Bonding Attachments Directly to Teeth
The placement of orthodontic attachments (buttons, hooks, and other attachments) directly to the teeth without the necessity of fabricating bands has long been the orthodontist's dream. For the past ten years, the Orthodontic Department at the Bronx-Lebanon Hospital Center has successfully developed and utilized the technique described in this article. It has been used most effectively in the anterior part of the mouth where esthetics is so important, or in specific situations where banding is very difficult or impossible. To date, the adhesive properties of a specific cold-cure acrylic called Pearl-on has been found to be most practical.
Indications
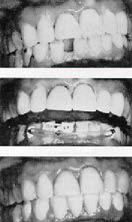
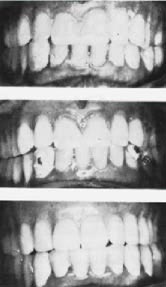
1-- In adult orthodontics preliminary to mouth reconstruction, especially the closing of anterior spaces and improving the axial inclination of the incisors (Figs. 1 & 2).2-- Where teeth cannot be banded easily:
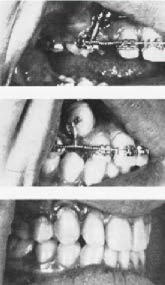
3-- For intrusion, elongation and retrusion of anterior teeth while wearing the face bow appliance; in situations where it is desirable to avoid anterior bands and still maintain adequate control of tooth movement (Figs. 8, 9 & 10).
Technique
applied to the tooth surface with a fine camel-hair brush. After the first thin layer has been exposed to the air for a few seconds, an additional amount of acrylic mix is placed on the same spot.
After treatment is accomplished or normal band placement is made possible, the acrylic base and attachment may be removed by means of a sharp scaler or with an ultrasonic prophylaxis instrument such as Cavitron. No damage has been known to take place on the enamel surface.
Commercially produced plastic brackets have been success fully attached using Pearl-on acrylic as the bonding medium and the attachment has been strong enough to hold light wires, up to .016", for periods up to six months and longer.
Experimental work is now being conducted with an alternate product called Permite A, shade 65. Both products are available through any dental supply house and are manufactured by American Consolidated Manufacturing Co., Inc., Philadelphia, Pa.
Summary and conclusions
By means of the technique described, various attachments may be successfully bonded to teeth by means of Pearl-on cold cure acrylic. The improved esthetics and the simplicity of the procedure make it a useful adjunct in both general and specialty practice. It is a boon to orthodontists in situations where it is not practical to place bands.