JCO Interviews Martin L. "Bud" Schulman on Fee Management
GOTTLIEB Bud, orthodontists probably have more control over fees than they have over the number of patient starts and costs in an orthodontic practice. Do you agree?
SCHULMAN Yes. I find that, in 1979, orthodontists are taking a more realistic view of fees and their fees are increasing at a more reasonable rate than I have seen in the past. I am very pleased to see that. Obviously, the orthodontic profession is faced with a reduced child population, with higher costs and lower profit percentages and, most damaging of all, the money that is left doesn't buy as much, due to inflation. There is no possible manner in which an orthodontist can continue to make an adequate living, if he doesn't raise his fees substantially.
GOTTLIEB Many orthodontists hesitate to raise their fees, for fear of rejection.
SCHULMAN Just as the level of the salary for an employee is not the primary consideration for employment, neither is fee the primary consideration for almost all patients in the selection of an orthodontist. I feel it is really something other than that. The word, I believe, that is most important is "confidence". If the doctor will convey a sense of confidence to the patient in his ability to deal well with the patient, the patient really feels that fee is absolutely secondary. He doesn't much care about the fee as long as he can afford it.
GOTTLIEB Do you think there should be a differential between a child fee and an adult fee?
SCHULMAN Several studies made in practices which treat lots of adults have determined that an increased fee for treating adults is absolutely in order, and I completely agree with that conclusion. The reason is that, although the adult patient's total treatment time is the same as a child's, and the level of cooperation from the adult is as good or better than cooperation received from the child, the time contributed by the doctor at each treatment procedure is greater with an adult than it is with a child. The doctor must "stroke" the adult, where a chairside assistant can "stroke" a child. Stroking the adult usually requires 20-40% more doctor time per treatment procedure. Therefore, that samepercentage of difference is appropriate for an adult treatment fee.
GOTTLIEB I've always felt that the fee for adults should be higher, but I think that most orthodontists I know have no differential.
SCHULMAN I think that's changing, Gene. I think that now about 50% or more practices have a differential and that the differential is growing. It was perhaps 5-10%, but now orthodontists who are treating lots of adults are up to 25-30%, and some as high as 50%.
GOTTLIEB As nearly as I can tell, the increase in the number of adult patients in the average orthodontic practice has been steady, but slow.
SCHULMAN I agree with you and I think that orthodontists have been just as remiss in pursuing the treatment of adults as most of them have been in pursuing the treatment of children. I'm reminded of the doctor who came to me and said, "Bud, I can't understand why I have about 95% acceptance of my consultations with children as the patient, but only about 60-65% acceptance when adults are the prospective patient". We talked about it at some length and finally agreed that the doctor was not conveying to the intended adult patient the level of confidence that the patient'spersonal commitment would be worthwhile for the results that would be achieved; that, in the end, it really wasn't worth the pain, the regimen of diet and hygiene, the visits on a regular basis, perhaps peer comments and ridicule because of wearing appliances--it wasn't worth all that to get the kind of dentition that the orthodontist was able to offer. So, essentially, the orthodontist was not convincing the patient that the personal commitment was worthwhile. The doctor agreed with this assessment and went home to work at preparing his consultation on a basis that would convince the adult patient that the personal commitment was worthwhile. We both agreed that fee was incidental. Fees related to adult treatment are almost never a cause for lack of acceptance.
GOTTLIEB Should not the same effort be made with children?
SCHULMAN When dealing with children, the parent usually makes the decision. So many children have been treated that parents are well aware of the results and benefits of orthodontic treatment with children. Even though the child may not be wild about entering into orthodontic treatment, the parent convinces the child that it is worthwhile. The adult in this case is already convinced.
GOTTLIEB Some orthodontists do not want to encourage adult patients. How does the orthodontist who is seeking more adult patients find them?
