JCO Interviews Dr. Bjorn Zachrisson on Excellence in Finishing, Part 1
DR. GOTTLIEB Bjorn, excellence in finishing cases is one of the most crucial aspects of orthodontic treatment. What are your goals in finishing?
DR. ZACHRISSON I have individualized treatment goals for posterior as well as for anterior teeth. I don't think all cases should be finished in the same way. For example, I do not treat a Class III malocclusion to the same result as a Class II malocclusion with regard to molar and bicuspid rotation. In Class II cases, I normally rotate the upper molars and bicuspids to the distal so they occupy less arch length. In Class III cases, I may rotate these teeth in a mesial direction. The same would be true when an entire maxillary arch is moved forward to close the space for congenitally missing lateral incisors (Fig. 1). Furthermore, I like to overtreat certain features of the original malocclusion in the anterior region. This creates differences at the end of treatment, although I might expect overcorrected teeth to reach a more or less ideal relationship in the long run. I also feel it is my job as an orthodontist to find the ideal arrangement for the six upper and lower anterior teeth. If they do not naturally have the potential to look really nice, then I change their shape, width, or axial inclination. I try to create a long-term perfect result for these teeth, and that is my main goal in treatment. I go along with Dick Riedel, who says that retention is not a problem in orthodontics-- it is the problem.
Similar articles from the archive:
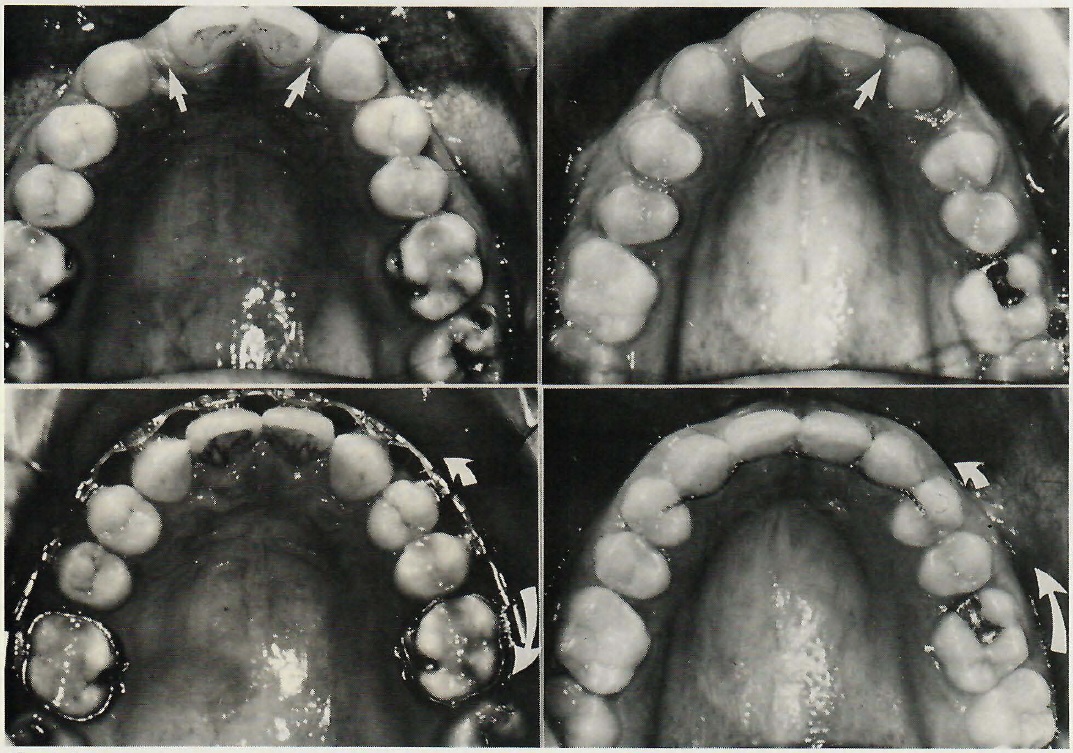
Fig. 1 Two cases with congenitally missing lateral incisors, showing good mesial rotation of first bicuspids during treatment. The first molars are rotated differently, depending on whether a Class I (left) or Class II (right) molar occlusion is desired.
DR. GOTTLIEB Let's take a Class II malocclusion. How do you set your treatment goals?
DR. ZACHRISSON Let me show you a chart of a difficult Class II case (Fig. 2). You can see how I make my cephalometric tracing and analysis. I measure maxillary and mandibular prognathism relative to Frankfort and SN, and the convexity in millimeters. For incisor position, I measure lower incisors to APo plane in millimeters, lower incisor angulation to APo and mandibular planes, interincisal angle, and upper incisors relative to Frankfort and SN. I measure mandibular plane relative to Frankfort and SN, Frankfort relative to SN, inclination of skull bases, and upper and lower face heights. And that's about what I need. For soft tissue analysis, I use a few Holdaway measurements-- the nose, the upper lip thickness, the lip strain, and the chin. In this case, the lower incisors are 2mm behind the APo line, and the lower lip is 4mm behind the esthetic plane. My thinking is that the lips are on the thin side and I have to be careful not to destroy the profile. The lower lip is resting on the incisal edges of the upper incisors. If I am going to move the upper incisors inward, I have to be careful not to retract the lip. The lip strain is 6mm, so I might be able to move in about 6mm without changing the lip relationship. I may have to move the lower incisors slightly forward in this case. Then the upper incisors will determine the interincisal angle. If I know where I want the lower incisors to be, and if I don't expand the intercuspid width, the lower arch is more or less given, and it is then just a question of matching the upper arch to the lower.
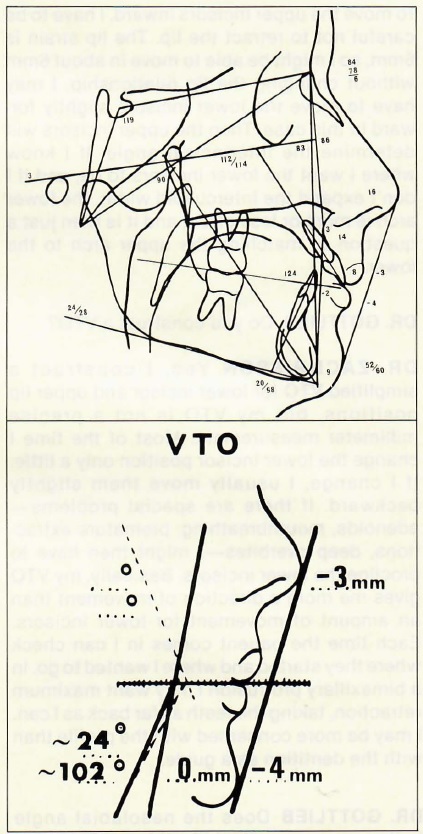
Fig. 2 Routine tracing and VTO of Class II case.
DR. GOTTLIEB Do you construct a VTO?
DR. ZACHRISSON Yes, I construct a simplified VTO for lower incisor and upper lip positions, but my VTO is not a precise millimeter measurement. Most of the time I change the lower incisor position only a little. If I change, I usually move them slightly backward. If there are special problems-- adenoids, mouthbreathing, premature extractions, deep overbites-- I might then have to procline the lower incisors. Basically, my VTO gives me more a direction of movement than an amount of movement for lower incisors. Each time the patient comes in I can check where they started and where I wanted to go. In a bimaxillary protrusion I may want maximum retraction, taking the teeth as far back as I can. I may be more concerned with the profile than with the dentition as a guide.
DR. GOTTLIEB Does the nasolabial angle bother you on a patient like this one?
DR. ZACHRISSON Of course. Anyone who does not take that into consideration can destroy the face, and the face is definitely more important than the dentition.
DR. GOTTLIEB You can't do a lot about it if you are going to have to bring those upper incisors back. At this age, which is close to 10, would you consider a functional appliance?
DR. ZACHRISSON In a case like this, I would try to use the principle of preventing the eruption of the upper first molars and freeing the occlusion so the mandible is free to move forward as much as it can. I have become strongly influenced by recent studies by Melsem, Sinclair and Little, and others on the importance of vertical control of upper first molars in managing severe sagittal discrepancies. I would not place a Herbst or a Frankel, because I use very few of those. My goal would be to influence the differential growth process between the growth of the condyle, the growth of the alveolar process, and the eruption of the upper teeth. We are presently testing different approaches to holding upper molars vertically and freeing the occlusion to get the maximum forward effect out of the normal mandibular growth.
DR. GOTTLIEB How do you decide where you want to locate lower incisors in relation to the APo plane?
DR. ZACHRISSON The amount of retroclination is largely determined by the type of soft tissue profile change that I want to induce. I use a simplified Holdaway analysis based on upper lip thickness and strain to calculate the optimum position and contour of the upper lip post-treatment. it may be more difficult to decide on lower incisor proclination. A number of studies, including our own, of untreated samples of ideal occlusions have shown that the lower incisors are more proclined than our usual norms. In our population, the lower incisors were 2.2mm on average ahead of APo plane (Fig. 3). We thought our people would have more retruded incisors than, say, the Smile of the Year Contest winners in the Los Angeles population, but they did not. The good things we learned from our study were, number one, the lower incisors on average were about 2mm ahead of the APo plane; number two, the interincisal angle in these patients was small (127°); and number three, most of these ideal patients were low angle or brachycephalic cases. In none of them were the lower incisors behind the APo plane. If we have a patient with incisors 2-3mm behind the APo plane, I would ask myself whether I want to move them forward, but first I would ask myself why these lower incisors are in that position. If I can find a biological reason for it-- a thumbsucking habit, a mouthbreathing habit due to adenoids, premature extraction of the deciduous cuspids, or a very deep overbite-- then I believe we have a biological reason to procline those lower incisors to somewhere near the APo plane and have stability. I try to find a biological explanation, and if I can't I am hesitant to procline those incisors.
