CONTROL YOUR PRACTICE
When a patient calls for an appointment it is most important that the person delegated to answer the telephone be trained to obtain the correct initial information and to create a desirable image.
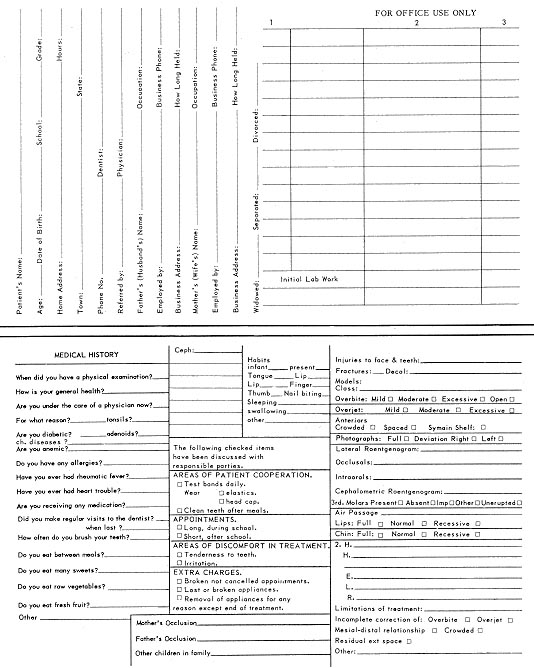
The patient's name, parent's name, address, and telephone number are recorded on a form (Fig. 1) which the parent will later complete. An appointment is made
A letter confirming this appointment is immediately mailed along with some preliminary information about orthodontics and a map indicating the location of my office. This communication gives me an opportunity to further instill my image to the patient and parent. It gives an importance to the appointment. It allows me to begin educating them with the brochure enclosure, I use a reprint of an article which appeared in a lay magazine. I believe that it instills more confidence than information from the orthodontist or from an orthodontic journal. The letter of confirmation is offset printed from my typewriter.
The Patient Arrives
When the patient and parent arrive for the first appointment, I try to see that their first impression is a pleasant one, that the office is calm and pleasant in feeling and appearance, and that an attractive assistant greets them warmly and pleasantly. The parent is given the initial examination card (Fig. 1). At this point we call it an "acquaintance card". The parent is asked to complete the preliminary information on it in the waiting room.
The patient and parent are then ushered into a private office and a short medical history (Fig. 1) is taken by an assistant. It is important that she have a pleasant, informal attitude.
I then come into the office and I am introduced. I take whatever additional professional information I may feel that I need and I try to put the patient at ease. I address myself primarily to the patient. I promise him honesty in telling him what will happen. I describe some of the things that do happen and I invite him to ask questions.
After the confidence of the patient has been gained, we go to the operatory for a thorough initial examination including an oral examination; occlusal, intraoral, lateral, and cephalometric x-rays; frontal and lateral intraoral and extraoral Polaroid photographs; and impressions for study models. The color photographs are invaluable in case presentation and are sometimes useful in the event of differences with the patient concerning pre-existing lesions.
An attempt is made to standardize all the examination techniques to insure ideal routine results. Photos are made in the cephalostat with uniform lighting and a screen as background. Periapical x-rays are taken using a Bard Parker Ortholator to hold the film. These techniques permit a well-trained, supervised assistant to take excellent photographs and x-rays.
Occlusal Film Technique
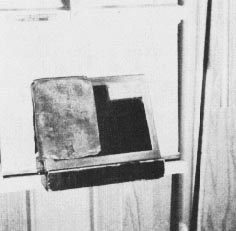
A technique that I use with occlusal film might be of interest (Fig. 2). The film is folded in half and held together With a piece of cellophane tape. Maxillary and mandibular exposures are made in succession without removing the film from the patient's mouth. The double layer of lead foil created by folding the film prevents double exposure. My lateral plates are taken in the cephalostat. I had a piece of 2 x 4 wood slotted to fit onto the ledge of the cephalostat and to hold the cassette at a 60° angle (Fig. 3). This permits routine exact lateral plates.
In taking alginate impressions I find it very helpful to have the patient hold the impression in the mouth. It gives the patient added confidence and prevents gagging.
All films are developed immediately. If retakes should be necessary, they are taken before the patient leaves to prevent later embarrassment.
An appointment is made for the second diagnostic visit and an ADA booklet is given to the parent. This is intended to further educate the parent about orthodontics and prepare the parent for later discussions. A form is now sent to the patient's physician requesting any observations that may be helpful. A like form is sent to the patient's general dentist requesting, in addition, a complete roentgenographic diagnosis. An assistant makes the cephalometric tracing. Study models are completed within 24 hours.
A diagnosis is made and the following information is added to the initial examination card: 1) a diagnosis (Angle classification); 2) prognosis without treatment; 3) treatment plan; 4) prognosis including possible hazards of treatment; 5) cost. The determination of the cost and the manner in which it is paid is of utmost importance from a legal, psychological, and public relations point of view.
Determining a Fee
I divide the treatment into phases and assign a cost to each. A charge is made for initial and final examinations, for all appliances (including a specific cost for various parts such as bands, arches, etc.). A charge is made for the estimated number of visits to be expected for treatment, retention and observation after the completion of treatment. If balancing of the occlusion at the end of treatment is anticipated, a cost is assigned to it. The costs are calculated and the strip of adding machine tape is stapled to the patient's record.
The parent is made aware that this careful figuring has been done and that each anticipated treatment operation has been assigned a fair and reasonable share of the total fee. This is usually done without presenting the actual tape to the parent, although there is nothing wrong with that. This breakdown not only helps me prepare a fee in which I have confidence and in which the parent can have confidence, but has also proven invaluable in transfer cases.
Now the patient and parents arrive for the second visit. On the consultation table are the finished study casts; the patient's intraoral and extraoral photographs mounted in a multiple frame; and the patient's chart which contains the preliminary orthodontic examination material, medical and dental histories, replies from the patient's physician and dentist, my diagnosis and treatment plan, and the fee. On the illuminated view-box are the x-rays, the occlusal film, the lateral jaw plate, the cephalometric film and tracing. (Fig. 4).
I am ready for a thorough discussion of the patient's problems and my recommendations. We realize that orthodontics is not a one-visit affair. It is important for the patient and parents to have a thorough understanding of the problems and the treatment necessary. This may set the pattern for the attitude of the patient and parents throughout treatment. I tell them from my records what the diagnosis means in lay terms. I show them what treatment is necessary to accomplish my goals. I spend time outlining the limitations of treatment and the possible hazards involved. I explain all those factors which will interfere with the success of treatment. In my practice, I find a frank discussion of the problems of treatment enhances my success.
I am now ready to talk about my fee and about methods of payment.
(To be continued next month)