JCO Interviews Robert J. Schulhof on Practice Management
JCO Bob, as President of Millenium Society, you have been heavily involved in orthodontic practice management. What do you see as the most significant single challenge orthodontists face today?
ROBERT J. SCHULHOF Survival. In the face of a declining economy, changing demographics and third parties who would very much like to control the marketplace, my first impression is to say survival. More than that, though, I think it is maintenance of those values for which the orthodontist became a specialist--a good standard of living, the satisfaction of a job well done, the independence of making your own decisions and being in control of your own fate.
JCO Do you have some solutions for orthodontists, to improve their chances for survival?
RJS There are solutions which have proven successful in individual cases, but they are not easy. According to Carl Gugino, who has taught me a lot about orthodontic management, success will require about three times the expertise needed in the past. Whereas the successful orthodontist of the 60's had to master only one "M", mechanics, the successful orthodontist of the 80's will have to master 3 "M"s: mechanics, management, and marketing.
JCO What do you mean by management?
RJS Management is the branch of human behavioral science which deals with getting others to accomplish work on your behalf. In orthodontics, this means getting your staff to work with you and for you, and having the patient cooperate in his treatment. All management really requires four steps: Planning, Organizing, Leading, and Controlling. Whenever you are performing any of these four, you are managing.
JCO Can you give examples? Let's start with planning?
RJS First of all, I think that periodically an orthodontist should sit back and take stock of things, decide what he would like to see happen. Set some objectives. How much would he like to make next year? Will this involve raising fees, cutting costs, increasing starts? How many cases would he like to start? What would he need to do to attract them? Will he need more staff and facilities in the future?
JCO You don't see many orthodontists doing any of that?
RJS Well, usually no time is specifically set aside for planning, and information on which to base plans is usually lacking, such as sources of referrals, number of exams, consultations, and starts each year, fees and costs. Very little attention is given to the overall condition of the practice until the bank balance gets too low.
JCO What about organizing?
RJS Most practices organize people. At the beginning, they have one "Mary Marvelous" who does everything. The second person hired then gets the jobs that Mary doesn't like to do, and the third and fourth must fit themselves into a jigsaw puzzle that is built around existing personalities. The systems and procedures in use are rarely written down and are really only in the minds of the key people--not a belonging of the practice. The work should first be organized into distinct areas of responsibility--almost territories--where people are encouraged to feel ownership of their area and are free to make as many of their own decisions as possible. Each person should have one and only one superior to answer to, and responsibilities should not be shared. If two people are responsible, then nobody is at fault when things go wrong, and nobody can see the fruits of their effort when things go right. It takes a lot of work to properly organize a practice and to adequately document the organization with position charters, job descriptions, policies and procedures. Most people really do not have a clear understanding of their job, and when they think they do, it is often different than what the doctor thinks it is. Of course there is the day-to-day organization such as scheduling and patient flow which are critical to practice operations.
[show_img]760-JCO-img-0.jpg[/show_img]
An important aspect of organization
is the written job description.
RJS Yes. After you have decided what is to be done, and organized the work so that people can efficiently accomplish it, they must be trained and motivated to do the work. Leading is really the most time-consuming of all. I hear over and over that people just aren't reliable: that turnover is too high. Most professionals see personnel matters only from the point of view of the judge--choose the right people, get rid of the ones who don't produce. A professional manager sees his role as a developer of people through counseling, coaching, performance feedback, and career planning. This kind of motivating can't take place at the chair in the form of side remarks, or at lunch, but requires special time set aside for one-to-one sessions. Real scheduled time shows you sincerely feel the employee is important.
JCO And controlling?
RJS If we did the first three steps, planning, organizing, and leading, perfectly, we would never have to add controlling. But that isn't the case. One of our greatest failings is having elaborate plans and then putting them away, never to see them again. The dates and schedules for our plans should become our controls. These can be reviewed at staff meetings and performance reviews to close the loop. It is a real letdown to people to get them all motivated about some objective and then just letting the subject fade away as we so often do:
JCO These seem like pretty natural ideas, but they are not widely applied in orthodontics. What is standing in the way?
