OVERVIEW
Hybrid Aligner Treatment
In this regular column, JCO provides an overview of a clinical topic of interest to orthodontists. Contributions and suggestions for future subjects are welcome.
Hybrid aligner treatment, also known as hybrid mechanics, is the combination of clear aligners with other devices, including fixed appliances, laboratory-fabricated appliances, or auxiliaries. Hybrid aligner treatment utilizes the advantages of removable clear aligners while still accounting for their limitations in producing certain tooth movements.
This overview is intended to evaluate the most popular types of hybrid aligner treatment and to quash the misconception that the planned incorporation of fixed appliances is an indictment of clear aligner therapy.
Fixed Appliances
The most common form of hybrid aligner treatment combines upper clear aligners and lower full-arch labial appliances (Fig. 1). This approach is typically employed in an adult patient with a deep overbite and excessive lower curve of Spee, especially in the presence of preexisting mandibular spacing. Such a patient benefits from a strong reverse-curve archwire throughout treatment to open the bite and intrude the lower incisors, while the upper clear aligners provide the necessary occlusal protection.1

Fig. 1 Lower full-arch labial appliance for use with upper clear aligners.
Clinicians can also use partial appliances with clear aligners in the same arch, as is commonly done when treating mesioangular lower second molars. In this instance, the labial appliances are placed only on the premolars and molars for insertion of a segmental nickel titanium wire, while the terminal end of the clear aligner extends just over the most anterior bracketed tooth (Fig. 2). Most recently, anterior lingual appliances have been used underneath full-arch clear aligners to reinforce their prescribed movements (Fig. 3).2

Fig. 2 Partial labial appliance for molar uprighting after protraction of upper left second and third molars; note that upper clear aligner partially covers upper left second premolar.
Hybrid aligner treatment can also entail placement of upper and lower full-arch or partial labial fixed appliances prior to delivery of the clear aligners (Fig. 4).3
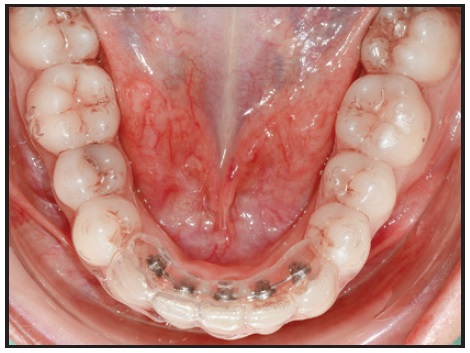
Fig. 3 Lower anterior lingual appliance under overlay clear aligners (photo courtesy of Dr. Luca Lombardo).

Fig. 4 Lower labial appliances placed immediately after lower-incisor extraction; patient transitioned into upper and lower clear aligners after four months.
This technique is usually employed for a few months following premolar or lower-incisor extractions or surgical exposure of impacted teeth.4 The most challenging movements, such as translation into extraction spaces or significant extrusion, are accomplished first with a short phase of fixed appliances, correcting the patient’s malocclusion to the point at which clear aligner treatment is appropriate and predictable results are possible (Fig. 5).

Fig. 5 Extrusion of impacted lower left canine with horizontally beveled attachment and lower full-arch labial appliances; patient transitioned into upper and lower clear aligners after sufficient extrusion.
A variation of this approach involves interim full-arch fixed appliances in one or both arches just prior to orthognathic surgery. In this situation, the patient starts with clear aligners and then transitions into fixed appliances midtreatment. The oral surgeon will thus have traditional fixation options during the surgical procedure, and the orthodontist can quickly move into heavy elastics for settling. If necessary, the patient can transition back into clear aligners three to four months after surgery.5
Some cases might require a short application of fixed appliances at the end of clear aligner treatment for root paralleling or correction of an iatrogenic posterior open bite, which is sometimes created when closing extraction spaces. At other times, it could be necessary to use clear aligners to finish a case that started with fixed appliances for torque control of flared incisors or plunging palatal cusps. The notion of finishing cases with clear aligners has gained momentum as a treatment strategy over the past few years.
Laboratory-Fabricated Appliances
In addition to fixed appliances, hybrid aligner treatment can make use of laboratory-fabricated devices. Banded appliances, such as rapid palatal expanders6; fixed functional appliances, including the Herbst* and the Mandibular Anterior Repositioning Appliance (MARA)**7; and distalizers,3 are typically used just before the delivery of clear aligners as a part of comprehensive treatment for adolescents with skeletal discrepancies. The MARA, for example, offers a more predictable alternative to the Invisalign*** mandibular-advancement feature (Fig. 6).