SCHULMAN It's a new area. It must be developed principally by increasing the awareness of the general dentist. I find that a general dentist almost never looks for a malocclusion when examining an adult. When he does see one, he almost never asks the patient if the malocclusion bothers them and if they would be interested in talking to an orthodontist about having it corrected. Can you imagine the number of adults who would be sent for treatment if general dentists would just ask their adult patients if they are bothered by their malocclusions. The job that needs to be done is not so much to educate the adults as it is to educate the general dental community, which should not be difficult to do.
GOTTLIEB The general dentist happens to be dealing with the portion of the adult population that seeks dental treatment and is concerned about teeth and health.
SCHULMAN That's right. Let me change the subject just a bit, still within the general area of fees. Two aspects of fees really bother me and have for a long time. One of these concerns the diagnosis and treatment plan, the most professional service an orthodontist renders; the one area that the doctor never can delegate and, in fact, never does delegate. Yet, the overwhelming percentage of orthodontists give away the diagnosis and treatment plan before they have even told the patient what the fee is going to be. When they do tell the patient what the fee is, they don't even mention that the fee covers the diagnosis and the treatment plan. Then they ask for the initial payment to be paid when the bands are placed or before the bands are placed, which triggers the thought in the patient's mind that the initial payment is for the bands. Then they ask that the balance of the fee be paid over a period of months, usually 24, which triggers the thought in the patient's mind that the monthly visits cost whatever the monthly payments amount to. To complicate this condition even further, doctors frequently say to the parent, "You can have Mary Jane bring the fee in when she comes in each month for her monthly visit". Actually, they should discourage having the fee come in with the monthly visit, because there isn't always a monthly visit; and, if the parent relates the monthly fee to a monthly visit, there is no way in the world that it is a reasonable fee for a monthly visit. I believe that this system for fees is one of the reasons that orthodontists have gotten the reputation among dentists and patients that they charge a great deal and make a great deal of money.I think orthodontists have brought it upon themselves by the way they conduct their consultations and by the way in which they have their fees paid.
GOTTLIEB You would still advocate a substantial initial payment, wouldn't you?
SCHULMAN Yes, but I would much sooner see the initial payment related to the decision to undertake treatment; and when a parent says, "I would like you to treat my child", the initial payment would be due at that time. The fee payment would be related to the acceptance of treatment. I would not relate any particular portion of it to bands and I would not relate the monthly payments to any aspect of treatment. The fee really is to cover a diagnosis, a treatment plan, and aseries of treatments to correct a particular orthodontic problem. For many years, I have been trying to get orthodontists to change the way in which consultations are conducted and the way that the fee is presented. Those who do change are always pleased that they did.
Another area that bothers me is transfer patients. Transfer seems to be a universally unhappy basis for undertaking treatment. Quite frequently, the doctor who is transferring the patient will tell the patient that they should be able to have the treatment completed for the unpaid fee. The new doctor, in order not to give the former doctor a bad name, will pretty much go along with completing treatment for the unpaid fee. It's really quite unfair.
GOTTLIEB What do you propose?
SCHULMAN There is never a patient transferred for whom the new doctor does not do a new diagnosis and treatment plan. He has to evaluate the patient's present condition and decide how he wishes to best complete the treatment. I believe that there should always be a transfer fee for this diagnosis and treatment plan; and I believe that the doctor who sends the patient to the new doctor should always say, "You can expect the fee to be larger than the unpaid portion of the fee that we originally arranged. There will be a fee for the new diagnosis and treatment plan".
Now, that's half the problem. The other half of the problem relates to an orthodontist undertaking the care of a transfer patient at no fee, in most cases, for the entire retention period. I believe that the new orthodontist is entitled to a fee for the retention period for transfer cases.
GOTTLIEB So, you would advocate at least a diagnostic fee and a retention fee on transfer cases?
SCHULMAN I'd like to see not less than a $200 diagnosis and treatment plan fee for every transfer orthodontic patient and I'd also like to see an adequate fee to cover retention for every transfer case. Together, they might perhaps amount to a minimum of $500-600 that any transfer case might have to pay upon going to another office.
GOTTLIEB A problem that often arises in transfer cases is that the appliance in place is not suitable for the second orthodontist. In order to achieve his best result, he feels that the appliance should be replaced. Should there be a fee for that?