RJS Certainly some professionals tell me that they wouldn't really know what to do with management time if they had it--that they need to learn the basic skills. But more often, far more is known than is actually applied. Most proprietors--and this goes for engineers, shopkeepers, lawyers, as well as doctors--are not willing to commit money to the long term results of management. There are always things that seem, in the short run, to be more important--like putting out the brush-fires that good management could have avoided in the first place.
JCO Can an unmanaged practice really be turned around?
RJS Yes, that is the really good news. The practices that have made the commitment to apply management techniques are bucking the negative trends. In our recent economic survey of Millenium practices, 80% said that they were up and 60% said that they were ahead of schedule. More than that, however, we get reports of much more career satisfaction from both the doctor and the staff. It's just much nicer to be in an environment where frustration is next to a minimum.
JCO Now what about delegation of duties. Many feel that the personal attention of the orthodontist in communication and treatment are the keys to practice success. Can these be delegated?
RJS In our experience, the key to practice success is to understand that the patient perceives the service rendered in an orthodontic practice totally differently than the orthodontist. The orthodontist sees his job as providing a particular occlusal scheme, which the patient had a need for at the first appointment and which the doctor will provide at retention. However, at each appointment, the patient has needs. He thinks, "How long am I going to wait today? Will it take forty minutes again to get five of work done? Will it hurt? Does this wire jabbing my cheek mean anything? Was this month worth it? Did I make any real progress toward getting these horrible things off?"
JCO You mean he has a need for communication above all?
RJS Precisely. And those practices who gear up to fill this communication need in a professional way, who show they really care are the most successful. They are busier, and can demand the best fees because they satisfy the real patient needs. Even in a small practice, the orthodontist is usually too preoccupied to be available to all the patients and parents, especially the ones in the waiting room or on the telephone.
JCO Should delegation of technical tasks free the orthodontist for communication, or should communication also be delegated?
RJS For consistency and availability, communication is best delegated and if the communication is handled well, who actually places the wires is secondary.
JCO How about the orthodontist who is skilled at treatment, but not management? Should he have an office manager?
RJS When an orthodontist goes into private practice--takes out his loan and opens his office, he is saying: "I wish to be master of my own destiny, not be someone else's employee. I am willing to take the risk for a sufficient reward which includes independence." He is really making a commitment to manage his own affairs. Now, today there for those who wish to exercise their technical skills only--they are the Tier I and Tier II organizations referred to by Avrom King--the clinics HMO'S and other large groups. These are organizations which professionally manage the professionals and many doctors will be happier in such a protected environment. The office manager is a throwback to the days when creative guidance of the organization wasn't necessary, and so the undesireable tasks of collecting money, paying bills, and listening to staff complaints were delegated to the office manager who probably began as a receptionist. The doctor who operates in this manner and takes no real interest in management will in the future be beaten by both the professional manager of Tiers I and II and the true managing professional of Tier III.
JCO Speaking of the big clinics versus the individual practitioners, many orthodontists feel pressure to compete on the basis of fee. How do you feel about the effectiveness of marketing on the basis of fee hoping to make a greater profit on the greater volume?
RJS The legend of Henry Ford makes us believe that greater volume will result in lower unit cost. This is definitely true in automobiles, but not in orthodontics. The more cases you start, the less the doctor can do himself, the more he delegates, the more people he hires, the greater the management needs, and so on. Quite often, overhead percent goes up as practice size increases. The unit costs for our largest practices are remarkably close to those of our smaller practices--about $1100 per case--given the same quality of service. Now an average fee is about $2100 and to make a serious dent in the demand curve, you would have to cut to about $1800. But, at $1100 cost, you can net $1000 at $2100 versus only $700 at $1800. Thus, if you are starting 100 cases per year at $2100, and cut your fees to $1800, you would have to get 143 cases just to break even. That's 43% morework for the same take home. You are much better off trying to find some way of starting 143 $2100 cases.
