Creative Adjuncts for Clear Aligners, Part 1: Class II Treatment
Clear aligners have been increasingly utilized by orthodontists in recent years. Originally directed toward the correction of mild orthodontic problems in adults,1-5 this approach became more challenging when applied to complex anteroposterior discrepancies and orthodontic movements such as intrusion of posterior teeth, extrusion of anterior teeth, and torquing.4,6,7 Specifically, clinicians encountered difficulties with bodily movement of teeth,3 especially after the extraction of four premolars in a situation requiring maximum anchorage.
Obviously, successful treatment with clear aligners involves much more than moving virtual teeth in a software program and dispensing plastic to patients.8-10 The application of adjunctive biomechanics through the addition of orthodontic elastics, springs, and other devices has certainly created more individualized options for predictable tooth movement across a wider range of malocclusions. Miniscrew implants, which have been effective in supporting anchorage for orthodontic tooth movement,11 are now being used as adjuncts to clear-aligner treatment as well.
The present three-part article describes a variety of treatment methods that can expand the clinical applications and improve the predictability of clear aligners. This month, we discuss several options for Class II treatment. Parts 2 and 3 will illustrate a variety of tooth movements. It should be noted that success in any of the case types presented here will depend on proper diagnosis, detailed treatment planning, and, most important, patient compliance.
Class II Treatment with Simple Aligner Adjuncts
At the dawn of sequential clear-aligner treatment, no substantial thought was given to the mechanics that would be required to address Class II or III malocclusions, leading to the widespread belief that "buccal malocclusions" were contraindications.2,6,12 During the ensuing 15 years, however, a number of methods have been proposed to treat both growing13 and adult Class II cases with aligners. The application of elastics to bonded buttons, brackets, or notches cut into the aligner material was an obvious first step.8 More recent adjuncts have included fixed functional appliances,14 molar distalizers,15 and miniscrew anchorage.16
Similar articles from the archive:
- Effectiveness of Composite Attachments in Controlling Upper-Molar Movement with Aligners June 2016
- Attachment of Intermaxillary Elastics to Thermoformed Aligners January 2009
- A Three-Dimensional Finite Element Analysis of Upper-Canine Distalization with Clear Aligners, Composite Attachments, and Class II Elastics January 2017
In a mild Class II or pseudo-Class I case, maxillary molar rotation with aligners may suffice to at least improve the molar relationship.17 With any tooth movement, however, there is a price to be paid in loss of anchorage. That axiom was "rediscovered" during initial attempts at molar distalization with aligners alone. A Class II case usually involves a struggle between the anchorage control needed to avoid iatrogenic mesial movement of lower anterior teeth and the patient compliance required to achieve that control.
The application of Class II intermaxillary elastics to clear aligners adds a further compliance burden.18 Since Class II correction in a growing patient is derived primarily from the interruption of dentoalveolar compensation (whether from headgear, elastics, functional appliances, or distalization), sequential molar distalization supported by elastics, as advocated by Daher,19 is a logical strategy that has proven successful with aligners (Fig. 1 AB, C).20

Fig. 1 Molar distalization supported by elastics. A. 13-year-old female patient with Class II, division 1 malocclusion and moderate overbite before treatment. Invisalign TEEN* treatment involved sequential upper-molar distalization and subsequent retraction of remaining teeth. B. Class II elastics hooked from notches in aligners mesial to upper canines and extended to bonded buttons on lower molars (continued in next image).

Fig. 1 (cont.) C. Mild overcorrection to super-Class I achieved in 17 months, including one refinement.
In an adult patient, on the other hand, Class II correction comes primarily from tooth movement without the benefits of growth; therefore, more anchorage control is required. Miniscrew anchorage fills that bill quite nicely. In a typical case, an adult male with the chief complaint of a "snaggle tooth" presented with a unilateral Class II malocclusion and significant anterior crowding (Fig. 2).