Fig. 6 Patient with upper clear aligners worn concurrently with Mandibular Anterior Repositioning Appliance (MARA),** which does not have occlusal rests on upper first premolars (lower aligners cannot be used because of holding arch).
The patient should wear vacuformed retainers full-time until the aligners are delivered to minimize any skeletal or dental relapse after removal of the orthopedic appliance. Banded appliances can also be used simultaneously with clear aligners; in this scenario, the aligners should be cut off just mesial to the bands, with attachments placed on the most distal teeth (Fig. 7).
Boneborne expanders and mesializers or distalizers with bondable pads are more commonly used during clear aligner treatment (Fig. 8).8

Fig. 7 Banded Horseshoe Jet‡ used with clear aligners.

Fig. 8 Boneborne expander used with clear aligners.
The most popular distalizers include the Carriere 3D Motion Appliance,†9 the Horseshoe Jet,‡2 and the Beneslider.††10 The Carriere appliance allows for simultaneous clear aligner treatment in the opposing arch; the bondable Horseshoe Jet and the Beneslider can be used in the same arch underneath the clear aligners to assist with movements of the posterior teeth (Fig. 9).
Auxiliaries
Clinicians can also take advantage of auxiliaries, such as miniscrews and bondable buttons, during clear aligner treatment. The use of miniscrew anchorage to extrude impacted upper canines or for intrusion11 (Fig. 10) is a common example.
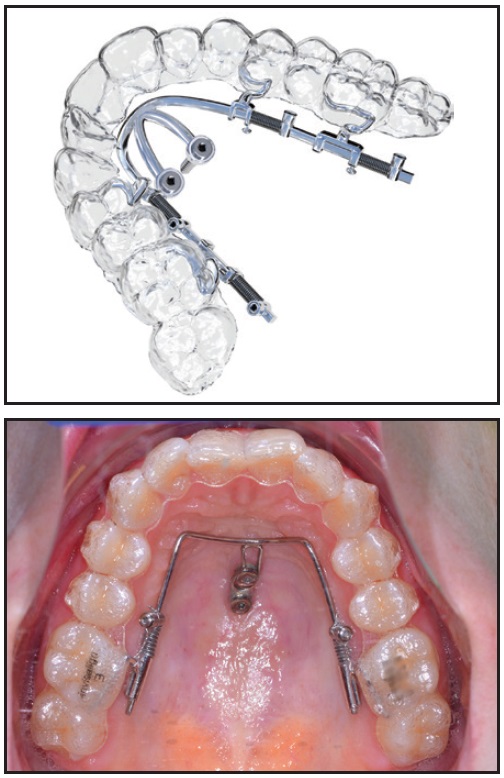
Fig. 9 Beneslider†† with bondable pads used with clear aligners.

Fig. 10 Miniscrews used with clear aligners for posterior intrusion (photos courtesy of Dr. Harry L. Dougherty Jr.).
Buttons with segmental elastic chains can be effective in correcting severely rotated teeth, such as premolars (Fig. 11).2 In virtual treatment planning for such cases, it is important to compensate for undesirable side effects created by the segmental elastic chain on the anchorage teeth.
Discussion
Not all uses of fixed appliances constitute hybrid aligner treatment, which makes it challenging to define this technique. For example, the conversion to fixed appliances after noncompliance, a Phase I expander used years before starting clear aligner treatment, or bonded buttons for attachment of interarch elastics should not be considered hybrid aligner treatment. Our definition implies that the fixed component is a planned part of comprehensive clear aligner treatment, and that it performs skeletal or dental movements that the aligners alone could not predictably achieve.