SCHULMAN If the orthodontist feels that he would like to change the mechanics, I believe that some compromise fee is in order. I don't believe that the doctor should undertake to do if for nothing, as many do. One might add half of his strapup fee, which is essentially his cost, because the average orthodontist has costs of 50% and profit of 50%. Charging 50% of his regular fee for installing new mechanics means that he is donating his services for nothing for that phase, in order to satisfy himself that he would be treating the case in the manner in which he felt he could secure the best results.
I don't believe that he should give away his staff, his supplies, his rent and all his direct costs of getting the new mechanics installed.
GOTTLIEB What is the obligation of Orthodontist A in regard to fee?
SCHULMAN I don't think that Orthodontist A generally prepares the patient for the fact that there may be changes in mechanics and an added fee. I think too many orthodontists, in an effort to have the patient like them when they leave, indicate that the treatment should be completed for pretty much the unpaid fee, and that's a sad position to take. That's an improper position to take. It's wrong not to prepare a patient at the time of transfer for a rather substantial additional fee.
GOTTLIEB Yes. I think it is part of the price of moving. Is a refund sometimes called for?
SCHULMAN By Doctor A? Oh yes, particularly if the fee is paid in advance. Doctor Aundoubtedly has an obligation to refund whatever portion of the fee has not been used.
GOTTLIEB Doctor A frequently may feel that lack of cooperation has prolonged treatment and he may find justification not to make a refund, even if much treatment remains to be done.
SCHULMAN The orthodontist does not really know when he sets his fee whether he is going to receive reasonable cooperation. Frequently, orthodontists will allow treatment to extend without adding to the fee, primarily out of the goodness of their hearts. It is hard to be precise about something that is an art. But, it makes it most difficult on transfer.
GOTTLIEB So, this is another aspect of fee--a contingency against noncooperation.
SCHULMAN Yes. I really believe that an open fee, which was common practice years ago, was fairer to the doctor and to the patient. The problem with an open fee was that from the time the anterior teeth got into alignment, the patient believed that the doctor was continuing treatment only to increase the fee. Even though the patient sometimes overpays and sometimes underpays, patients prefer the fixed fee and obviously most orthodontists agree, because 95% of all fees today are fixed fees.
GOTTLIEB Do you think a fee range would be superior in any way to a fixed fee, and a compromise between the two?
SCHULMAN I don't think that patients would like it. I think you'd find it difficult to raise the stated fee level merely because unexpected difficulties are encountered. I also feel that it is just as wrong to give away part of a fee for finishing early. I think that, on the average, the fee should be about where it is on a fixed fee basis. Some patients will undoubtedly finish early and will perhaps have paid more on a per-hour basis. Others will take longer, and for that the doctor will receive no added fee.
GOTTLIEB Do you not believe in a contingency that would extend the fee, by continuing monthly payments, in the event of noncooperation?
SCHULMAN Well, I actually do believe in extending the fee in the event of noncooperation, but I believe that you must arrange for it at the time of the initial consultation. If the patient has not been told in advance that lack of cooperation may lead to a larger fee in the event of extended treatment time, you really can't institute it a year or two later. The other aspect of extended treatment is the most difficult case, such as a skeletal open bite, which I think many orthodontists handle wrongly at the time of consultation. I believe that they should undertake to treat the patient for perhaps 24-30 months--whatever period they feel is appropriate--as a first step; and then do another diagnosis and treatment plan and decide if they wish to go further. In many cases they may decide that they do not recommend further treatment. If the doctor does decide that he would like to go further,feeling that there could be further improvement, then the patient should be given an added fee to go into another stage of treatment.
GOTTLIEB Patients will accept the idea that you have gone as far as you reasonably can go and they are willing to terminate a case that is not corrected 100%, realizing a lot more readily than most orthodontists believe that perfection is sometimes an elusive thing. If you set it up in advance that this case is difficult and that we'll treat it for 30 months; do the best we can; and then reevaluate it at that time; and you and I together will decide how much we have accomplished; and whether,for an additional amount of time and fee, we feel that we would gain that much more by continuing; that sounds pretty logical.