Fig. 2 Class II unilateral en masse retraction supported by miniscrew anchorage. A. Adult male patient with anterior crowding and unilateral Class II malocclusion before treatment. B. Closed-coil retraction spring extended from miniscrew in palatal alveolus between upper left molars to improvised “power arm” bonded to palatal surface of first premolar for en masse quadrant retraction guided by Invisalign tray.21 C. Original power arm later replaced with tomas** bonded aligner hook. D. Patient after 18 months of treatment, using 52 aligner pairs and two refinements.
Although distal movement of the upper left posterior quadrant was needed, anchorage control was a concern. To improve the predictability of the aligners' distal drive, a miniscrew was inserted into the palatal alveolus between the roots of the left first and second molars.21 A nickel titanium closed-coil spring was extended anteriorly from the miniscrew to a "power arm" bonded to the palatal surface of the first premolar, obviating the need for Class II elastics. The advantages of placing miniscrews in the palate include a substantially lower failure rate, the availability of larger interradicular spaces than on the buccal, and the ability to apply forces closer to the center of resistance, thus avoiding unwanted tipping. Mesially beveled attachments were also placed on the premolars to improve tracking during distalization. The clear aligners' primary task in this scenario was to guide and contain the selected teeth during the programmed retraction. A substantial improvement in the posterior occlusion and anterior esthetics was achieved in 18 months of treatment without elastics, using 52 aligner pairs (including two refinements).
Miniscrew anchorage has also been used to provide simple "posts" for the patient's attachment of either intermaxillary or intramaxillary elastics to bonded buttons, hooks, or simple notches cut into the aligners themselves.16,22 For example, a young adult female with a unilateral Class II malocclusion, generalized maxillary spacing, and moderate overjet exhibited significant anchorage issues (Fig. 3).
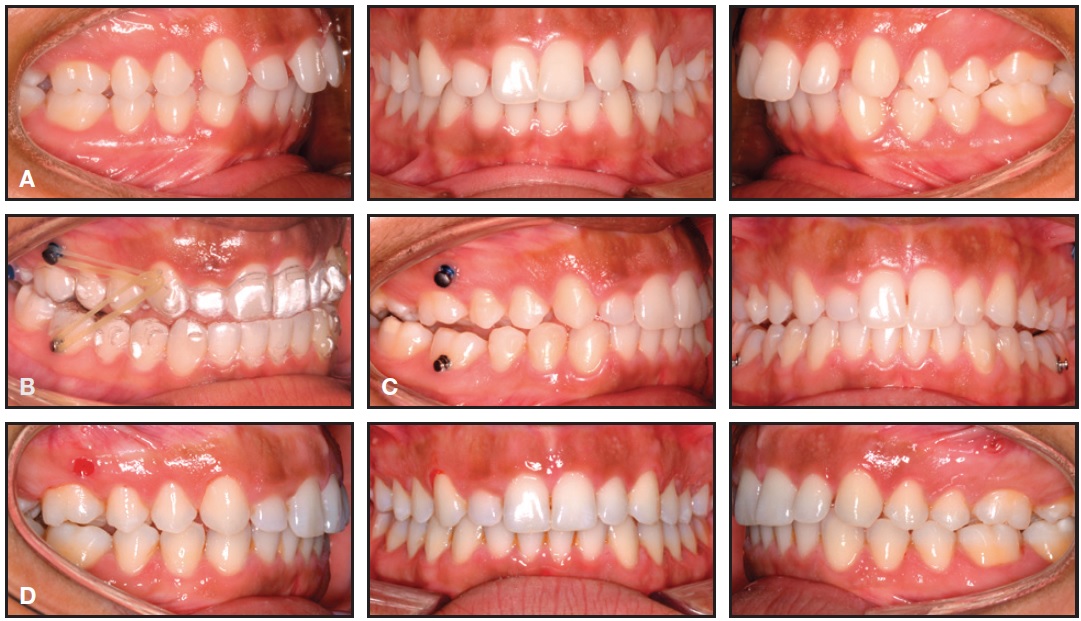
Fig. 3 Class II en masse retraction supported by miniscrew anchorage and elastics. A. 18-year-old female patient with unilateral Class II malocclusion, generalized maxillary spacing, and moderate overjet before treatment. B. Miniscrews inserted bilaterally between roots of upper first molars and second premolars. Class I elastics attached from miniscrews to notches in Invisalign tray mesial to upper canines; Class II elastics attached from maxillary tray notches to bonded buttons on lower first molars. Lingual root torque applied to upper anterior teeth by torque ridges. C. After one year of treatment, patient shows improvement toward Class I, but refinement with posterior buccal root torque and leveling of lower curve of Spee will be required to seat occlusion. D. Refinement aligners with additional intermaxillary elastic wear still required.