Fig. 11 Bonded buttons used with segmental elastic chain for derotation of lower left second premolar. Horizontal attachments can be placed on lingual surface of rotated premolar and mesiobuccal surface of first molar; consider compensating for elastic chain by programming slight mesial-out rotation of lower first molar.
Clinical studies from the past 15 years have shown that clear aligners are less predictable for certain types of tooth movements, including lower-incisor intrusion, rotation of canines and premolars, translation into extraction spaces, expansion, and sagittal correction.12-21 The relatively low reliability of these movements has remained consistent, despite advancements in clear aligner technology. Therefore, the main purpose of combining fixed appliances with clear aligner treatment is to mitigate such limitations.
Although esthetic enhancement is the primary advantage of clear aligners, they are also beneficial in patients with oral parafunction, extensive restorative work, poor oral hygiene, predisposition to root resorption, compromised periodontia, complex medical histories, or anterior open bites associated with posterior extrusion. Hybrid mechanics enable the orthodontist to provide a version of clear aligner therapy to all patients—no matter the severity of malocclusion or oral condition.
Even so, critics of clear aligners have suggested that the need to use any form of fixed appliances is an abject failure in treatment. These opinions likely represent pushback against inappropriate corporate marketing and paid speakers, who may have suggested that clear aligners would someday replace labial braces. In fact, the merger of fixed appliances and clear aligners has simply expanded the creativity with which orthodontists can successfully treat a variety of complex malocclusions. That sentiment was perfectly summarized in 2004 by Wheeler: “[Clear aligner therapy] has become a technique that is not limited to delivering aligners. . . . Some patients can be treated with aligners alone, but, in many cases, the aligners must be modified, or used with auxiliaries or fixed appliances as complete or segmented bond ups. . . . We need to keep in perspective that we are all trying to treat to the ‘gold standard’ no matter what technique or appliance system we use.”22
Even 20 years ago, most orthodontists already understood that the incorporation of fixed appliances into clear aligner therapy was not a reflection of the aligners’ ineffectiveness, but merely an innovative use of the clinician’s full armamentarium. Today, the use of planned hybrid aligner treatment has ushered in a new era of modern and esthetic orthodontic solutions. As adolescent and adult consumer demand for clear aligners continues to grow, orthodontists will be increasingly dependent on hybrid treatment to provide these patients with the best possible results.
FOOTNOTES
- *Registered trademark of Dentaurum, Inc., Ispringen, Germany; www.dentaurum.de.
- **AOA Orthodontic Appliances, Sturtevant, WI; www.aoalab.com.
- ***Registered trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
- †Registered trademark of Henry Schein Orthodontics, Melville, NY; www.henryscheinortho.com.
- ‡Specialty Appliances, Inc., Cumming, GA; www.specialtyappliances.com.
- ††PSM North America Inc., Indio, CA; www.psm-na.us.
REFERENCES
- 1. Kravitz, N.D.; Moshiri, M.; Nicozisis, J.; and Miller, S.: Mechanical considerations for deep-bite correction with aligners, Semin. Orthod. 26:134-138, 2020.
- 2. Lombardo, L.; Pepe, F.; Carlucci, A.; and Cremonini, F.: A hybrid approach to clear aligner therapy in lower-incisor extraction cases, J. Clin. Orthod. 55:211-220, 2022.
- 3. Bowman, S.J.; Celenza, F.; Sparaga, J.; Papadopoulos, M.A.; Ojima, K; and Lin, J.C.: Creative adjuncts for clear aligners, Part 1: Class II treatment, J. Clin. Orthod. 49:83-94, 2015.
- 4. Giancotti, A. and Di Girolamo, R.: Treatment of severe maxillary crowding using Invisalign and fixed appliances, J. Clin. Orthod. 43:583-589, 2009.