SCHULMAN I think it is reasonable. It is similar in some ways to two-stage treatment in children. The doctor is always faced with the problem, if he states the fee just for the first stage, that he has to receive acceptance again before he can begin the second stage. The other side of the coin is that, if a fee is quoted for both first and second stages at the start of the first stage, the patient has no further choice to make since they agreed to be treated for both stages; but, the problem is that this arrangement discounts the effect of inflation over too many years to make it justified. I must say that the difficulty with giving the patient a choice of whether or not they wish to proceed into a second phase is that a fair number of patients decide not to do it, much to the chagrin of the orthodontist. So, that is a problem.
GOTTLIEB Bud, let me take you through a sequence. A patient calls for a first appointment. They've been referred by Dr. So-and-so. Is there going to be a fee for that first visit?
SCHULMAN My feeling is that there should not be a fee for that. It is similar to the first contact with an accountant or a lawyer, at which time you are trying to decide whether to retain them. There is never a fee for the initial consultation.
GOTTLIEB So, you believe that the orthodontist should have an open door policy?
SCHULMAN Yes. In spite of the fact that I believe that the patient would be prepared to pay a fee, I don't think one should be charged, because it is so valuable to be able to have a referring dentist feel comfortable in sending a patient to you to see if that patient has an orthodontic problem.
GOTTLIEB Now this patient comes to see you and you determine that they have a problem, but it is not ready for a diagnostic workup. You must see them again in 3 months or 6 months. Do you recommend seeing them until they are ready for a diagnostic workup still at no fee?
SCHULMAN No, I don't believe that no fee is in order. Once the patient has entered the practice, fees are in order. I believe that every appointment that the patient returns for an other examination and evaluation justifies a fee. I have seen a development in recent years where the orthodontist will establish a reasonable fee to cover the entire period of recall and observation until some final disposition is made.
GOTTLIEB When the case is ready for diagnostic records, should the patient be informed what the fee will be for diagnosis and treatment planning?
SCHULMAN A fee is definitely in order and, no matter what fee is charged, it is usually inadequate because the orthodontist must do so much of the diagnosis and treatment planning himself. He can't delegate that aspect of the program. The most he can delegate is some of the record taking, but the decision-making must always be his. Most orthodontists don't talk about the value of that particular visit, unless the patient does not accept treatment. Then they might present the family with the bill for diagnosis and treatment planning in the area of $75 to $200.
GOTTLIEB Do you think it is preferable not to create a possible stumbling block at that point in the relationship? Or, would it better to establish just what the financial obligation will be prior to taking the diagnostic records?
SCHULMAN I think that most doctors say at the first visit, "I would like to take diagnostic records of your child and do a diagnosis and treatment plan and present the results to you at our next meeting. If you then enter my practice for treatment, assuming your child needs treatment, that will become part of the overall fee. If you do not enter my practice for treatment, either because you choose not to or because we find that your child does not need orthodontic treatment, there will be a fee for the diagnosis and treatment plan of so-much money".
GOTTLIEB The word "shopper" enters my mind at this point and I wonder how you feel about that. Do you feel that a person has a legitimate right to shop, and what can or should the orthodontist do to protect himself against shoppers?
SCHULMAN That's an interesting point. I believe that most people are more prepared to undertake treatment on their very first visit than they are at the second or third visit. If the doctor would be prepared at that visit to make a commitment as to the need for orthodontic treatment and the type of treatment indicated, in general a way without being specific about the exact treatment plan until one can be presented, that really thwarts the shopper, because he is presented with a total fee at that first visit before a diagnosis and treatment plan has been presented. If the patient decides that the fee is unreasonable, the patient leaves before the doctor has done any work on the case, other than an initial and superficial examination and an estimate that is not binding as to the type of problem and the general kind of treatment procedure to be followed.
I believe that the two-consultation technique was initially designed as a device to justify an $800 fee. It was felt that a doctor could not present a diagnosis and treatment plan that would run $800 without two visits to build the patient up to the level of confidence at which they would accept an $800 fee. I maintain that the psychological approach today is quite unnecessary.