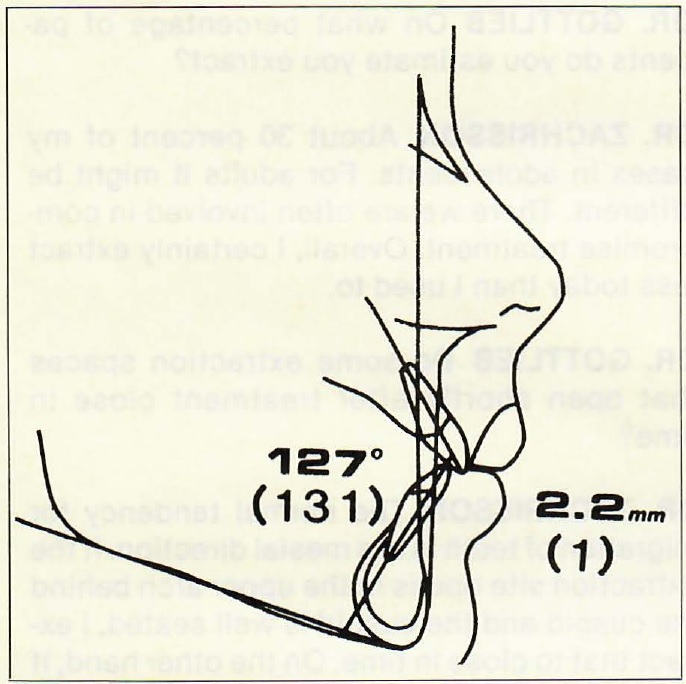
Fig. 3 Lower incisor protrusion (in millimeters to APo) and interincisal angle in Norwegian children with untreated ideal occlusions, compared to commonly used standards (in parentheses) for Scandinavian adolescents.
DR. GOTTLIEB People seem to like front teeth protruding more than orthodontists do.
DR. ZACHRISSON To most people protruding incisors mean youth. A slightly full profile is a younger profile than a flat profile. The reason is that the nose and chin grow more than the lips, so if you have a profile that is slightly protrusive it is an indication of youth. The incisor position in space is reflected on the profile, and most laymen like slightly protruding profiles. You must discuss the pros and cons of that with the parents and patients. Many patients come to my office with a prejudice against tooth extraction because they don't like the flat profiles they may have seen as a result of extraction. That is one reason I am reluctant to extract lower first bicuspids. Routine extraction of first bicuspids followed by lots of Class II elastics to close the spaces can sometimes result in a flat profile, large interincisal angles, high lower face, tipping of the occlusal plane, and a lot of unnecessary and undesirable side effects; and if the patient does not use the Class II elastics, or if they are contraindicated because of root resorption tendencies, you have all kinds of problems.
DR. GOTTLIEB How much arch length can you get out of lower second bicuspid extractions?
DR. ZACHRISSON I think you can get enough, because most of the time the crowding in the lower arch is not substantial. You can handle a moderate amount of crowding very easily with second bicuspid extractions. What I like about it is that the appliance is very simple-- just a straight wire and elastomeric chains. One cuspid and one bicuspid are matched pretty much against one first molar. You can easily get 50/50 use of the bicuspid space. If you want to move the first molar farther forward, you can add a light Class II elastic (3 ounces) to give an additional force to the molar, with very little side effect to the upper arch. It is a very simple and easy treatment. If you have a very severe crowding or a Class III tendency you may extract first bicuspids. I used to extract first bicuspids in the lower arch almost exclusively, but today that is rare-- 75 to 80 percent of my lower arch extractions are second bicuspids, and I am much happier with the treatment results. The treatment is also much less dependent on the cooperation of the patient.
DR. GOTTLIEB If you have significant crowding and protrusion of the lower anterior teeth, do you then extract first bicuspids?
DR. ZACHRISSON Yes. It's simply a matter of having the space available where it will do you the most good.
DR. GOTTLIEB Do you find any problems with second bicuspid extraction?
DR. ZACHRISSON We have psychological barriers to second bicuspid extraction, rather than any solid indications that it should not be done. The only problem I have with regard to second bicuspid extraction is that I don't like the morphology of the lower first bicuspids-- they are often small teeth with small lingual cusps. But as far as I can see there are no contraindications from a functional point of view, from a contact point of view, from an esthetic point of view, or from a tooth size discrepancy point of view that would prevent me from using that approach; and as I mentioned, the treatment is simple, predictable, doesn't depend so much on the cooperation of the patient, and gives better lower incisor torque and interincisal angles and better profiles. There are a lot of pluses and only a few minuses. If you really don't like the anatomy of the first bicuspid, you can build a composite lingual cusp, but I never do that.
DR. GOTTLIEB It can be a major mistake to extract four first bicuspids when you have lower incisors that are behind the APo line. Then you can really create a flat face and destroy a patient's profile.
DR. ZACHRISSON Those are orthodontic faces that you rarely see normally. Patients are starting to realize that.
DR. GOTTLIEB On what percentage of patients do you estimate you extract?
DR. ZACHRISSON About 30 percent of my cases in adolescents. For adults it might be different. There we are often involved in compromise treatment. Overall, I certainly extract less today than I used to.
DR. GOTTLIEB Do some extraction spaces that open shortly after treatment close in time?
DR. ZACHRISSON The normal tendency for migration of teeth is in a mesial direction. If the extraction site opens in the upper arch behind the cuspid and the cuspid is well seated, I expect that to close in time. On the other hand, if the second bicuspids are well seated and the cuspids are forward, that will not correct by itself. In the lower arch, if you have taken out lower second bicuspids and you have moved the lower molars forward-- and if the occlusion on the first bicuspid and cuspid are acceptable-- I expect that the molar will come forward in time, and I don't necessarily do anything about it. Mesial migration in the mandible is different from that in the maxilla, because there is less mesial movement of the entire dentition. Mesial migration of lower first molars tends to be influenced by the eruption of the second and third molars.
DR. GOTTLIEB You don't routinely try to prevent reopening by going across the extraction site with a bonded retainer?
DR. ZACHRISSON In adults I do, because our clinical experience indicates that the relapse tendency is greater in adults than it is in children. So in most adult patients, if I have extracted bicuspids, I will bond a thin retainer and cross the extraction sites (Fig. 4). In children that does not seem to be required.

Fig. 4 Thin retainer wire (.0215") bonded to hold upper first and lower second bicuspid extraction sites closed in adult patient.
DR. GOTTLIEB Sometimes an overextended filling is placed to make contact over an open extraction site.
DR. ZACHRISSON I haven't seen too much of that, but something is known about the effect of open contacts on the periodontium. A study made by Jernberg and co-workers indicates that if you have an open contact you may see some attachment loss. There are other studies by Silness and co-workers that indicate that you don't see that type of thing. It may have to do with how large the space is. In any event, the indication for an overextended filling in my office would be in treatment of a spaced dentition where I have put in a six- or eight-unit bonded retainer and see spaces opening behind the retainer. This may take place after three or four months, and it could remain like that for several years. In those instances, you could use overextended fillings or crowns to eliminate those spaces. I see little need to do that on a routine basis in treatment of adolescents.
DR. GOTTLIEB Do third molars cause irregularity of lower anterior teeth?
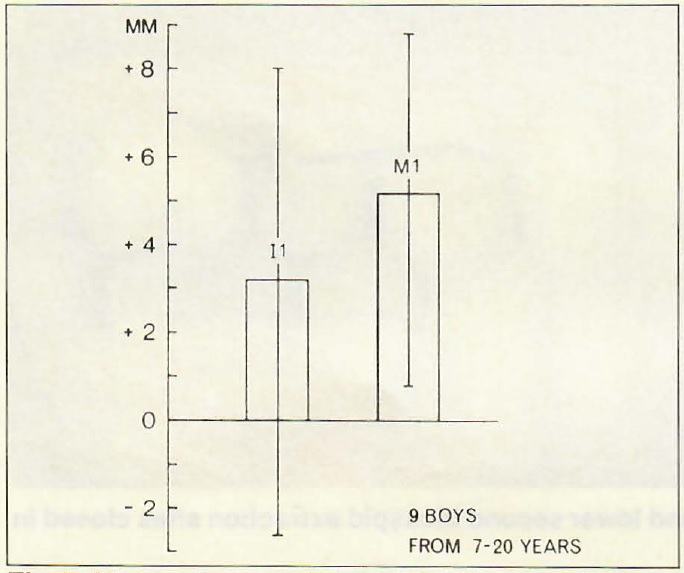
DR. ZACHRISSON We do not have the exact answer to that question, but my analysis of present knowledge is that third molars do exert a pressure and do influence the normal mesial migration of the molars. If they are impacted or if the third molars are very far away from the second molars, I don't think that is true, but if they are erupting and touching the second molars it is hard for me to see how they would not have an influence on the normal mesial movement of the first molars. This would have to lead to more crowding in the anterior region. Bjork indicated that, on average, from 7 to 20 years of age the first molar moves forward 5mm relative to implant lines (Fig. 5), and I think that mesial movement can be influenced by the third molar-- but not necessarily in the sense that we have been thinking about. We have to think about the three-dimensional picture and not just two-dimensionally along an occlusal plane. It was interesting to see in Bjork's study that while, on average, his first molars came forward 5mm, on average the lower incisor only came forward 3mm (Fig. 5). That may be one explanation of late crowding in the lower arch. Recent studies by Richardson and Schwarze have shown that if you extract second or third molars, you reduce the normal mesial movement of the first molars and the teeth forward of them.