While Class II elastics would certainly be required during the Invisalign* treatment to assist in space closure, upper-molar distalization was also needed to correct the Class II malocclusion. Miniscrews were inserted into the buccal alveolus between the roots of the upper first molars and second premolars. Class I intramaxillary elastics were prescribed as a "headgear substitute"; combined with Class II elastics, they produced a net force vector that drove the maxillary dentition distally. Because some space closure was also desired from protraction of the lower posterior teeth, the anchorage loss in the mandibular arch as a result of the Class II elastics was not a major concern. What was disconcerting was a lack of patient compliance, which resulted in unacceptable tracking of the anterior teeth and inadequate upper lingual root torque.
The attachment of orthodontic elastics to clear aligners is simplified by bonding buttons, hooks, or brackets to selected teeth. Sections of the aligner plastic must be removed to seat the aligners over these adjuncts. This can easily be accomplished with the Hole Punch*** plier, designed to punch out a half-circle at the gingival margin of each tray in a series (Fig. 4A). The Tear Drop plier is then used to cut a teardrop shape along the gingival margin of the aligner, creating a "hook"for the application of elastics (Fig. 4B).
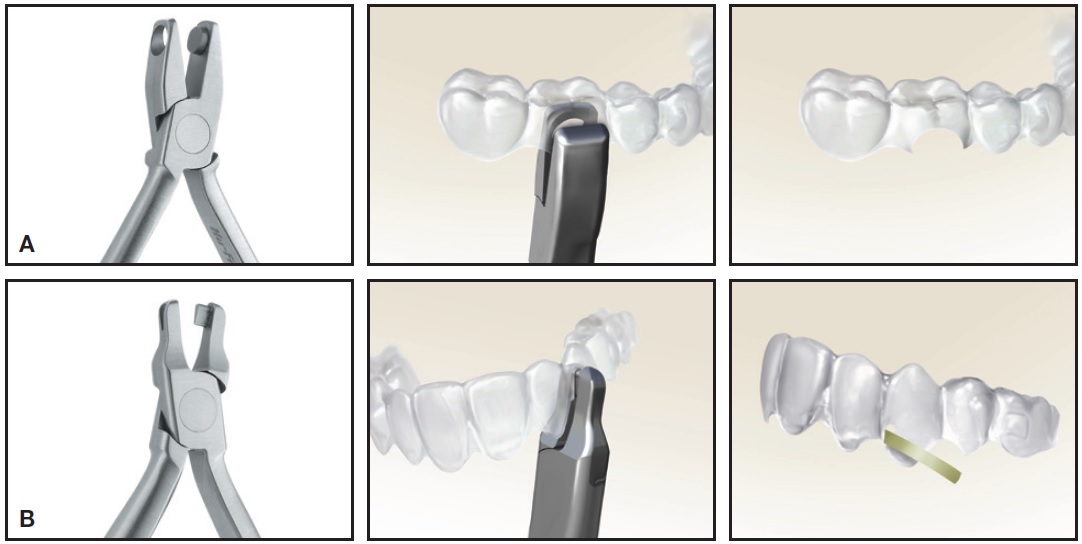
Fig. 4 A. Hole Punch*** plier cuts half-moon shape into aligner plastic to provide relief for bonded button. B. Tear Drop*** plier cuts teardrop-shaped notch at gingival margin of aligner, providing reservoir that makes application of elastics easier for patient. (Photos courtesy of Hu-Friedy Manufacturing Co., Chicago.)