- 5. Boyd, R.L.: Surgical-orthodontic treatment of two skeletal Class III patients with Invisalign and fixed appliances, J. Clin. Orthod. 39:245-258, 2005.
- 6. Mompell, R. and Bowman, S.J.: Microimplant-assisted aligner therapy, in Temporary Anchorage Devices (TADs) in Contemporary Orthodontics, ed. J.H. Park, Wiley-Blackwell, Hoboken, NJ, 2020, pp. 567-580.
- 7. Eckhart, J.E.: Sequential MARA-Invisalign treatment, J. Clin. Orthod. 43:439-448, 2009.
- 8. Wilmes, B.; Schwarze, J.; Vasudavan, S.; and Drescher, D.: Maxillary space closure using aligners and palatal mini-implants in patients with congenitally missing lateral incisors, J. Clin. Orthod. 55:20-33, 2021.
- 9. Lombardo, L.; Cremonini, F.; Oliverio, T.; Cervinara, F.; and Siciliani, G.: Class II correction with Carriere Motion 3D Appliance and clear aligner therapy, J. Clin. Orthod. 56:187-193, 2022.
- 10. Wilmes, B.; Schwarze, J.; Vasudavan, S.; and Drescher, D.: Combination of clear aligners and Beneslider for correction of severe midline deviation, J. Clin. Orthod. 55:675-683, 2021.
- 11. Bowman, S.J.; Celenza, F.; Sparaga, J.; Papadopoulos, M.A.; Ojima, K.; and Lin, J.C.: Creative adjuncts for clear aligners, Part 2: Intrusion, rotation, and extrusion, J. Clin. Orthod. 49:162-172, 2015.
- 12. Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; and Makki, L.: Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign, Am. J. Orthod. 158:420-425, 2020.
- 13. Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; and Agran, B.: How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign, Am. J. Orthod. 135:27-35, 2009.
- 14. Blundell, H.L.; Weir, T.; Kerr, B.; and Freer, E.: Predictability of overbite control with the Invisalign appliance, Am. J. Orthod. 160:725-731, 2021.
- 15. Charalampakis, O.; Iliadi, A.; Ueno, H.; Oliver, D.R.; and Kim, K.B.: Accuracy of clear aligners: A retrospective study of patients who needed refinement, Am. J. Orthod. 154:47-54, 2018.
- 16. Kravitz, N.D.; Kusnoto, B.; Agran, B.; and Viana, G.: Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign: A prospective clinical study, Angle Orthod. 78:682-687, 2008.
- 17. Grünheid, T.; Loh, C.; and Larson, B.E.: How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 87:809-815, 2017.
- 18. Tien, R.; Patel, V.; Chen, T.; Lavrin, I.; Naoum, S.; Lee, R.J.H.; and Goonewardene, M.S.: The predictability of expansion with Invisalign: A retrospective cohort study, Am. J. Orthod. 163:47-53, 2023.
- 19. Dai, F.F.; Xu, T.M.; and Shu, G.: Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign, Angle Orthod. 89:679-687, 2019.
- 20. Patterson, B.D.; Foley, P.F.; Ueno, H.; Mason, S.A.; Schneider, P.P.; and Kim, K.B.: Class II malocclusion correction with Invisalign: Is it possible? Am. J. Orthod. 159:e41-e48, 2021.
- 21. Kravitz, N.D.; Dalloul, B.; Zaid, Y.A.; Shah, C.; and Vaid, N.R.: What percentage of patients switch from Invisalign to braces? A retrospective study evaluating the conversion rate, number of refinement scans, and length of treatment, Am. J. Orthod. 18:S0889-5406(22)00773-9, 2022.
- 23. Wheeler, T.T.: Invisalign material studies, Am. J. Orthod. 125:19A, 2004.
-
 DR. KRAVITZ
DR. KRAVITZ -
 DR. MILLER
DR. MILLER -
 DR. BOWMAN
DR. BOWMAN -
 DR. WILMES
DR. WILMES
Dr. Kravitz is the Editor-in-Chief of the Journal of Clinical Orthodontics and in the private practice of orthodontics, 25055 Riding Plaza, Suite 110, South Riding, VA 20152; e-mail: nealkravitz@gmail.com. Dr. Miller is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics in Orange, CA. Dr. Bowman is a Contributing Editor of the Journal of Clinical Orthodontics; an Adjunct Associate Professor, St. Louis University, St. Louis; Assistant Clinical Professor, Case Western Reserve University, Cleveland; Instructor, University of Michigan, Ann Arbor, MI; and in the private practice of orthodontics in Portage, MI. Dr. Wilmes is a Professor, Department of Orthodontics, University of Düsseldorf, Düsseldorf, Germany.

COMMENTS
.