ROUND TABLE
Retention
Round table participants: Drs. Arthur I. Thomas, Howard D. Dimond, Walter S. Bogad, Howard S. Spurrier (Moderator), Harry S. Galblum, and George W. Moss.
DR. SPURRIER: Will someone begin this discussion on retention by relating some of his ideas concerning retainers?
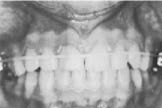
DR. BOGAD: In my practice I use mostly removable acrylic appliances, upper and lower. Most of the time they are modified Hawley retainers with acrylic on the labial bow for retention of the retainer (Fig. 1). These appliances were introduced by Dr. Herbert Margolis.
For severe Class II cases, I don't use removable retainers. I remove all of the bands, recement the molar bands and go back to headgear for a year or so.
DR. SPURRIER: Does that include a circumferential elastic on the anteriors?
DR. BOGAD: Yes. Where the ANB was excessive initially, a real extreme case, I find that the anteriors tend to relapse to some extent-- even with adequate lingual root torque and nice axial inclinations. I feel safer retaining with the headgear and elastic.
DR. SPURRIER: That elastic can get you into trouble, though. I've seen some, on a transfer basis, where the patient hasn't been seen by the orthodontist in six months. And, if they're wearing their elastic more than their headgear, they have a pretty crowded upper arch.
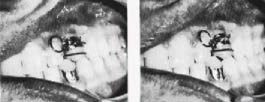
DR. BOGAD: I do not run the elastic from molar to molar (Fig. 2). I solder two hooks on the inner bow of the headgear and the elastics (¾" latex) are worn off those hooks (Fig. 3).
DR. DIMOND: When we start talking about retention, we should discuss philosophy before we get into mechanics. In the first place, what is retention, is it necessary and why should we have it-- if we do have it?
My philosophy calls for the use of very little retention. I expect a certain amount of collapse. I've told that to my patients before starting treatment. Are we fooling ourselves or being a little
dishonest in postponing a collapse that we are going to get anyway?
One of the papers presented this very morning (at the 1969 AAO Convention in Miami) a lecturer said he finishes his treatment and places 3-to-3 cuspid retainers. He leaves them on as long as the patient will wear it. Well, then what does he do? Will there be a collapse? If so, wouldn't it be better to have debanded and not put on that 3-to-3? Just try to get as good a result as you possibly can when you finish the case.
DR. GALBLUM: I think the philosophy of the people who use the 3-to-3 for an indefinite period is that they feel-- they hope-- that the environmental structures including the periodontal membrane and the musculature will readapt in a period of time. And, they feel that the longer they wear it, the better the chance to readapt.
DR. DIMOND: Philosophically, I can't justify a feeling that growth will help us, considering that the problems that we are having are being compounded by growth. Your patient is losing facial fat, the orbicularis oris and buccinator muscles are becoming more and more tense. The third molars are erupting. The chin button is getting bigger, not smaller. Statistically, the anteriors have a tendency to upright. How is leaving the 3-to-3 in there going to help us?
DR. SPURRIER: One point in favor of the retainer is the work that Reitan did years ago on the amount of time that recalcification takes. Some took 9 months, some 18, some 24. Some patients-- or monkeys as it were-- never did recalcify. On that small percentage of patients where the apparatus never returns to normal, the retainer is a good thing to have in place. And, on those where it does return to normal in a proper amount of time ( 9 or 18 months), then I like to have the retainer on there to give my patient the benefit of alignment during recalcification.
It's the same philosophy where a parent will say, "We don't want perfectly straight teeth. They look like dentures." But, the same parent is on the phone with one degree of rotation during retention. So, we do make the teeth as nearly perfect as possible, because we anticipate a little collapse. And the reason we hold for 18 months is because we don't want them to collapse during the recalcification period.
DR. DIMOND: Well, I'm not talking about the men using a retainer for a year, possibly a year and a half. I'm talking about the person who finishes the child at 13 or 14 years of age and keeps the 3-to-3 on until he's 20 or more, and has him wear the upper retainer at night. And, that's his minimal retention.
DR. SPURRIER: Well, let me say this one thing. Retention becomes easier as we deal with older patients. Don't you find that in your practice?
DR. DIMOND: I don't retain to any great extent. I do place positioners, which are a form of retention (Fig. 4). I question how long the patients will wear them. The positioner is such an awkward device that it is very difficult to get them to wear it very long.
I do get a very small number of cases that crowd up. But, I feel that I would get them anyway.
DR. SPURRIER: The men in our area, myself included, follow Reed Holdaway. Our philosophy is that if you can maintain the occlusion to the point where the mature upper and lower third molars are in place or where they have been extracted and all the muscles are as mature as possible, then retention can be discontinued.