Molar Distalization Prior to Aligner Treatment
Concerns about the predictability of Class II correction with only elastic support have prompted orthodontists to consider aligner treatment as a follow-up to molar distalization, much as they would use fixed appliances for finishing. One such method involves the Carriere Distalizer†, which is bonded to the upper molars and canines of one or both sides as needed.23,24 Class II elastics are attached between hooks on the canine and the lower first molar to produce molar rotation and distalization of the buccal segment. The Distalizer is then removed, and impressions or digital scans are taken for clear-aligner treatment.15 A retainer should be inserted immediately to prevent any mesial rebound of the distalized teeth during the time needed for laboratory fabrication of the aligners.
Because the Carriere Distalizer is visible at the upper canine and typically creates a space be tween the upper canine and lateral incisor, its esthetic appearance should be discussed with the patient, along with the absolute necessity of compliance with elastic wear. In addition, Class II elastics will tax mandibular anchorage, which can be enhanced with the use of lower brackets, lingual arches, full-coverage plastic retainers, or even concurrent lower aligner treatment.15,18,23,24
The compliance and anchorage issues have typically limited this approach to milder Class II and pseudo-Class I patients. In a more severe Class II case, skeletal anchorage can be employed by inserting a miniscrew between the roots of the upper first molar and second premolar (Fig. 5).

Fig. 5 Pre-aligner distalization with miniscrew-supported Carriere Distalizer.† A. Adult female patient with unilateral Class II, division 2 malocclusion before treatment. B. Miniscrew inserted between roots of upper right first molar and second premolar. Elastic chain attached between mesial Distalizer hook and miniscrew; Class II elastics hooked to lower lingual holding arch. C. Improvement in upper right quadrant results in space between canine and lateral incisor after five months, just prior to start of Invisalign treatment. D. Same supporting elastics connected from notch in aligner mesial to upper canine for support during space closure and torque expression during anticipated 16 months of aligner treatment.
Elastic chain is then applied from the miniscrew "post" to the canine hook of the Distalizer, applying a constant retraction force even if Class II elastics are not worn. In any event, it is important to continue to prescribe Class II elastics during clearaligner treatment to support anchorage during retraction of the remaining maxillary teeth and thus avoid unintended loss of any distalization that has been achieved.
Another option for accomplishing molar distalization as a precursor to aligner treatment is to use a stand-alone appliance such as the Pendulum‡25 or Distal Jet††.26 Although these devices require no patient compliance and are relatively esthetic (being inserted in the palate), some attendant maxillary anterior anchorage loss is possible. Miniscrew anchorage has substantially improved the predictability of these appliances in delivering the desired molar corrections. Indeed, the Horseshoe Jet‡‡, a skeletonized modification of the Distal Jet, was designed to be supported by miniscrew anchorage, thereby avoiding anterior anchorage loss.22,26-29 Miniscrews are inserted in the palatal alveolus between the roots of the first molar and second premolar (generally the largest available interradicular space) or in the anterior palate. Stainless steel ligatures are tied from the miniscrews to hooks on the anterior portion of the Ushaped wire framework to support distalization forces from compressed-coil springs. The molars are distalized--and the premolars follow due to forces from the transseptal fibers--into super-Class I or partial Class III positions within six to eight months (Fig. 6 AB, C-E).