Fig. 5 Mean values and ranges for the mesial migration of lower first molars (M1) and lower central incisors (11). (From Bjork, A. and Skieller, V.: Normal and abnormal growth of the mandible: A synthesis of longitudinal cephalometric implant studies over a period of 25 years, Eur. J. Orthod. 5:1·46, 1983.
DR. GOTTLIEB Is there any evidence about the predictability of enucleating third molars?
DR. ZACHRISSON It has been shown convincingly by Richardson that it is hard to predict at an early age whether third molars will erupt, but we don't do that type of prediction. When we do germectomy of third molars, it is always in connection with a nonextraction treatment plan where one could eliminate one of the factors that might result in relapse, or we want to use the third molar space to change the eruption paths of the first and second molars.
DR. GOTTLIEB What are your considerations for increasing arch length?
DR. ZACHRISSON I divide the arch into segments-- an incisor segment, a cuspid segment, a bicuspid segment, and a molar segment. In the majority of cases, I would not procline incisors to gain arch length, except under very special circumstances as we discussed previously. Most of the time I either maintain the lower incisors where they are at the start of treatment or move them slightly inward-- except, of course, if you have a protrusive profile.
DR. GOTTLIEB How often do you try to gain space for crowded lower incisors with lip bumpers?
DR. ZACHRISSON There are a number of studies on it. Lip bumpers do not all act the same. Some orthodontists claim they don't get too much proclination of lower incisors when the lip is held away from them. They position the bumper high so that they still get some lip action against the lower incisors. I don't think you can avoid at least some slight proclination of the lower incisors, which would not be desirable in most instances. If one wants to create arch length with a lip bumper, I don't think it should be done by moving the lower incisors forward, but by uprighting molars that may be tipped forward and by lateral expansion of molars that have been tipped lingually. One deterrent to using lip bumpers is that you need special attachments on the molars. Most orthodontists don't have a tube for the lip bumper in their usual setup, and bands would have to be replaced. More lip bumpers might be used if there were a transfer tube mechanism that didn't require replacing the molar bands. Recently, many orthodontists have become interested in gaining arch length by trying to change the molar eruption path to a more vertical one, and a lip bumper is well suited for that purpose. I think we will be more concerned in the future with the mesiodistal position of lower molars relative to the vertical plane than we are today, plus various methods to hold the leeway space.
DR. GOTTLIEB Do you increase the inter cuspid distance?
DR. ZACHRISSON I rarely change the intercuspid distance. All reliable studies I know of show that expansion of the lower intercuspid distance will relapse with time. You might be able to do that in some Class II, division 2 cases, but even in those cases I think the gain over the long term is no more than a half a millimeter to a millimeter. So one of my keystones is not to expand the intercuspid distance if it is in the normal range, which is about 26mm in our population.
DR. GOTTLIEB If you extract lower first bicuspids and move the cuspids back, are you moving them into a wider portion of the arch?
DR. ZACHRISSON This has been discussed by orthodontists for years. As you move the cuspids on the arch curve, you don't move them great distances. In theory you should be following the curve to what seems to be a wider section of the arch. If you were able to use the entire extraction site for the cuspid, then you could get away with some expansion, because you would be moving the cuspid to a wider portion of the arch. But most of the time in correction of a Class II, the farther back you move the lower cuspids, the farther back you have to move the upper cuspids. The more distally you move the lower cuspids, the more distal you are making the case. In most instances, therefore, I think the lateral dimensions in this region will not reflect a significant amount of increase. So you can say that the intercuspid width should not be increased.
DR. GOTTLIEB You would rather not change intercuspid distance very much, and solve the residual crowding by stripping lower incisors?
DR. ZACHRISSON Certainly, and particularly if I have triangular-shaped teeth. My deciding factor when it comes to solving arch length with stripping depends not on enamel thickness, not on the Peck and Peck ratio or any other measurement, but simply on the morphology of the teeth. If I have triangular-shaped lower incisors, I may reshape those teeth and in doing so regain a substantial amount of arch length. On the other hand, if the lower incisors are parallel to start with I might not be able to strip them at all. That would just destroy them. That would be my limiting factor.
DR. GOTTLIEB What about expansion farther back in the arch?
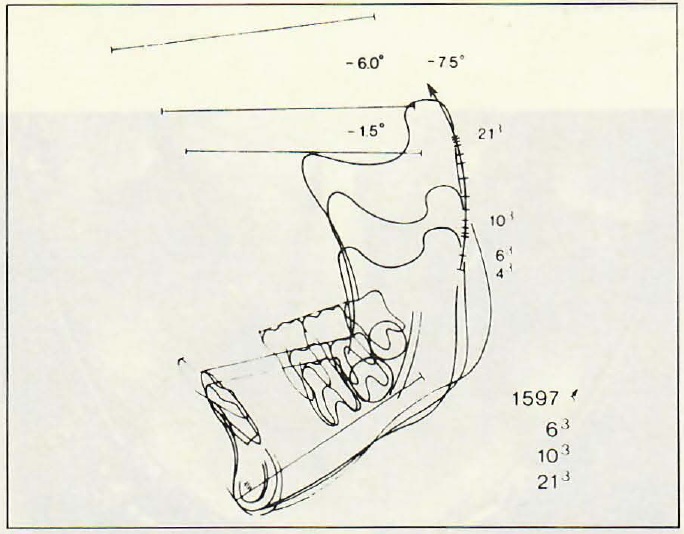
DR. ZACHRISSON The chance for stable expansion increases the farther back in the arch you go. You can expand lower first bicuspids, and long-term results indicate you can expand first molars laterally to a considerable degree and expect that to remain stable. But we are only talking about one plane of space. The plane of space that I think is most interesting now is the vertical plane. Research by Bjork and Skieller indicates that the normal eruption from 10 to 20 years of age is substantial. In the lower arch it may be up to a centimeter in the vertical/mesial direction (Fig. 6). There we have a source of arch length potential that I have not been concerned with previously. When we are talking about gaining arch length and converting extraction cases to nonextraction cases, we are usually only looking at the lateral plane. Guiding the eruption of the lower molars in a more distal or vertical direction than normal will provide us with space that can be used in resolving crowding in the lower arch (Fig. 7).
DR. GOTTLIEB What kind of an appliance do you use to do that?
DR. ZACHRISSON It doesn't matter very much. There are a number of appliances you could use to influence the eruption and position of the lower molars. You can use a utility arch or a lip bumper. I often use a rectangular wire with a closed coil between the molar and the cuspid, and allow the bicuspids to erupt in a more distal direction while holding the molars back at the same time (Fig. 8). You might want to use light Class III elastics. There are many ways you can do it. In fact, Baumrind recently demonstrated how appliances conventionally employed to retract the maxilla-- cervical and high-pull headgear-- lead to distal crown tipping of the lower first molar. I am suggesting that one should go for the principle. To me that is a more promising and interesting view of orthodontics than trying to get away with lateral expansion.
Fig. 6 Mandibular tracings of case with forward rotation of mandible, showing "average" molar and incisor eruption pattern relative to implant line. (From Bjork and Skieller, op. cit.)
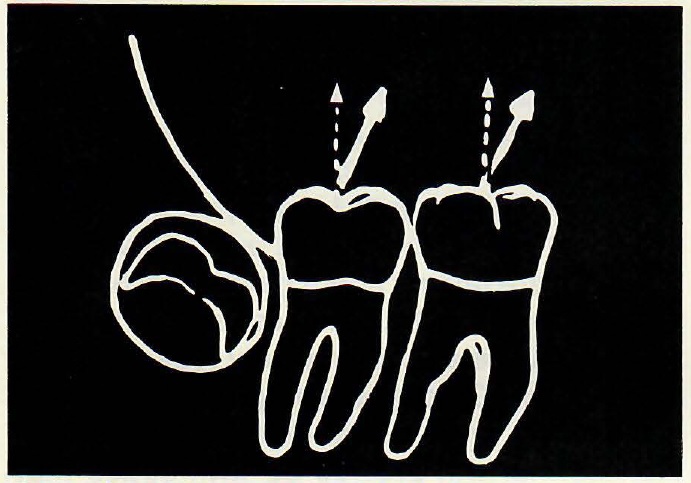
Fig. 7 Guiding eruption of mandibular molars in a more distal vertical direction (broken arrows) than normal (solid arrows) to gain arch length more anteriorly.
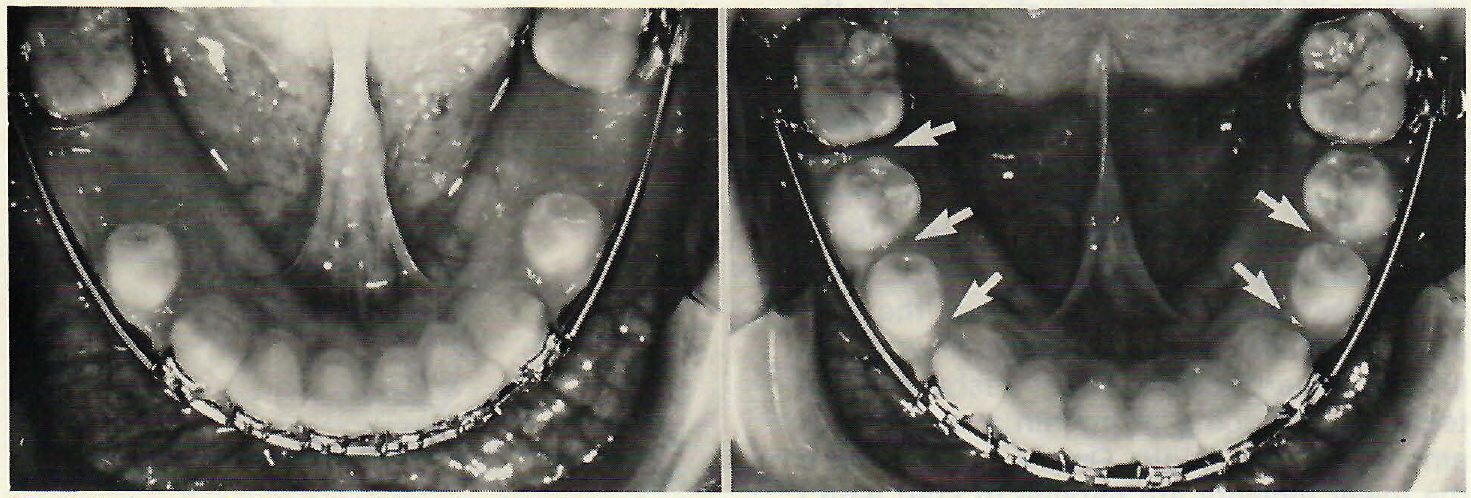
Fig.8 Using an .016" x .022" flat wire to hold leeway space and allow mandibular bicuspids to erupt more distally provides space (arrows) to resolve anterior crowding.