That's why the seven years. I think most people in our area will keep that cuspid-to-cuspid on at least that long. Seven years, or more.
DR. GALBLUM: I leave them on 2 to 3 or 4 years depending upon how courageous I feel when I take them off.
One important thing in retention is how the case is stripped. Bob Moyers takes off everything but the molars and canines, one arch at a time. I used to do that and I found, unless I was real careful, and even then, sometimes the incisors rotated during the stripping process.
So, I always leave my incisors and molar bands on until the end. Then we put a 3-to-3 on the day we take off the incisor bands. The 3-to-3 can be done directly.
The two cuspid bands are fitted and an arch wire bent. This is tack welded on one cuspid and reseated in the mouth. Then the other side is tacked and they are put back in the mouth. If they look good, then you solder. And, if you're lucky, they fit.
DR. DIMOND: You fellows may have seen the way I deband. It was in JPO (January, 1968). I take off everything but my maxillary and mandibular canines and molars and I run an elastic ligature around (Fig. 5). That ligature is only left in for the time it takes to make a positioner. It pretty well closes up the spaces and the positioner finishes it off.
How do you fellows remove your bands?
DR. MOSS: I think we share a lot of Howard's opinions in our practice. We try to anticipate retention. About 25% of them are never retained. And, we suspect that another 25% that we are attempting to retain are not wearing retainers. Which puts us in about the 50% category.
When we finish a case out, we remove all the archwires, leave all the bands in place, and let the case go for 6 weeks. At the end of 6 weeks, if we don't see a noticeable change, we then strip the case and don't use any retention. If we see a change, we come back to archwires and finish the case out in another appointment and prepare ourselves for a long retention period.
DR. GALBLUM: It's interesting how many different philosophies and techniques there are.
DR. MOSS: Fundamentally, we seem to have two contentious groups. One that will say they never retained an orthodontic case, such as Strang. Then, you have those such as Reed Holdaway and Charles Tweed that will retain as long as the patient lets them.
The terrific polarization about these two views doesn't make it seem that they could both be right. But, they can both be right in part. In other words, a certain case may not need retention, another has to be retained at night, another should be retained for the rest of the patient's life or the duration of his dentition. What do you retain and how?
DR. GALBLUM: I think anyone who has severe rotations and doesn't retain is very courageous.
DR. BOGAD: I don't think too many people retain good lower arches if they were not part of the treatment or were merely leveled in treatment.
DR. DIMOND: There are always exceptions. Where you had spaced upper and lower anteriors, forever retention plus a splint may be indicated.
DR. THOMAS: The only time I don't retain in the lower arch is where I don't use Class II mechanics. If you start a maximum arch length discrepancy case or a case wherein the tooth size is abnormally large, you'll have to retain.
DR. MOSS: I do not use any lower retainers.
DR. DIMOND: I never have, either.
DR. GALBLUM: How many of us who get some crowding of the teeth during or after retention strip the teeth and go back and align them?
DR. MOSS: Almost everybody is forced in this direction occasionally. I think a better time for stripping though is at the time the bands are removed.
DR. DIMOND: If you can anticipate it. When do you balance and when do you strip?
DR. MOSS: I think the point that Bob Moyers makes is important. There is a direct correlation between anterior crowding and the forward slide. It is one thing we always look for when we determine retention requirements. Our objective in equilibration is to prevent a slide.
DR. GALBLUM: We've had a particular retention problem which others may have had. When we finish a case, we try to do it with a minimum of overjet and overbite since we expect these to increase. But sometimes, the lower jaw comes forward. Can you anticipate these problems?
DR. MOSS: This is bound to be a growth problem. This is something you really can't control.
DR. GALBLUM: We handle it in various ways. Sometimes, taking a lower incisor out, sometimes using a lower headgear. I know of somebody who uses a lower Margolis ACCO. But, it would be nice to anticipate this.
DR. SPURRIER: With a high ANB difference, you wouldn't anticipate it. With a 1° or 2° angle, you've got to be careful.
If you do have an edge-to-edge problem and you have headgear bands in place and a 3-to-3 in the lower, just run a light latex band from the upper band down to hooks on the cuspid-to-cuspid. That irons it out if its not a big discrepancy.
DR. GALBLUM: When do you take impressions for upper retainers? We take it the day the incisor and molar bands come off and we're sure to get the retainers on within the week.
DR. THOMAS: I wait about 10 days before taking the impression.
DR. MOSS: Reitan says you get some relapse in 30 minutes. We make the impression the day we remove the bands and the patient is scheduled a week later for the retainer.