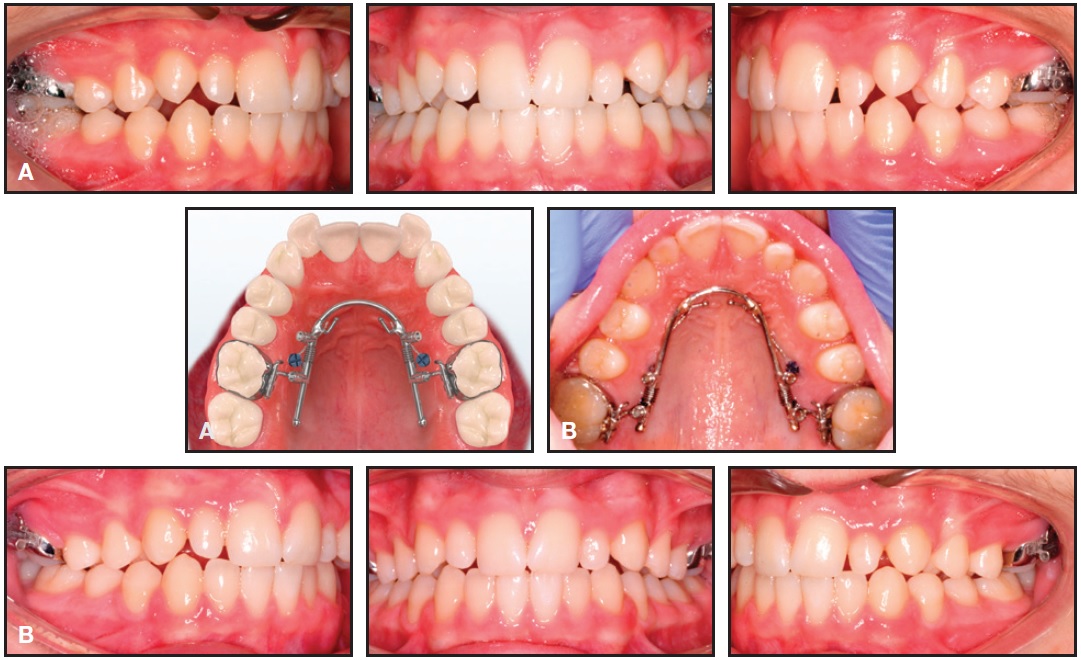
Fig. 6 Pre-aligner distalization with miniscrew-supported Horseshoe Jet.‡‡ A. 14-year-old male patient with half-step Class II malocclusion treated initially with upper-molar distalization, using Horseshoe Jet supported by two miniscrews in palatal alveolus between first molars and second premolars. B. After seven months, super-Class I molar relationships achieved without any anchorage loss or compliance requirements (continued in next image).

Fig. 6 (cont.) C. Horseshoe Jet removed, but miniscrews left in place in case of future need for retraction support. D. Invisalign trays in place with Class II elastics. E. Retraction of remaining maxillary teeth nearly complete after one year of aligner treatment. (Photo of appliance courtesy of IACT, Birmingham, AL.)
Three options are then available for subsequent clear-aligner treatment:
- The Horseshoe Jet is removed, and Class II elastics are used to support aligner retraction of the remaining maxillary teeth (see Fig. 1 AB, C). In this scenario, it is imperative that a clear retainer be delivered immediately after removal of the Horseshoe Jet to prevent any mesial relapse of the molars while awaiting aligner fabrication.
- The Horseshoe Jet is removed, and aligner retraction is then supported by coil springs or elastics from the palatal miniscrews to bonded hooks on the palatal surfaces of the first premolars or canines (see Fig. 2).
- The Horseshoe Jet is "locked" and left in place to hold the molars in position. To support retraction of the remaining teeth, aligners are designed with the plastic ending at the second premolars, and Class I intramaxillary elastics are worn from the first-molar hooks to notches cut into the aligners mesial to the canines. After retraction is complete, the Horseshoe is removed and refinement aligners are designed to incorporate all teeth for finishing.
Another option is to correct the Class II and other less predictable aspects of the malocclusion using fixed appliances in a short phase of treatment prior to clear aligners. We conducted a combined clinical evaluation of two products--Insignia‡30 brackets and Invisalign--in an adult male patient with a unilateral Class II malocclusion and dental crowding (Fig. 7 AB, CD).