JCO Is it necessary to have a big practice?
RJS The secret is not so much sheer size as offering a superior service, charging accordingly, and collecting what is owed. The single practitioner, working 4 days per week or 160 days per year, can comfortably start about 325 full cases, preferably in one office. In states where the doctor is restricted in his delegation, you would have to cut that start figure significantly down to 150-200.
JCO You said "preferably in one office" Are you against satellite offices?
RJS From a standpoint of cost and complication, I would much rather see 200 patient starts in one office than 100 in each of two offices. I would make sure that my systems were well worked out and that the growth in the main office had plateaued before going into a second office. Two poorly managed offices can be just twice as many headaches.
JCO How about group practice?
RJS The main value of adding an associate is to take the pressure off, to allow time off, or in anticipation of retirement. Just two doctors can be a problem in terms of dividing the duties equitably. Our favorite setup is the 3-doctor practice, with each doctor's age differing from the next
[show_img]760-JCO-img-1.jpg[/show_img]
[show_img]760-JCO-img-2.jpg[/show_img]
[show_img]760-JCO-img-3.jpg[/show_img]
The management structure to accomplish the work in a small practice.
JCO How so?
RJS Suppose you have a typical 100 start per year practice, squeezing out every dime, and posting a 45% overhead, even with a competitive $1800 fee. The doctor is making $99,000 a year, which doesn't go as far as it used to, and the practice is threatened by a new orthodontist on the block. If he came to us for help, we would probably tell him to hire additional staff to improve his communication, patient flow, and collections; and try some marketing programs. This might cause a jump to 60% overhead temporarily, but if it allows him to raise his fees 10% in real terms and increase his starts 20% (a reasonable Millenium objective in the second or third year), it's well worth it. As the following example shows, even at a 50% overhead level:
Old gross: 100 starts X $1,800= $180,000
Old net: .55 X $180,000 = $99,000
New gross: 120 starts X $1,980= $237,600
New net: .50 X $237,600 = $118,800
In addition, he now has a superior delivery system capable of continued growth. You shouldn't be afraid to spend money.
JCO What constitutes a good management system in orthodontic practice?
RJS We have five key principles that are tough to swallow, if you are not prepared for them: management time, the concept of supervisors, delegation of consultation, our scheduling system, and the total systems approach.JCO How do you define management time?
RJS If management is really an important job, real time needs to be set aside for it--not after hours and not at lunch. You need time to talk to your subordinates, to counsel, to coach and to motivate. Your supervisors need time with each other to coordinate activities, and with their subordinates in review sessions. These communication meetings really mean the difference between a smooth functioning unit with people who are working well together, and the more usual stressful relationship characterized by high turnover, low morale and problems that never get solved. Doctors are reluctant to put away this time at first or even to find it in their helter skelter schedule But, once they do, they are very thankful that they did.
JCO How much time do you feel should be allotted for management functions?
RJS While it is always risky to generalize, we like to see a half-day of pure management time set aside for each three days at the chair.
JCO You mentioned supervisors. Does a small practice really have room for supervisors?
RJS Let's take our optimized practice of 150 starts. The practice is open 3½ days per week and there are 7 people on the staff, most of whom work part-time:Clinical Supervisor (5 days)Chairside 1 (3 days)Chairside 2 (3 days)Chairside 3 (2½ days)Records Technician (2½ days)Comm/Fin Supervisor (5 days)Receptionist (4 days)
JCO Let's begin in the clinical area.