DR. GOTTLIEB Is maintenance of arch length in cases with deep curves of Spee one of the beneficial effects of using that technique?
DR. ZACHRISSON That would be one example of the value of the technique-- to make sure that the lower molars do not come forward as you level the curve of Spee and that the lower incisors are not protruded. If no precaution is taken, you will increase the arch length at the expense of incisor protrusion. It all depends on the case, of course. If you have a deep curve of Spee and lower anteriors inclined inward, you might just take a utility arch and throw lower molars back and lower incisors slightly forward. Every case has to be analyzed by itself. Given two deep overbites that look the same, cephalometric analysis may show that in one case the lower incisors are overerupted and in the other the upper incisors are overerupted. In the latter case you may have a gummy smile and will have to intrude the upper arch. The other case should be diagnosed differently, treated differently, and retained differently.
DR. GOTTLIEB Do you ever intrude lower incisors?
DR. ZACHRISSON Yes, but most of my archwires are relatively flat. I don't put tipback or much reverse curve of Spee into my archwires. What concerns me most in leveling is the contact relationship of the lateral incisor and the cuspid. I check the patient from in front. I like to see the cuspid tips a millimeter or so above the incisal edges of the four lower incisors. That means that I frequently make a stepdown bend between the cuspid and the lateral, rather than using a reverse curve of Spee or tipback bends. I may add base arches in tough deep overbite cases.
DR. GOTTLIEB Do you intrude teeth as freely in adults as you do in children?
DR. ZACHRISSON With proper technique and force, deep overbites can be treated satisfactorily in all age categories. However, you obviously cannot play on differential eruption methods if teeth are no longer erupting. So you might say that deep overbites can be more difficult to treat in older patients.
DR. GOTTLIEB Do you pay any special attention to their periodontal condition when you do that?
DR. ZACHRISSON Yes. There is experimental evidence that intrusion can convert supragingival plaque to subginginval plaque. If it is left there, it can lead to periodontal destruction. Therefore, it makes good sense whenever we intrude teeth in adults, and particularly in adults with periodontally involved teeth, that we see that the plaque is removed professionally.
DR. GOTTLIEB Is there any functional significance to the curve of Spee? We automatically level the curve.
DR. ZACHRISSON The tendency is for a percentage of the curve to return after treatment. I flatten the curve of Spee except in open bites. One consideration is that I prefer not to use Class II elastics against the curved dentition. It could encourage arch collapse. The flat occlusal plane will settle into a mild curve of Spee, which should meet static and functional goals.
DR. GOTTLIEB Of course, if the curve of Spee returns, a certain amount of overbite automatically returns.
DR. ZACHRISSON Yes, and if it does so excessively you are going to have reduced arch length and a tendency for irregularity to recur. I am using flat wires and securing correct contact relationships, and retaining differentially with bonded wire retainers. That is all I think is possible to do. As we study cases long term, we may see more return of the curve of Spee than we like. Still, I feel what we are doing is the best we can do.
DR. GOTTLIEB Do you measure torque or do you eyeball it?
DR. ZACHRISSON There are a number of factors that have to be taken into consideration, but basically I decide from an esthetic point of view how much torque the upper incisors need. My ideal goal is an interincisal angle around 125°, which I believe provides the best opportunity for stability and esthetics.
DR. GOTTLIEB Do you take a progress ceph to check the torque angulation?
DR. ZACHRISSON I take a cephalogram about three-quarters of the way through treatment, while the appliances are still on, to check the axial inclination of the incisors; in an extraction case, just before the extraction sites are completely closed. I can supplement my clinical judgment with cephalometric judgment while I still have some time to do something about it. I may see from the cephalogram that I need to torque the upper incisors more to get the interincisal angle and esthetic result that I am shooting for. When I compare the lower incisor position to my VTO, I may see that I was 2mm ahead of APo pretreatment and I planned to maintain that, but now at the end of treatment I am 3mm ahead of the APo plane. That means no Class II elastics. If the same case was - 1mm to the APo plane, that would call for continuous use of heavy Class II elastics and maybe rule out headgear. So the progress film gives me some clues on how to finish the case.
DR. GOTTLIEB Do you also take a panoramic x-ray at that time?
DR. ZACHRISSON Yes. Many times it is hard to eyeball the axial inclinations of all teeth, and I often see things in the panoramic x-ray that I didn't see in the mouth. It may be the inclination of the teeth next to extraction sites or of the lateral incisors, but it certainly is helpful to me to check those points while I still have a chance to do something about them.
DR. GOTTLIEB Do you overtorque?
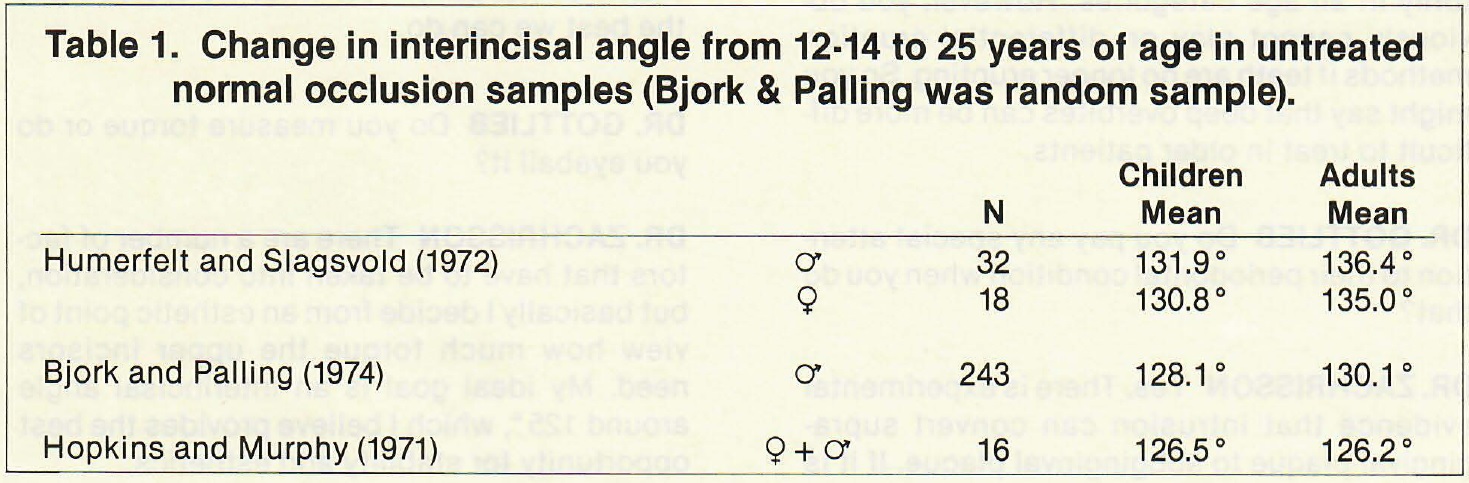
DR. ZACHRISSON There are two situations that I do not like to overcorrect. One is the axial inclination in extraction sites and the other is torque. In extraction sites, I try to place the teeth in an ideal rather than in an overcorrected position, and I do the same with torque. The reason I do that in extraction sites is, as Harry Hatasaka showed, if you overcorrect the axial inclination in extraction sites these teeth may never correct themselves. My clinical experience is that torque also remains pretty much where you leave it. In fact, smaller interincisal angles seem to have a greater tendency to remain unchanged over long periods of time. It is interesting to me to compare age changes of the interincisal angle in different studies of untreated normal occlusions(Table 1).For example, in the Smile of the Year Contest sample, the interincisal angle at age 10-12 was 126°, and it remained the same when these patients were 20-25 years of age. In other studies in which the interincisal angles in adolescents were 128°, these have had small increases. In cases from samples where interincisal angles were 131° or 132° at 10-12 years, there were increases to about 136° or so. So there are some indications that smaller interincisal angles may provide a better platform for the teeth to occlude on, as Schudy pointed out several years ago. Therefore, I think it makes good sense to try to treat to interincisal angles in the 125° range if at all possible. I don't know if we should call that overtorque, but if I have a choice to select the interincisal angle in a Class II case, I would aim to finish below 132 ° rather than above. The real problem is inadequate torque-- up to 150 ° and more-- which I think is an invitation to long-term relapse.
DR. GOTTLIEB Do you feel that the interincisal angle retains overbite corrections?
DR. ZACHRISSON I only have clinical evidence to back it up, but statements made by Schudy, Ricketts, and many others indicate that is the case. It seems to me that the larger the interincisal angle, the greater the chance for a deep overbite to relapse. As it does, only two things can happen. There will either be some crowding in the lower arch or spacing in the upper arch.
DR. GOTTLIEB Do you generally overcorrect overbite to edge to edge?