Patients today are quite prepared to undertake fees of several times that $800 fee without multi-visit buildups.
GOTTLIEB How does the orthodontist starting out decide what the fee ought to be?
SCHULMAN I believe that the new orthodontist in an area almost always takes a fee that he believes to be a little bit lower than the fee of established orthodontists in his area, and that is probably a reasonable fee philosophy for him to follow.
GOTTLIEB When and how does he raise his fees?
SCHULMAN Raising fees involves a great emotional strain for most professionals. They really hate to raise their fees. They have all kinds of mental anguish associated with raising fees. They look for reasons not to raise their fees. The orthodontist nearby has not raised his fees and, therefore, they are reluctant to raise their own. I maintain that fees only occupy third position in people's decisions to undertake treatment. If I could convince doctors that the fee is not as important to the patient as they believe it is, the whole professional would be better off. There is no question that some people will shop fees. Those are the people who set up these doubts in doctor's minds, when actually the doctors are probably better off without those patients anyway. But, orthodontists always seem reluctant to raise their fees. They subject themselves to a terrible emotional stress whenever it comes to fee-raising time.
GOTTLIEB Do you have any suggestion to relieve that stress?
SCHULMAN One device that may be helpful is for orthodontists to raise employees salaries once a year and, at the same time, raise their fees by a relative percentage.
GOTTLIEB With annual increases in cost and with inflation, the orthodontist shouldn't have much difficulty convincing himself that he must increase his fees, but there is a lot of pressure of competition out there, in spite of the fact that the Federal Trade Commission doesn't think so--it's one person against the world out there.
SCHULMAN Without an annual reevaluation of fees, the orthodontist stands to take an annual income reduction.
GOTTLIEB What do you consider a preferable way to present a fee? Is it in one figure--"The fee will be $2000 to treat this case"?
SCHULMAN I believe so, Gene, and it should be part of a compound sentence, such as--"The fee for treating Mary Jane's problem is $2000, and the time during which Mary Jane will be in active tooth movement will probably be 24 months". Or the doctor might say," . . . and this kind of problem can usually be corrected in about 24 months".
GOTTLIEB Does the doctor present the fee?
SCHULMAN I believe the doctor should mention the total fee, but not make the arrangements for payment. As a matter of fact, if the patient were to say to the doctor at the same time the fee is stated. "Doctor, how do I pay that fee?", the doctor should say, "Well, my secretary works something out with everyone. She seems to be very good at that". With that, he dismisses himself from further relationship to the money, which patients seem to prefer. I'm reminded of Marcus Welby on television who is much loved by all of his patients. If you have ever watched the show, I think you may realize that in all the years he has practiced medicine, he has never yet charged a patient a fee.
GOTTLIEB No wonder he's loved!
SCHULMAN Psychologically, it is quite valid that the doctor should divorce himself from the money. Patient's like it and I think that people other than the doctor can deal better with the money.A trained secretary should present the different payment alternatives.
GOTTLIEB What alternatives do you favor?
SCHULMAN One of the alternatives should always be payment of the entire fee in advance. In that case, the patient may use that payment as an income tax deduction as a medical expense. In myobservation, only a very small percentage of orthodontic practices offer that option.
GOTTLIEB Should there be a percentage discount inducement for payment in advance.
SCHULMAN In almost every case, a discount is illegal. If you state that there is no interest charge for payment on an extended basis over a period of many months and then give a discount for payment in advance, it really means that you are charging a premium or interest to people who do not pay in advance, to the extent of the discount given. Therefore, your statement that you do not charge interest is untrue and is in violation of the Truth in Lending Law.
GOTTLIEB That law is still in force?
SCHULMAN Yes.
GOTTLIEB And orthodontists should still be filling out those Truth in Lending forms?
SCHULMAN Oh yes. The contract for treatment should still be completed.
GOTTLIEB Since it is a contract, any fee contingencies, such as for lack of cooperation, should be included, shouldn't they?
