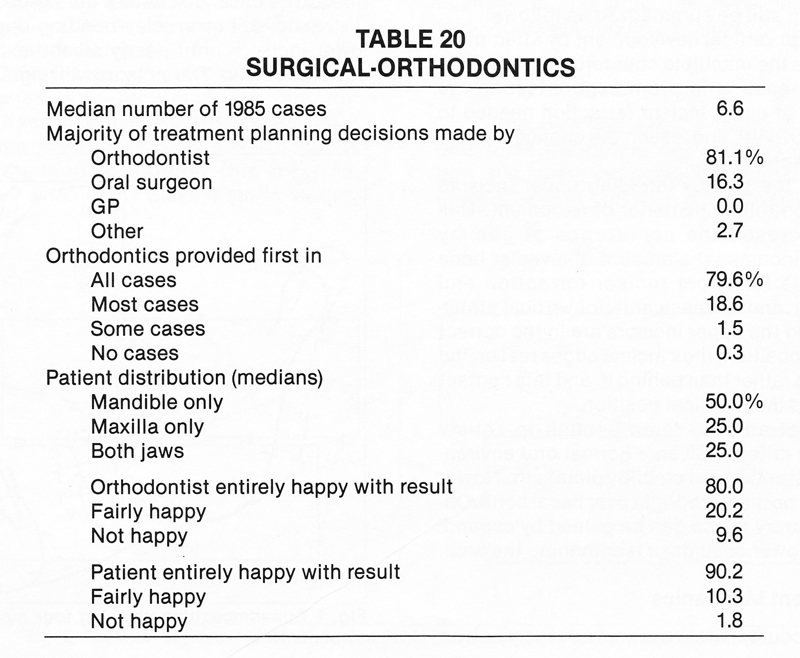
About 81 % of the total sample reported treating at least one surgical-orthodontic case in 1985, with a median of 6.6 cases (Table 20). Most of these said the majority of treatment planning decisions were made by the orthodontist, but about 16% said the oral surgeon made most of the decisions. About 80% of the respondents said orthodontic treatment came first in all cases, and another 19% provided orthodontics first in most cases. Those who treated surgical-orthodontic cases said half their patients had mandibular surgery only, one-quarter had maxillary surgery, and one quarter had surgery in both jaws. Each respondent was asked to divide the cases by the percentages in which the orthodontist and the patient were entirely happy, fairly happy, and not happy with the result. Although the medians add up to more than 100%, it is evident that orthodontists were more critical of the results than the patients were. Orthodontists said they were not happy in a median of 10% of the cases, but they thought the patients were not happy in only 2% of the cases.
-
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Gottlieb is Senior Editor and Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302. Dr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.