DR. ZACHRISSON I used to overcorrect deep overbites into open bites, but I don't do it any more, since some of them did not relapse to adequate overbite. Nowadays, I do overcorrect deep overbites, but maybe to a 1mm overbite and then let them relapse to 2-3mm.
DR. GOTTLIEB What if the overbite wants to relapse further?
DR. ZACHRISSON I am not afraid of the deep overbite itself as long as the patient occludes on teeth. A deep overbite of a couple of millimeters more than the ideal is, in my opinion, not necessarily an indication that something has to be done. However, the available space for the lower incisors decreases as overbite increases, as pointed out by Swain, and overbite relapse is thus frequently associated with lower incisor crowding or upper incisor spacing, which may be objectionable to the patient.
DR. GOTTLIEB Do you see relapse of torque?
DR. ZACHRISSON As I mentioned, relapse of torque is not that frequent. Of course, there are changes in growing patients, but I don't overtorque with the feeling that the torque is going to be reduced with age. I torque the teeth to the angle that I like to see. What concerns me is undertorque, which I believe should be avoided as much in the lower as in the upper arch (Fig. 9).
DR. GOTTLIEB Do you routinely include second molars in the strapup?
DR. ZACHRISSON I think you should control the lower second molars in as many cases as possible. The real breakthrough came with bonding, because you could bond small buccal tubes in that triangular region of exposed tooth as soon as the second molars erupt. The best of these attachments bond really well. It gives me much better control of the entire mandibular arch. I also think it has to do with the vertical dimension. If you can get hold of that lower second molar and intrude it or level it with the first molar, the treatment of a Class II is much easier because the second molar is not sticking up and preventing the upper first molar from seating properly. Also you have a better control of the forward growth of the mandible, because the further back you are and the more eruption of those teeth you have, the less you can take advantage of the horizontal component of normal growth. So, yes, I do think that lower second molars should be included in the strapup in almost every case. The only exception would be when the treatment is almost done and the lower second molars are just coming in and seem to be in a nice position. A more interesting problem may be what you do with upper second molars. I am strapping up more and more upper second molars.

Fig. 9 Undertorque of upper and particularly lower incisors in this case is undesirable, and may increase chances for vertical relapse.
DR. GOTTLIEB What labiolingual inclination of molars are you shooting for?
DR. ZACHRISSON The heights of the lingual cusps of the mandibular first and second molars are very important. I want them to be high enough to give me a nearly flat curve of Wilson. This is one of the reasons I use 0° torque on my lower second molar tubes-- if the lower second molars are inclined too much lingually, the upper molars erupt to occlude with them and could create balancing interferences. Another reason is that there is not enough strength in the terminal ends of the archwire to really overtorque them, so you more or less hold them in position. The position of the lingual cusps of the lower first and second molars may be the most important functional factor to look for. If the lower molars are tilted toward the lingual and the upper molars occlude with them, the lingual cusps of the upper molars are hanging down and that's where you get the interferences in the balancing occlusion.
DR. GOTTLIEB Does it make any sense to finish to a particular gnathological scheme? Do you believe in a cuspid protected occlusion?
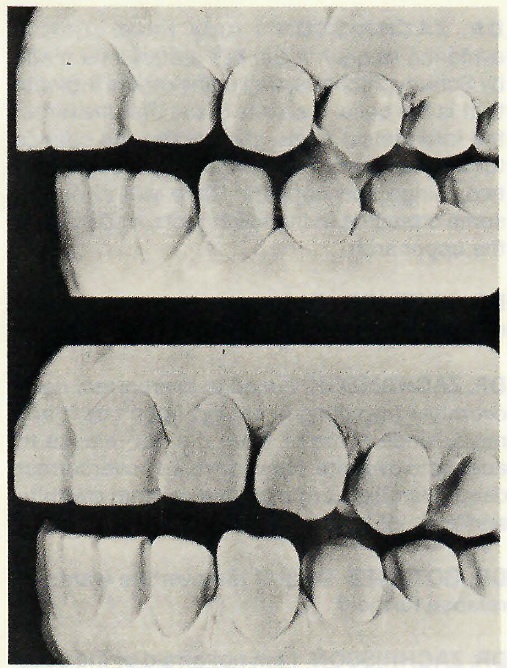
DR. ZACHRISSON Ingervall did a study which showed that group function is seen as often as cuspid protected occlusion. In a study of untreated ideal occlusions from the Los Angeles Smile of the Year contest, at age 12 these patients all had cuspid protected occlusions and no cuspid wear. Ten years later, 25 percent had considerable cuspid wear and a group function type of occlusion (Fig. 10). I feel that a cuspid protected occlusion is probably the preferable one, but that a group function occlusion functions equally well, even long term.
Fig. 10 Cuspid wear after 10 years with change from cuspid protection to group function. (From Hopkins, J.B. and Murphy, J.: Variations in Good Occlusions, Angle Orthod. 41:55·65, 1971.)
DR. GOTTLIEB Does the orthodontist influence cuspid protection to any great extent? Can the orthodontist create cuspid protection if the patient doesn't have it?
DR. ZACHRISSON I think you can create it, and you can take that into consideration when you plan and treat a case. The question is, will it remain there? As in the Smile of the Year sample, 10 years later the cuspid protection may be worn off in a significant percentage of the cases. It is not one of my major concerns in treatment. Several other aspects are more important, but of course I try to finish my cases to the best possible functioning occlusion. In that regard, I am shooting for a cuspid protected occlusion on the working side.
DR. GOTTLIEB Do you check for slide?
DR. ZACHRISSON Yes. I think you should avoid slide, unilateral contacts, and balancing interferences. I like to see the balancing side disocclude in lateral movements and the posterior teeth disocclude in protrusive movements. I like to have bilateral contact in the glide from centric relation to centric occlusion. But that is something I presently believe I can obtain automatically if I keep checking and correcting the axial inclination of the teeth, torque, and height of marginal ridges during treatment. In other words, if I take the patient to a good static occlusion with no dual bite, I think the functional aspects for practical clinical purposes fall into place by themselves. I am careful in checking the buccal torque of molars, the height of the lingual cusps, the height of the marginal ridges, the relative height of the cuspids, and the anterior overbite. That is a biological approach.
DR. GOTTLIEB You do not believe in routinely mounting cases on an articulator?
DR. ZACHRISSON I have not been convinced by studying my own cases that I should start mounting all the cases on articulators and do a more elaborate analysis. I haven't seen the research evidence that convinces me you can do better by doing so. That is not an excuse for sloppy treatment. For example, one of the things I see all the time is marginal height discrepancy between the lower bicuspids and first molars. Most of the time when I place a lower molar band, I have to push the band down to avoid interfering with the bite so the patient does not bite on the buccal tube. I have to compensate for that in my archwire. If I don't, I only raise the molar and may create a functional disturbance in that region. These problems could be analyzed on an articulator, but you should be able to analyze them in the mouth as well.
DR. GOTTLIEB It has been said that traumatic occlusion and malocclusion per se do not cause periodontal problems. But isn't it reasonable to think that might only be true under conditions of perfect hygiene, and that malocclusions do create all kind of food traps and can have a detrimental periodontal effect?
DR. ZACHRISSON I agree. At least when it comes to the relationship of malalignment of the teeth and periodontal destruction, I think we have some very good evidence in the classic study of Ainamo. He divided his sample into subgroups depending on their hygiene. In the group with good hygiene he didn't find any relationship between crowding of the teeth and periodontal breakdown; and there was no difference among those who never brushed their teeth or had very poor hygiene, because that group had periodontal breakdown regardless of crowding. But in the average group he found a clear correlation. The more crowding he had the more loss of attachment, because malalignment of the teeth decreases the effect of average hygiene procedures.
DR. GOTTLIEB The lower anterior teeth are the ones that are most irregular, and yet those are the teeth that have the greatest longevity.
DR. ZACHRISSON They are also the teeth that are most easy to clean. The contact relationships and the possibilities for plaque accumulation are quite different in the anterior region compared to the posterior region, and the tooth anatomy is so different. For instance, there are no bifurcations in the anterior teeth or proximal indentations as you have on bicuspids. But we have to distinguish between moderate and severe irregularity. I have seen several patients with pronounced irregularities in the lower anterior region that were in essence impossible to clean, and I have seen marked periodontal destruction around such teeth. Malalignment of teeth does decrease the effectiveness of average hygiene efforts. But with mild to moderate crowding, I have to agree that it seems possible to maintain such teeth for a lifetime with average hygiene procedures.
DR. GOTTLIEB In a way, it diminishes the importance of straightening them out for health reasons and increases the importance of cosmetics.
DR. ZACHRISSON Certainly the straightness of teeth is an esthetic problem more than anything else. I think people treat their anterior teeth more for esthetic reasons because those are the teeth that are most important to them.
DR. GOTTLIEB How often do you adjust the incisal edges of anterior teeth?
DR. ZACHRISSON I adjust the incisal edges of upper incisors about 95 percent of the time. I mostly modify uppers, but if the lowers are uneven, worn, or chipped, I routinely modify those too (Fig. 11).

Fig. 11 Chip in right ·central incisor and triangular morphology of four upper incisors corrected by grinding and slenderizing before bracket placement.
DR. GOTTLIEB How much of an incisal chip can you consider grinding away instead of adding on?
DR. ZACHRISSON You have to evaluate the morphology of the tooth and relate that to the type of case you are working with. The advantage of grinding away the tip is that you are achieving a permanent result in comparison to a composite build-up, which must be regarded as needing replacement several times later in life. So you have to make a judgment in each case. You have to relate clinical crown height to the total impression you get when you look at the patient from the front.
DR. GOTTLIEB Are there any pulpal considerations?