SCHULMAN It is quite a valid contract. It should state whatever fees and contingencies there may be.
GOTTLIEB Do you suggest asking for a large initial payment?
SCHULMAN I think that the patient should be given a choice of initial fees, the smallest of which is probably the amount the doctor is presently proposing and that there should be alternate choices for initial payments, all calling for larger payments initially, with correspondingly smaller monthly payments.
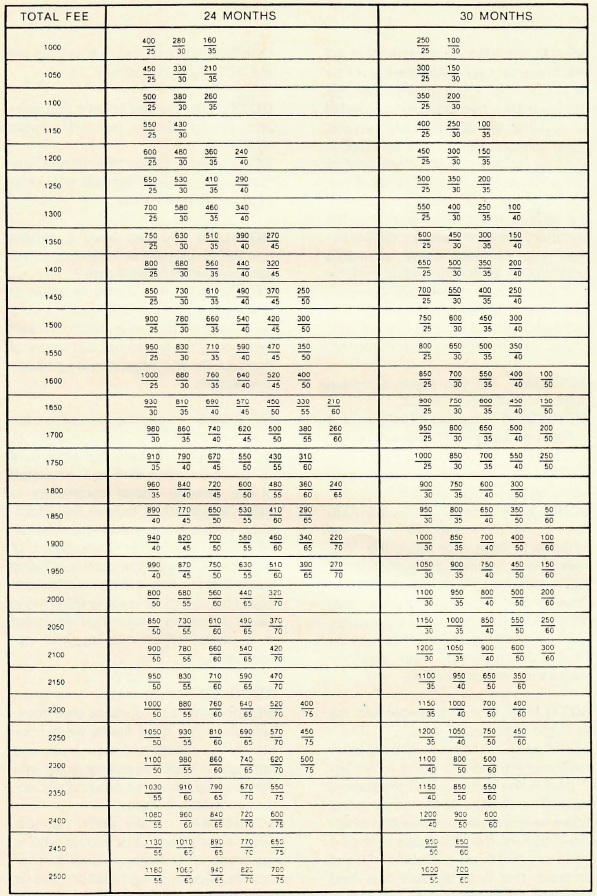
GOTTLIEB Do you still suggest the DCA formulas?
SCHULMAN Yes. Here is an updated version of that.
[show_img]190-jco-img-1.jpg[/show_img]GOTTLIEB How do you suggest handling delinquency?
SCHULMAN I feel somewhat differently about that than many people do. I believe that nonpayment of the orthodontic fee is really related to expectations on the part of the patient as to whether the fee must be paid promptly. If a patient believes that the practice is going to require prompt payment of the fee, in almost every case the fee will be paid promptly. If the patient does not believe that, or has been given no belief as to what the practice will require, many patients will test the practice to see how far they can stray from prompt payment before the practice takes action. So, it is really quite important at the time of the consultation that the secretary say to the family, "We will expect you to meet these payments promptly". I think that should then be reinforced by a letter that confirms treatment, so that the patient has a good understanding that the practice will require prompt payment of the fee.
GOTTLIEB Do you have a limited number of months in mind?
SCHULMAN I believe that 24 months is about as many as most practices go.
GOTTLIEB How do you feel about handling the fee for retention?
SCHULMAN Many orthodontists have found that if they didn't have the fortitude to raise their basic fee, they were able to institute a retention fee of $200 and really felt no resistance. Other orthodontists in the area, with whom they felt they were competing, really weren't aware that they had instituted that fee and, in fact, that their fee was increased by $200.
GOTTLIEB Is that arrangement set up in the beginning?
SCHULMAN It is covered in the letter confirming treatment, but it is not included in the contract that the patient signs. The contract is for the period of active treatment only. At the end of active treatment, the office calls to remind the family that there is a retention fee of so much that is to be paid now, and asks how would they like to deal with it. Orthodontists who use this system tell methat it works quite well.
GOTTLIEB Do you believe that anyone should receive free orthodontic treatment?
SCHULMAN Only the immediate families of general dentists who refer patients to the practice.