DR. DIMOND: I routinely use a positioner. We strip everything and take impressions. Then we recement the molar and canine bands and put an elastic on to close the spaces up. About 10 days later we remove them and place the positioner.
DR. SPURRIER: What other problems affect retention?
DR. BOGAD: I think everyone feels that if you have a reverse swallower or a related problem, you'll try to retain as long as possible. But, I don't know if you'll ever cure those things.
DR. GALBLUM: For tongue thrusters, we use positioners. The way most positioners are made tends to increase overbite.
DR. DIMOND: If you take the acrylic retainer and drill a hole in the area of the rugae about ¼" wide and leave it rough (Fig. 6) the patient will play with it and keeping the tongue in that area may become a habit. But, with all the exercises, mints and speech therapists, I haven't seen successful tongue training.
DR. MOSS: The results have been disappointing.
DR. BOGAD: The kids are smart. They say, "When I think about it, I swallow your way. When I don't, I swallow my way."
DR. SPURRIER: What about the chin cap?
DR. THOMAS: I use them in maxillary deficiency cases with elastics off the horns where I wish to move the upper denture forward. As far as restraining Class IIIs or Class III tendencies, I don't think anything has been proven to support that contention.
DR. SPURRIER: Any comments on mid-palatal disarticulation retention?
DR. THOMAS: In the deciduous dentition, where correction is done in a week or two, the maintenance is excellent and retention is not essential.
In the mixed dentition, retention is good but should be reinforced with a plate to hold it.
In the permanent dentition, about ages 12 to 16, relapse can occur. But, we haven't had bad relapses. These should be retained.
DR. GALBLUM: Two things that must be retained include the upper lateral incisor that was very lingually placed in crossbite with the root palatally and the palatally impacted cuspid. We spend a lot of time putting labial root torque into those laterals and/or cuspids but they still tend to go back.
DR. SPURRIER: Lateral incisors tend to be bugaboos-- particularly with rotations. I'd be afraid not to retain those.
There's a good little appliance for retaining cuspids that tend to go back up and in. It's an acrylic appliance with an arm that comes off one of the clasps. You bend a loop in it, bent back on itself. Solder 2 hooks on the cuspid band and recement it. Then activate the wire down and out to the position you want the tooth. The patient puts the appliance on and places the spring forcibly into the hooks on the band with a twisting motion and it torques the tooth down and out. It works beautifully (Fig. 7).
DR. GALBLUM: What about equilibration? When do you equilibrate?
DR. MOSS: I do it whenever I see the need for it-- usually before the end of treatment, but before I get the bands off.
I don't know if I have any orderly or routine way of doing it. I watch for a slide. That's all I try to equilibrate for. I don't feel qualified to do any other type of equilibration.
DR. GALBLUM: We try to take care of any slides with the appliance without equilibration. It sometimes means we have to recement bands to get improved tooth positions. I think orthodontists create as many slides as, perhaps, they cure.
DR. DIMOND: How many cases, after being under retention for a while, start to exhibit temporo-mandibular joint disturbances? I've had this happen.
DR. THOMAS: Frank Celenza, a gnathologist, points out that temporo-mandibular joint problems may be subclinical before we start. The potential may be there and it comes out during or after treatment. He feels that the cases should be equilibrated. Most of the problems could be eliminated.
DR. GALBLUM: There's something to be said for eliminating prematurities and for the psychosomatic aspects of TMJ problems. A lot of the problems are due to grinding and clenching.
DR. MOSS: Don't you find that most of the problems we see in our patients are transitory?
DR. GALBLUM: That may be why I've treated them so well.
DR. BOGAD: What about the patient who comes in with a TMJ click, goes through treatment with the click and gets a nice dental result with a click?
DR. DIMOND: You do a Spanish flamenco.
DR. BOGAD: Either that or you tell the patient not to sleep at night. But, be sure to tell the patient about the click prior to treatment.
DR. DIMOND: This brings up another point. All of us, whether we retain for 15 days or 15 years, are going to have a certain number of cases that collapse to an extent. Some very few are going to be a problem no matter what. We even tell the patient beforehand that we expect improvement but never perfection in our results and we mark it down on their records. It's a peculiar thing that when the patient comes back four years later, after a slight collapse, they don't seem to remember or have the paper I gave them.
DR. GALBLUM: The orthodontists may not be communicating with the parents. But, no matter what we say, the people remember what they want.
DR. SPURRIER: It is interesting to see how non-standardized our ideas and procedures are with regard to retention. I have a feeling that we need to pool our experiences more than we have if we expect to come up with knowledge about retention that will tell us when to retain, how long to retain, and with what appliance to retain.