While the use of hypnosis in dental treatment has a long established and well-documented history, there is little or no mention of its application in orthodontics. This is probably due to the fact that orthodontists are not usually involved in dental procedures that call for frequent use of hypnosis, viz. analgesia, pain control, etc. However, hypnosis has several other applications in clinical practice that are often overlooked, and some of these have very definite applications in orthodontics.
This report deals with an orthodontic case that was treated with the help of hypnosis.
Case Report
C.K., a 21-year-old female, had a Class I malocclusion with Class III tendencies, a steep mandibular plane angle, missing mandibular left first molar, maxillary lateral incisors in crossbite and maxillary second molars in buccal crossbite. There was a severe midline discrepancy and the case was by no means an easy one.
There was generalized hypocalcification and several of the anterior teeth bore stains. The patient was due to undergo bleaching subsequent to her orthodontic treatment and it was felt that bonded appliances were contraindicated. When banding was started, however, we encountered a severe problem. The patient was unable to tolerate almost any pressure on her teeth, and the first few sessions for banding and placement of initial archwires proved to be excruciatingly painful. C.K. proved to be an extremely cooperative patient and followed all instructions given to her. So eager was she to receive treatment that she kept struggling through each appointment. There is absolutely no doubt that she was not "shamming" and that the pain and discomfort she felt, which lasted for several days after each appointment, were very real. Things soon became impossible, however, and the placement of a ligature tie would often bring tears to her eyes.
It was felt that it would be impractical, as well as undesirable, to use some form of analgesia or anesthesia for each archwire adjustment. Unless some form of pain control was instituted, it was obvious that treatment may have had to be terminated. The possibility of using hypnosis was suggested, and the patient readily agreed to try it. She proved to be a good subject.
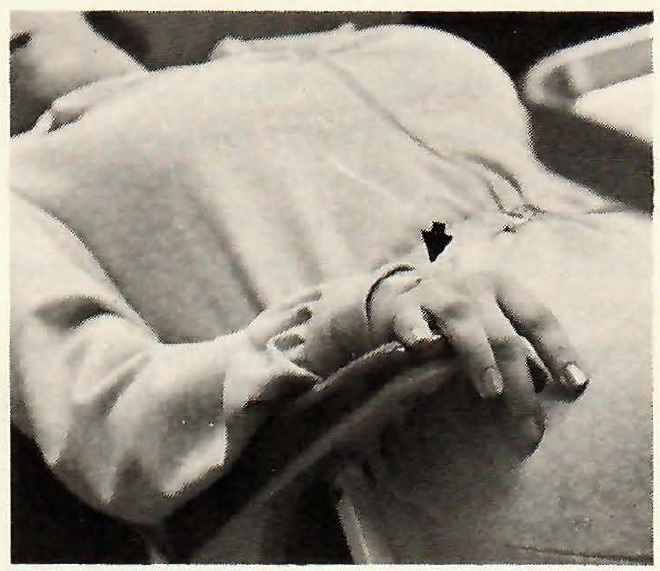
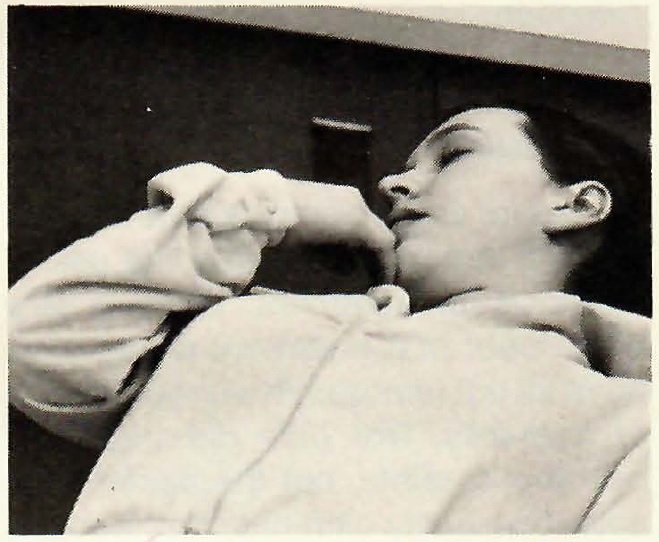
A hypnotic trance was induced and the depth of the trance enhanced through the use of visual imagery (Fig. 1). When the patient was judged to have achieved adequate depth of trance, she was asked to let her right hand "become numb" and to give a signal when this "numbness" was achieved. Her ability to achieve this numbness was tested by inserting a sterile needle into the back of her right hand (Fig. 2). The patient was then asked to place her "numb" right hand in the region of her jaws and to transfer this numbness to her jaws, teeth, and the surrounding soft tissues (Fig. 3). The entire session took approximately 30 minutes.
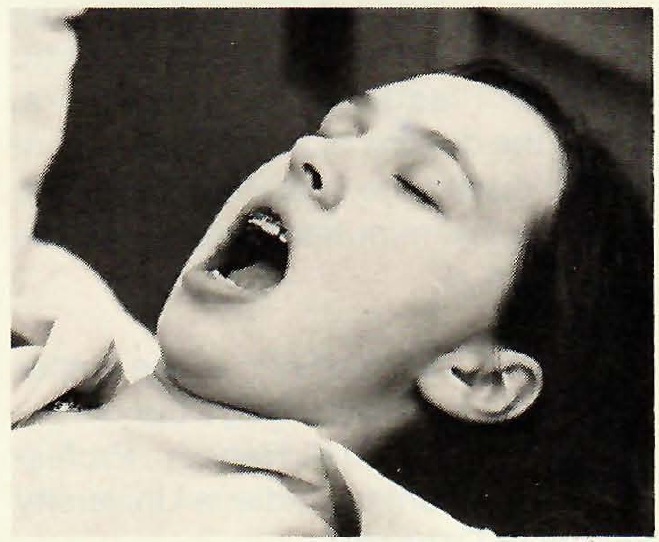
On subsequent visits, the patient was able to make her jaws and teeth numb on request, and it rarely took her longer than a minute to achieve this state. She was also able to "lock" her jaws open for prolonged periods of time without much discomfort (Fig. 4). Appliance adjustments for the duration of her treatment were performed routinely and the patient rarely felt any discomfort. In addition, the patient was given posthypnotic suggestions that greatly reduced the discomfort she had normally felt after appliance adjustments. Treatment was successfully completed and the patient is now in retention.
Conclusion
As far as the author is aware, this is the first report to describe the use of hypnosis for treatment. There is very little doubt that treatment would have been all but impossible without the use of hypnosis. Not only did treatment become possible, but the patient was able to virtually eliminate the discomfort she felt. It is not unusual to hear orthodontists describe the occasional patients who squirm in the chair every time an archwire is activated. The use of hypnosis for such cases ought to be considered, since most orthodontic treatment lasts two years or more. Given the dozens of visits each patient makes during the course of treatment, the extra few minutes of time would be well spent.
ACKNOWLEDGEMENT: The author would like to acknowledge the contribution of Dr. David K. Hennon, Professor of Pedodontics, Indiana University School of Dentistry.