GOTTLIEB Do you have a certain number of referrals in mind to qualify a general dentist for free care?
SCHULMAN It is certainly unfair of many general dentists, who are not in a position to reciprocate, to accept treatment on a no-fee basis, but many of them do. By and large, it is an unhappy arrangement.
GOTTLIEB Is anyone entitled to a fee discount?
SCHULMAN I believe that a discount of 10% to your own staff and to the staff of the general dental community is quite reasonable. I believe that chairside assistants in general dental offices are entitled to a discount of perhaps 50%, with the comment being made that treatment is being offered at cost. I believe there is some advertising value in having a chairside assistant in a dental office wearing your appliances.
GOTTLIEB There was a time when orthodontists did not raise their fees, because their case starts were constantly increasing and their gross and net income kept increasing along with that. Do you think this productivity approach to fees is valid?
SCHULMAN I really don't. I almost never encounter a practitioner who is not prepared to have a higher level of income. Considering inflation, this is quite valid.
GOTTLIEB Of course, orthodontists do not really know how many patient starts next year will bring. It makes planning difficult.
SCHULMAN It's interesting that people have asked me what their goals should be and I say that they should really have two goals. One goal is to try to start more patients each year; and a second goal is to maintain their level of gross income or perhaps have it exceed the previous year. That's a minimum goal and, if they can't meet that goal, they should begin to think in terms of some radical changes.
GOTTLIEB That's absolutely true, because if you stand still you are falling behind. Do you have a concept similar to anticipatory pricing used in business to raise prices in anticipation of increased costs and inflation?
SCHULMAN Gene, it's hard to do. All you can do is fight your battle year by year. You really can't be that precise.
GOTTLIEB I have a feeling, though, that orthodontists would be more comfortable if they had some formula basis to justify fee increases in their minds.
SCHULMAN It could be done as I suggested, by applying the same increase to fees annually as you do to salaries of employees. It is a fairly logical approach to the problem.
GOTTLIEB And, I think that percent might cover both the kind of cost increases and inflation that we have been experiencing, although it might be slightly low at this point.
SCHULMAN Well, orthodontics in general has not kept pace with inflation. The proof of that statement is that the profit percentage has declined from 60% to 52% since 1970.
GOTTLIEB Is there a $2000 fee barrier?
SCHULMAN I don't think it is a barrier. I don't think doctors feel it is the barrier that the $1000 fee was some years ago. This year, I am seeing a growing percentage of doctors coming right through that barrier with no hesitancy at all. They are having no problem.
GOTTLIEB Are orthodontists controlling costs as well as they should?
SCHULMAN I've seen practices with a 75% profit percentage, but I think that on the average a profit percentage of 52% 55% 57% is reasonable. I have also encountered one 17-year-old practice that had a 16% profit level. I was appalled by it and the doctor was scared to death by it.
GOTTLIEB Can you budget costs in an orthodontic practice? Can you say, "I'm going to have a 50-50 cost/profit percentage next year and it is going to be allocated in this percent for rent, this percent for salaries, etc"?
SCHULMAN Well, I believe you can't. Many of your expenses are uncontrollable. The balance is only controllable if you also can control the number of incoming patients, but that also is uncontrollable.
GOTTLIEB Where can costs be cut?
SCHULMAN There are very few places you can cut.
GOTTLIEB Are orthodontists over-hiring, for example?
SCHULMAN Some do.
GOTTLIEB Are they permitting salaries to escalate automatically with annual increases without regard to performance?
SCHULMAN Some do. Labor averages about 16% in most practices. In the practice I mentioned with the 16% profit margin, his labor percentage was 30%. That's not too uncommon. But, there are so many ways that employees' costs can be out of line, that it almost has to be approached on an individual basis. It could be that the employee benefits are unreasonable. It could be that the wages are too high. It could be that the performance standards are too low. It could be that there are too many employees. There are all kinds of reasons.
GOTTLIEB Do you subscribe to an hourly wage?
SCHULMAN I much prefer that people be paid by the hour or by the day, than by the week or by the month.
GOTTLIEB Why?