DR. ZACHRISSON Not with the correct technique. Our studies demonstrate that you can convert cuspids to lateral incisors with no fear of pulpal involvement, as long as you grind them down with adequate water cooling. When we recontour cuspids to lateral incisors and when we do gross recontouring of incisal edges, I like to use an abundant water and air stream. Actually, I place a towel around the patient's neck and have an assistant shoot a constant water and air stream to the teeth while I do the gross recontouring. This has the advantage of making the grinding less painful, too. Anesthesia is never needed. When we do the fine tuning, I just use an air stream so I have greater visibility. For stripping, I do not usually use any type of cooling. But I do use air cooling for the flexible diamond disc on triangular teeth, because I want to see exactly what I am doing.
DR. GOTTLIEB When you reduce the incisal edge of a tooth you then have to reduce the labiolingual thickness, too.
DR. ZACHRISSON Yes, many times that adjustment must be made. When you move a cuspid into the lateral position, you have to take the labiolingual thickness into consideration. You have just two choices. You can reduce on the lingual or position the tooth forward labially.
DR. GOTTLIEB Do you grind incisal tips before treatment and adjust your bracket height accordingly, or do you anticipate your bracket height and make the incisal tip adjustment as the tooth is elongated?
DR. ZACHRISSON It depends on how much of a chip it was (Fig. 11).
DR. GOTTLIEB Do you treat the ground incisal edge for sensitivity?
DR. ZACHRISSON No, you don't have to. Both clinical and in vitro studies have shown that as long as you cool it so you don't get odontoblast aspiration in the tubules and have smooth, self-cleansing surfaces-- then just use normal fluoride from toothpaste or mouthrinse--you don't get increased sensitivity to hot and cold.
DR. GOTTLIEB Under what circumstances do you not modify the incisal edges?
DR. ZACHRISSON In cases where I have inadequate overbite. By doing the recontouring I would reduce the overbite, which I need in those cases. So in those cases, I usually leave them as they are or add composite.
DR. GOTTLIEB Do you ever grind incisal edges to reduce overbite?
DR. ZACHRISSON You could decrease overbite on one incisor if the incisal edges are not even, but I see no indication for grinding down extensively for the reduction of an overbite.
DR. GOTTLIEB If an incisal chip has permitted an incisor to extrude, do you do a gingivectomy?
DR. ZACHRISSON You could, but the disadvantage of that would be that the root is narrower mesiodistally and the contours of the two central incisors would not match as well. One would be normal and the other would have a triangular shape. It would not look as good as with the Kokich technique, which intrudes the tooth to bring the gingival contours even and then adds composite to the incisal tip (Fig. 12).
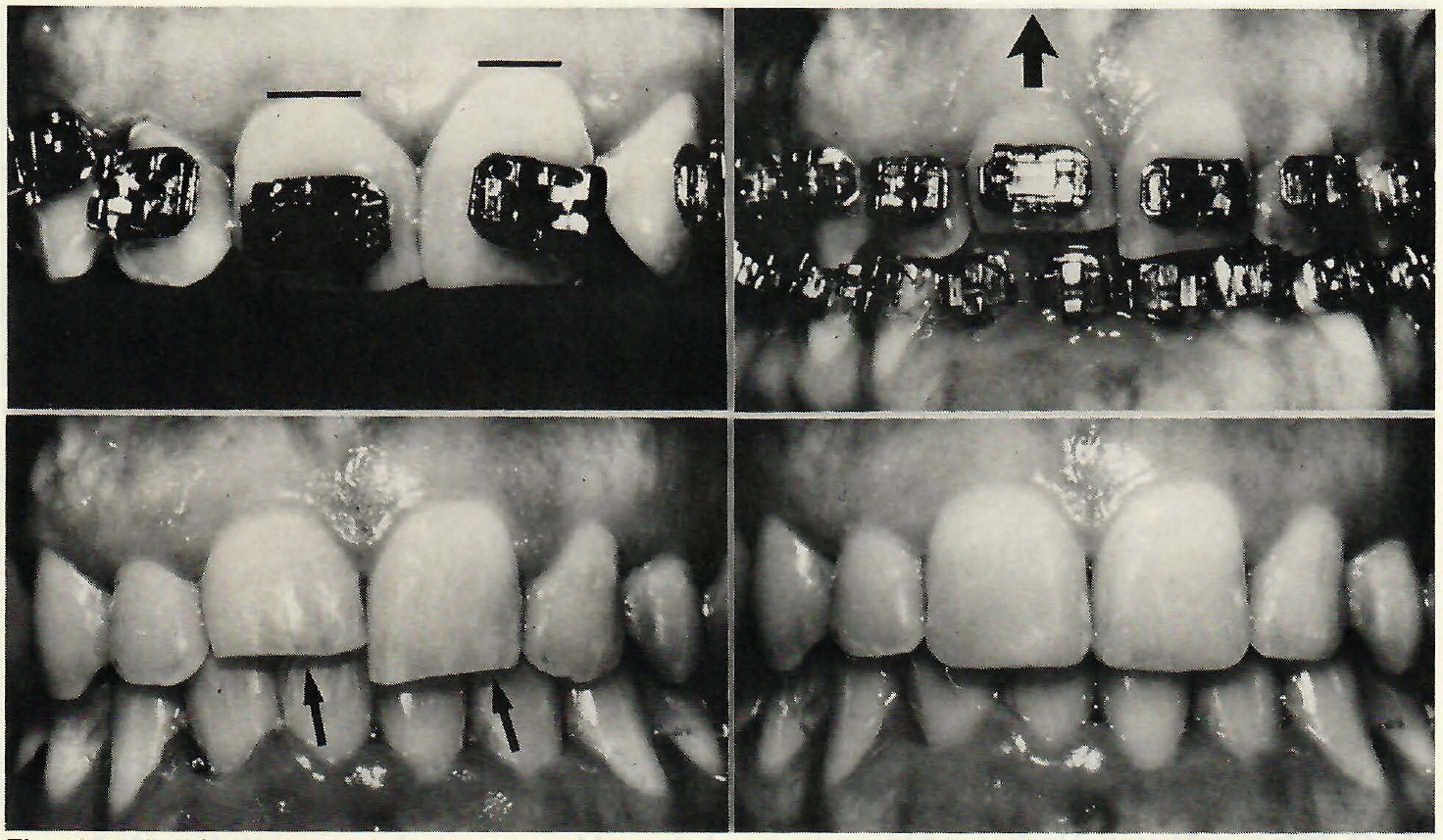
Fig.12 Incisal fracture of right central incisor resulting in different levels of marginal gingivae on upper centrals. Case was treated by intrusion (large arrow) and composite build·up (small arrows) to produce matching gingival levels. (Courtesy of Dr. Vincent Kokich)
DR. GOTTLIEB Would it tend to re-extrude?
DR. ZACHRISSON No, because we are just restoring the morphology of the tooth. These are teeth with traumatic injuries, chips, or wear of one incisor. This procedure just puts the tooth back where it should be. It has extruded. You just reposition it, and I see no reason why it should re-extrude.
DR. GOTTLIEB If you extrude a tooth orthodontically, do you expect some relapse?
DR. ZACHRISSON Yes. I think that tooth movement in the vertical plane has the same degree of relapse tendency as any other type of tooth movement. If I am forcing the eruption of one incisor, I like to overdo it by a half a millimeter to a millimeter to allow for some relapse.
DR. GOTTLIEB Do you believe orthodontists should do composite add-ons or should that be referred out?
DR. ZACHRISSON They should be referred to a general dentist (Fig. 13). The optimal situation is to work with a good GP to whom you can refer. In working with different GPs, you are going to have a variety of quality. It is so rewarding to have high-quality work, it is difficult to accept a lower standard. On the other hand, you have to deal with the family dentists. To me it has been an ideal solution to have one dentist come into the office about one day a month to do them for us, so we can discuss in detail how they should be done.
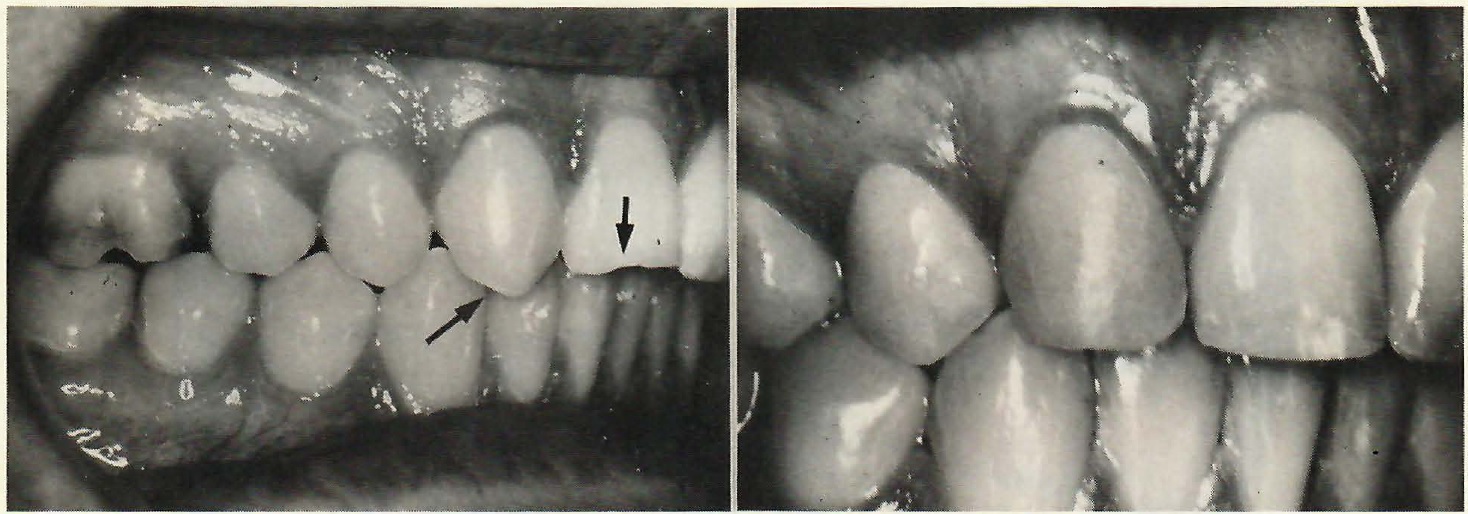
Fig.13 Grinding of right cuspid and composite add-on to cuspid and central incisor in case with missing lateral incisor.