RJS It needs someone competent to control flow and routing of the doctor to the appropriate chair,train new staff members and order supplies. In addition, the assistants needs to have someone to hear their grievances, to counsel and coach them. The doctor rarely has the patience or time for this, so it goes undone. Someone should have this responsibility. We call her the Clinical Supervisor. Now for the front office. I am sure you will agree that communication is the weakest link in many practices. For us, communication is not only the first step on the road to cooperation, but the cornerstone of marketing. We feel that someone should be readily available to the patient and parents at all times and, because of other assignments, that person cannot be either the doctor or the receptionist.
JCO You are recommending a separate PR person?
RJS Yes. There are many opportunities to build PR in communications from the initial phone call to exam to the consultation, progress reviews, and retention conference, all of which are important enough to have preplanned, documented procedures and someone qualified and responsible to carry them out. That person we call the Communication Supervisor. It is an important part of delivering the superior service. In addition, the finances of the practice are worthy of attention. Many Millenium practices have recovered the total cost by just giving collections and budgeting their proper due with a good system. In some practices, financial is a part-time person; in others it is handled by the communication supervisor. In the large practice, it is a full-time job. The receptionist, secretary, or clerical staff would also report to the communications supervisor. This means the doctor only has to coordinate through two people--much easier on him, and they do it better in the long run.
JCO You showed only two employees--the Clinical Supervisor and the Communications Supervisor--working 5 days a week. The rest of the employees are part-timers?
RJS Well, it usually means having a part-time receptionist and part-time chairside assistants, as the supervisors fulfilled these duties before.
JCO How do you select the supervisors?
RJS Making the selection of the clinical supervisor may be difficult. If there haven't been supervisors before, there is often ill-feeling from those not selected. It would be nice if the person with the greatest seniority was the most respected for technical knowledge and the best at working with people. If I were to compromise, the technical skill is probably the least important. She won't really be working in the mouth.
JCO You can't do that overnight. The person elevated to supervisor needs training.
RJS Sometimes, it may be appropriate to phase someone into the job--first as a coordinator, then add the training. The full duties of a supervisor include hiring, firing and raises. Some practices have avoided the problem because the doctor does a good job of communicating. But, there are benefits to everyone in having a supervisor who can provide a smoother, less stressful environment to staff and doctor. Other practices have had to experience the loss of recalcitrant staff members.
JCO That can be traumatic.
RJS While our systems are designed to avoid the loss of good staff members, occasional turnover is unavoidable and with good training and procedure manuals should not be traumatic.
JCO Do you believe that the Communications Supervisor should give most of the consultation?
RJS Definitely. Although Frank Edwards has expounded on this at length, there are still some doubters. Even if the doctor had so much free time that he could take the full time needed without
ruining his schedule, I think that a trained communications specialist can provide a better presentation to lay people in their terms. Also they can be more complimentary of you than you can of yourself. A final benefit is that the consultation thus establishes the credibility of a person other than the doctor who will always be available to them. This principle has really worked.
JCO What is special about your patient scheduling?
RJS We don't schedule patients. We schedule doctor time, staff members and resources, the patient is added last.
[show_img]760-JCO-img-4.jpg[/show_img] [show_img]760-JCO-img-5.jpg[/show_img]on data from real appointment. Note that significiant portion of an appointment may be wait time, which is wasteful.
[show_img]760-JCO-img-6.jpg[/show_img] [show_img]760-JCO-img-7.jpg[/show_img]
The basis for effective practice management is valid for decision making.
JCO How does that differ from conventional systems?
RJS There are two systems in wide use today. The first is filling up the appointment book with one, two, or three unit appointments wherever they will fit. This we call random chaos because you may at random require the doctor to be in three places simultaneously. The other is "like things at like times"--which I call organized chaos, since you guarantee that you will require the doctor to be in three places at once. The result of most such scheduling systems is that either the patient is kept waiting or that the doctor has nothing to do. Usually, both occur at different times in the same day. Also, once you get behind, you tend not to carry out the planned treatment. The Millenium system pre-plans how many of each type of appointments will be required for a typical day, what they look like in terms of needed doctor and staff time, and how they can best be arranged to avoid conflict. Once this system works, the patients go in and out, the parents are happier, and the doctor eventually finds that he can cut out some practice days with refinement of his scheduling system. Its a second key for superior service. But, you have to have data on which to base your plans. Initially, this takes time and effort; and if the staff doesn't understand the benefits, it can be a stumbling block.