SCHULMAN Because it's more definitive. When employees are paid by the hour, it's less expensive when the doctor is away. Where employees are paid by the week or month, the doctor's absence usually results in the employees being paid without working, which to me seems unreasonable.
GOTTLIEB How close to the vest should the orthodontist think of operating with regard to costs?
SCHULMAN You must think of a practice as being similar to a business, with one primary advantage. The average well-operated business will have a net profit percentage of 5-20%, whereas the average profit in an orthodontic practice is in the area of 50%. The businessman must be terribly careful in order not to have his costs become unreasonable and lose his profit. A professional in a practice can be more relaxed, particularly if his gross income is at a satisfactory level. It isn't too painful if his profit percentage slips from 50% to 44% or 40%. He may not care to have a real tight operation. If he doesn't care, it's perfectly all right. I find no fault with that, but I think he should be aware of what he is faced with and, if he does care, he should look for better performance. If he doesn't know how to make it better, he should find out.
GOTTLIEB To go from 60/40 to 50/50 would mean either reducing costs by one-sixth or 162/3% or increasing gross income by 20%. Do you believe it would be easier to increase the gross under those circumstances than cut the costs?
SCHULMAN Yes. I believe that it's easier to raise gross income that it is to reduce costs. Most costs defy reduction, whereas income can always be increased through better practice building performance. One advantage is that all added income normally carries only an increased cost of perhaps 25%, which are the variable costs. That would be labor and materials.
GOTTLIEB That's an interesting point. Once you have established a practice, the cost of each additional patient is an entirely different matter. It does not involve just dividing the number of patients into the cost to get a unit cost.
SCHULMAN Yes, because costs are divided into two areas, fixed and variable. That is why doctors have such a terrible time starting a practice. Once the practice is established, adding patients should raise the profit percentage, because instead of making 50% on the additional patients, you should be making 75% net profit, because all of your fixed costs--such as rent, utilities, repairs, dues and subscriptions, insurance--are not variable and don't increase with more patients being treated.
GOTTLIEB That's right. After the break-even point on your fixed expenses, you are operating at a different cost/profit level.
SCHULMAN Well, you see, businessmen are very aware of these differences, whereas doctors never really pursued this level of sophistication in their practice operation, due to the nature of their education and frequently to the absence of a need to know.
GOTTLIEB Do you think that doctors are going to have to pay more attention to this in the future?
SCHULMAN No, I don't. If they can maintain their practice gross incomes at a healthy level and with a good rate of growth each year, they don't necessarily have to be any more aware of how their costs are arrived at, as long as they are satisfied with the results. It's really a kind of personal thing.
GOTTLIEB You think that orthodontics is going to continue to be a happy and lucrative profession?
SCHULMAN Oh, you bet. There are very few vocations in which people are as well off as medical and dental practitioners. They control their own destiny, they earn good incomes, they have choices in terms of investments, they can accumulate quite good amounts through pension and profit sharing plans that enable them to retire quite comfortably. Most people don't have the choices that practitioners do. Most people work for large companies; the company tells them what to do; they retire, at best, on modest retirement programs; they don't have the choices of time commitment. Most doctors don't have to work the number of hours to generate their incomes that most people in commerce and industry do. So, doctors really have all sorts of wonderful advantages. By the sametoken, they are bright, committed people who devote their lives to their practices and their patients. But, I think doctors are treated quite well, accordingly.
GOTTLIEB Do you think that the variety of alternative delivery systems--retail dentistry,clinics, franchises, etc.--represent a threat to this way of life and will have an adverse affect in depriving practitioners of their autonomy and their income?
SCHULMAN There are inroads being made. Whether the changes will have a profound effect or not is hard to say. I think that the fee-for-service practice is the most desirable kind of practice there is. If I were an orthodontist, that is the practice I would seek. In my judgment, I don't believe that fee-for-service practices will ever fall below 65% of all orthodontic practices in the U.S.
GOTTLIEB Well, Bud, you have covered our subject in a broad and interesting manner, and I want to thank you on behalf of the readers of JCO.