DR. GOTTLIEB Do you have a preferred material for composite build-ups?
DR. ZACHRISSON We use Durafil, but the new light-polymerized composites are all very similar. Of course, you must take precautions to protect the eyes, if you do a significant number of restorations.
DR. GOTTLIEB How much equilibration do you do for functional purposes?
DR. ZACHRISSON I do it to a limited degree. Again you have to distinguish between adolescent and adult treatment. I look upon it differently in an adult, periodontally involved case in which I want to avoid traumatic occlusion. In those cases I am more likely to grind the traumatic interferences than I am in a child with an intact periodontium. There I equilibrate for an obvious interference, but I do not go through a very careful analysis. Another case where I would do it is in the case of a missing upper lateral or central incisor in which I moved the entire posterior dentition forward so that the first bicuspid is in the cuspid position (Fig. 14). As you rotate the bicuspids, the lingual cusps may be a source of interference, and I check for that. If there is an interference, I reduce the lingual cusp at the end of treatment when I analyze the occlusion.
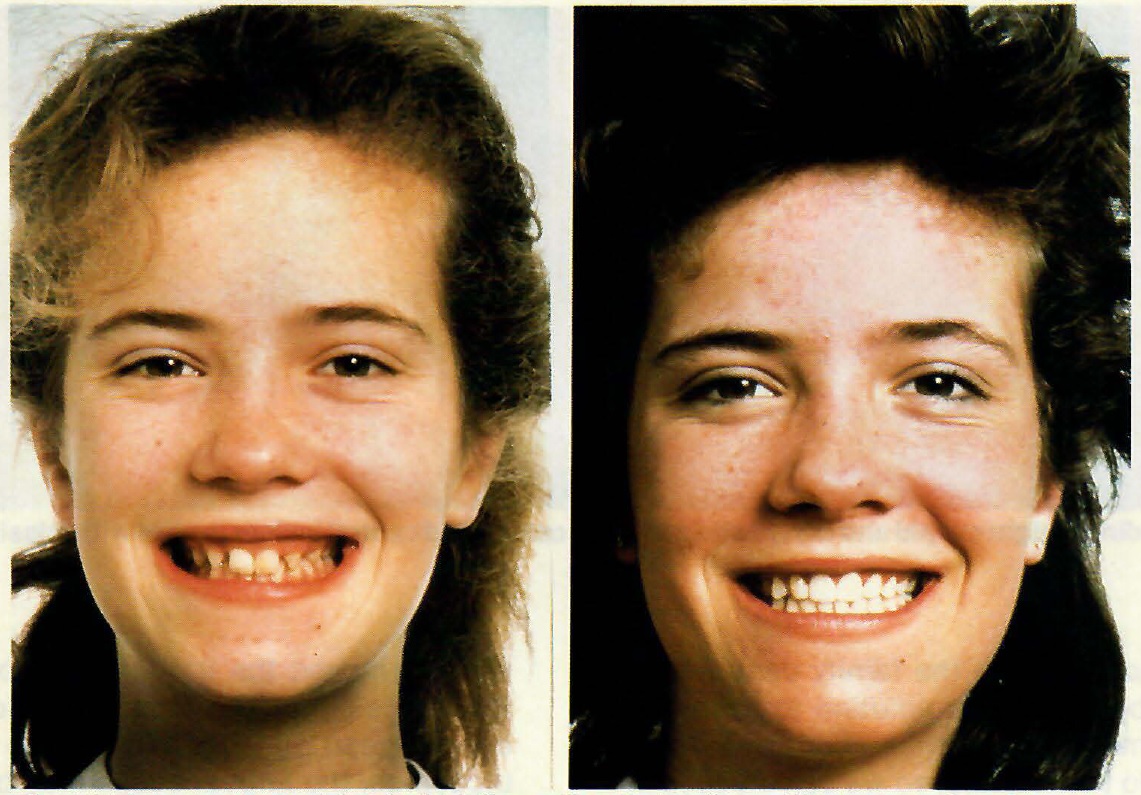
Fig.14 Fourteen-year-old girl with bilaterally missing lateral incisors, pointed cuspids, and gummy smile before and after treatment. Both cuspids were ground and received mesial composite build-ups. Gingivectomy was performed over the four anterior maxillary teeth.
DR. GOTTLIEB Do you wait a certain amount of time to see what trauma you have before you do equilibration on a tooth?
DR ZACHRISSON When and how to equilibrate are complicated questions. So far, I do not feel we have adequate documentation or scientific evidence to back up the different clinical recommendations of which we learn at present. Studies in electromyography by Harold Perry (1961) have shown that the more severe malocclusions have greater asynchronous harmony of masseter and temporal muscles, and even after orthodontic treatment, these cases still do not have synchronous muscle activity. Jim Jensen has been following cases that have been mounted on a SAM articulator and then carefully equilibrated, and he found that a year or two later these patients do not have a perfectly balanced occlusion any more. They were again equilibrated and it was found that the occlusion on these cases again changed, and these changes may be associated with asynchronous muscle activity. The only thing that really scares me is a vertical bone defect in the periodontally involved dentition, because in some instances I have seen that severe traumatic occlusion, superimposed on a patient who has an advanced periodontitis, has created marked bone loss that I was very unhappy to see. I make very certain today that a patient with vertical bone defects is sent to a periodontist and the inflammation is controlled. Some periodontists claim that all you have to do in those cases is to control the inflammation, and the teeth will settle and the traumatic occlusion will be eliminated, so that grinding should really not be needed. However, I do not like to take any chances, and I would keep the tooth out of function or traumatic occlusion one way or another--with a splint, with grinding, or with whatever means there may be.
DR. GOTTLIEB How much changing of tooth morphology do you do before treatment?
DR. ZACHRISSON Over the years, my thinking has changed. Today I am more likely to make changes at the start of treatment (Fig. 11). If I have incisal edges that are worn, chipped, or abnormal, I like to recontour them because it makes bracket placement easier and better. If I have triangular-shaped teeth with nice gingival contours at the start of treatment, I inform the patient that these teeth are triangular, and because they are crowded or overlapping the gingiva is now filling in the space-- but as we resolve the crowding we are going to have problems with triangular spaces between the teeth, which can be corrected (Fig. 15).
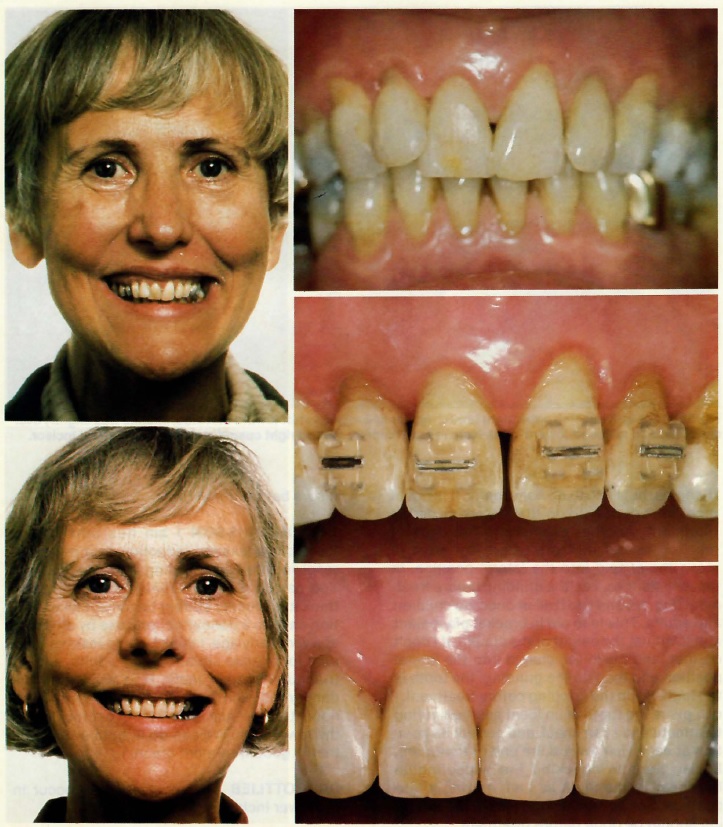
Fig. 15 Crowding promotes good gingival fill-in before treatment in 54-year-old woman with malaligned, triangular upper incisors. Slenderizing was necessary after space opening to avoid interdental gingival recession. Incisal edges were recontoured.
This can be done later in treatment after the patient realizes that there are triangles, but I like to do some early. It is not of great importance if I do that before or during treatment. Another example is the case of missing lateral incisors where we want to move the cuspid into the lateral position. In those instances, I do the grinding before treatment (Fig. 16) and I do it all at once, on children and adults. This is to aid in bracket placement and to adjust the height of the cuspid. If I don't do that, and move the cuspid into the lateral position and then do the grinding, the tooth is too high. If I do the grinding before treatment, I can place the tooth in an ideal position during treatment and I can check and correct its position at each visit toward the end of treatment. It also permits checking the buccolingual thickness of the tooth as I am moving it into position. So I believe a good part of recontouring should be done before treatment.