JCO And what was your last key management principle?
RJS The total systems approach. Most doctors' systems are a hodgepodge of handy hints they picked up from here and there, which were never intended to work together, but which they may feel very possessive about. They tend to pick and choose from Millenium systems and their systems in hopes of retaining some "personality" In the long run, they end up using all the Millenium systems, since even if they don't seem better on an Individual basis they really work well together.
JCO Do you have any new concepts?
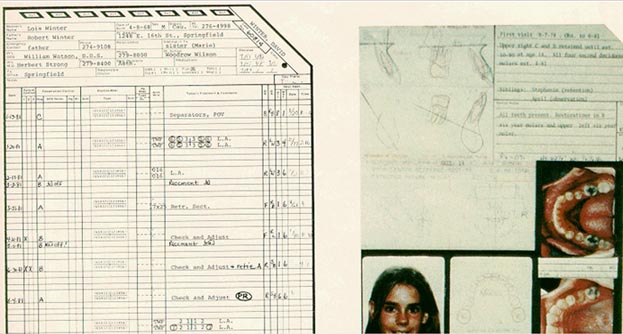
RJS Yes. Our training systems, the ortholetter system, and the financial system usually get accepted without resistance. The recall system is also very cute and really beats anything going. We have had some practices that had a computer, stop using it for recall since our manual system gave thembetter controls. Probably the biggest development in use over the last two years has been our treatment card originated by Dr. Gugino. The concept is a complete visual communication system right at hand to minimize the decision time at each appointment. One side gives all the patient information visually, including photos of models, facial photographs, tracings, and treatment objectives. With one glance at this page, the doctor knows whom he is looking at and where he is going. The treatment steps are pre-programmed so that at each appointment he can judge the patient's progress. The final page is a progress reporting system--another key to superior service.
JCO How do you manage to get the ceph tracing and everything else on one side?
RJS The tracing is miniaturized.
JCO Do you do the miniature tracings, treatment objectives and the treatment sequences with the Rocky Mountain Data Systems computer.
RJS It is not absolutely necessary, but it works best and saves time. The total result is worth it, since it boosts efficiency. Another recent development is our marketing program.
Treatment Chart showing complete patient information and the ultimate practice control/preprogrammed
treatment section.
JCO How do you feel about marketing for the professional? Particularly the place of advertising?
RJS Again, I would refer you to the Edwards article since this subject deserves a complete discussion. The AAO advertisements are tasteful and effective. We still believe that at this stage, advertising by a specialist would lose more business than it would gain, and it doesn't coincide with the first-rate quality image our practices have been so successful in projecting. For now, we believe that a superior service backed by superior communication is a prerequisite to successful marketing. In addition, we have a slide program with quality "capabilities brochures" The key is to make the brochure so nice that it won't be thrown away, but will be handed on. Most practices could not afford this on their own. The joint Millenium effort has been very cost effective.
JCO What do you see in the future for the private practice of orthodontics?
RJS Dentists have been rightfully against "dental insurance" programs as being not really insurance, but merely prepayment with an added administrative cost. Our system of taxation however grossly distorts the economy toward tax-deductible services. Any method of making orthodontics tax-deductible will give it a considerable advantage over its other competitors: cars, vacations and the like. For this reason, many futurists predicted the demise of private practice as large groups sell contracts to unions and companies, or company-owned clinics proliferate.
Much to their credit, the AAO is doing a fine job selling the unions on policies with freedom of choice, and most dentists are taking an admirable hard line on the fact that payment is still the patient's responsibility and that the practice does not deal directly with the insurance company. As long as these trends continue, things look excellent for the private practitioner.