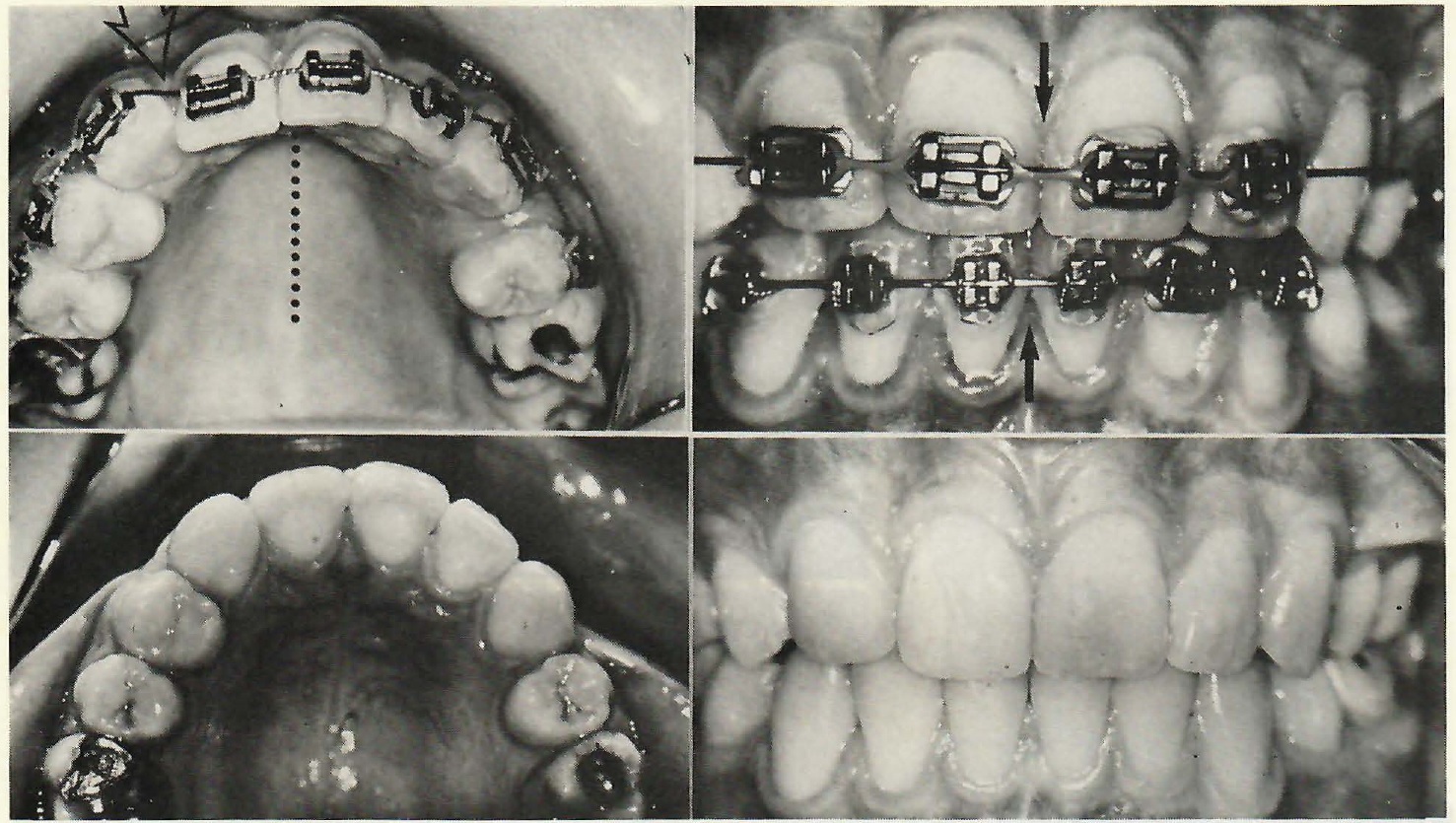
Fig. 16 Case with missing upper right lateral incisor and midline shift toward that side. Midline was slightly over-corrected and relapsed toward ideal. Note resemblance of ground right cuspid and intact left lateral incisor.
DR. GOTTLIEB Do you strip crowded lower incisors before treatment?
DR. ZACHRISSON I am hesitant to use mesiodistal enamel reduction as a means of resolving marked crowding in a young patient. You can do it in borderline cases, but I don't think it is entirely correct to convert an extraction case to a nonextraction case by stripping at a very early age. I think I would reserve stripping for relapse situations, for adults, and for triangular-shaped teeth. It is a little on the dangerous side to treat almost every case nonextraction and strip 2-3mm of crowding in the lower arch. We can do it, but I don't think that is good treatment planning.
DR. GOTTLIEB Does most relapse occur in the lower incisor region?
DR. ZACHRISSON Yes, and because of that I like to use techniques like placing the four incisors outside the cuspids, broadening the contact points slightly, recontouring if necessary, and placing a bonded 3-3 retainer for a couple of years. Placing all four incisors outside the cuspids can mask or avoid a good deal of that crowding. In particular, late lower crowding with lateral incisors to the lingual of the cuspids may be more noticeable from the front.
DR. GOTTLIEB If you grind the labial corner of one tooth and the lingual corner of the next one to mask an irregularity, it may look good at the moment you do it but what is the prognosis for that procedure?
DR. ZACHRISSON I was talking about recontouring the incisal edges. That creates a flat plane that the patients like to see. The procedure you are referring to has to be evaluated by the amount of the original crowding, the age of the patient, and the length of time after treatment. You might have a hunch whether it will remain stable or become worse. If you suspect it will become worse, you must be careful about the technique you mentioned.
DR. GOTTLIEB Such crowding can result from the reciprocal effect of the upper and lower incisors on each other.
DR. ZACHRISSON Duterloo has shown in longitudinal growth studies that abnormal morphology of the lingual surface of the upper incisors may reflect itself in a corresponding malalignment of the lower incisors. You can't treat those patients successfully unless you do something about both arches. You have to treat the root of the problem and not just the symptom. This might mean that in the future I will have to be more concerned with recontouring the lingual surfaces of some maxillary incisors.
DR. GOTTLIEB Sometimes the crowding problem may be solved by the extraction of one lower anterior. Does this cause bite closure?
DR. ZACHRISSON My experience over the years is that it definitely does. In selected instances I have extracted one lower incisor purposely in Class III open bite tendency cases. As far as I can judge, what happens then is that the lower anterior teeth move inward and upward, and do exactly what I like to see in a Class III open bite tendency case. I have also taken out lower incisors in the opposite situation-- in Class II deep bite cases-- with results that I have not liked.
DR. GOTTLIEB When you see one missing lateral, what are your considerations about opening or closing the space?
DR. ZACHRISSON These are usually difficult problems, and it is hard to obtain excellent results with whatever solution you choose. In a situation like that, you must first consider the spacing and crowding conditions in the arch. I would also take a look at the color of the cuspids-- not so much their shape, because today by grinding and composite add-on we can change the cuspid to almost any shape we want (Fig. 13)-- but it is hard to do much with a cuspid that is too yellow. On the other hand, I think that if the alternative is to open up space and put in bridgework, in the majority of cases my preference would be to close the space and avoid that-- even if we might need a bonded retainer for a long period of time on the lingual. I am not afraid of treating missing laterals unilaterally. It is difficult treatment, but it can be done, the midlines can be held, and the result can be satisfactory (Fig. 16).
DR. GOTTLIEB What are limiting factors to closing the space?
DR. ZACHRISSON Generalized spacing and the size of the crown on the remaining lateral on the other side. If it is small, the patient would not look symmetrical. If you have had a peg-shaped lateral on the other side, particularly if there was a good deal of crowding in the arch, I would extract the peg-shaped tooth.
DR. GOTTLIEB Peg-shaped laterals are a problem all by themselves. What are your considerations in preserving them or extracting them?
DR. ZACHRISSON You have to consider the size of the root and the size of the crown. You can overbuild a peg-shaped lateral that has a narrow crown, and that creates another problem. A small peg-shaped lateral limits what you can do with a composite build-up in the mesiodistal dimension at the gingival margin. You can't put too much composite on those teeth or you may end up with composite buildups that are not very esthetic and may be caries prone. There are great variations among peg-shaped laterals, and it is hard to make generalizations about them.
DR. GOTTLIEB If there is a missing lateral and you move the cuspid over to take the place of the lateral, you are moving a first bicuspid to take the place of the cuspid. What are the considerations about that?
DR. ZACHRISSON I see no contraindications to that movement. There is no evidence that it is undesirable from a functional point of view. On the contrary, I think it can be done nicely if a number of factors are taken into consideration-- like moving the cuspid to the lateral position and reshaping it nicely, rotating the bicuspid properly so that it looks good, and reducing the lingual cusp of the bicuspid if there is a balancing interference with that cusp. You secure a modified group function occlusion, and I think you have found a solution that works efficiently and is esthetically acceptable. In fact, Nordquist and McNeill showed that patients whose lateral incisor spaces had been closed were healthier periodontally 10 years after treatment than patients with prosthetic lateral incisors, and that the presence or absence of cuspid protection was not related to periodontal status. There was no evidence to support a preference for the establishment of a Class I cuspid relationship for patients with missing upper lateral incisors.
DR. GOTTLIEB Are you satisfied with the Class II posterior occlusion in those cases?
DR. ZACHRISSON I am more concerned about having a good occlusion on the bicuspids and cuspids than I am about the exact positioning of the molar occlusion. I find that if I have a good interlocking occlusion in the bicuspid and cuspid area, there seems to be no reason why themolar occlusion should be a negative influence. There is no indication as far as I know that a Class II molar occlusion should be of any significance or damage to the dentition, except possibly if you have only extracted in the upper arch and teh lower ach may be mildly crowded to start with. By restricting the arch length in the upper arch you might transmit that restriction to the lower arch, and in the long run the lower arch might be more crowded.