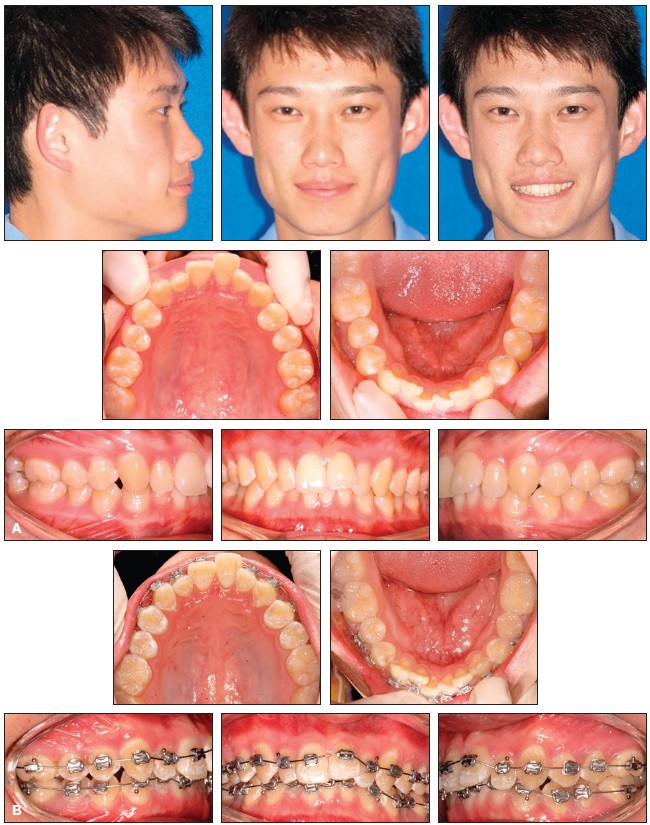
Fig. 7 Pre-aligner distalization with miniscrew-supported Insignia‡ fixed appliances. A. Adult male patient with unilateral right Class II malocclusion and significant dental crowding and protrusion before treatment. B. Customized Insignia brackets combined with miniscrew anchorage for en masse retraction of upper right posterior segment (continued in next image).
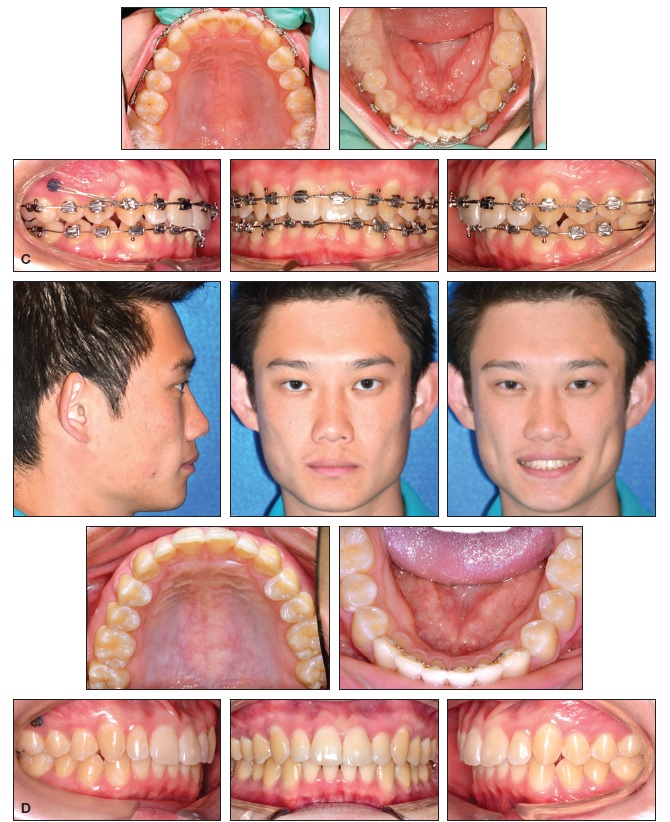
Fig. 7 (cont.) C. Reasonable alignment and Class I molar relationship achieved after seven months. D. Treatment completed in additional 17 months with Invisalign and continued Class I elastic support from miniscrew.
The brackets were custom-designed with built-in overcorrection to address the most difficult aspects of the patient's malocclusion over a seven-month period. Distal en masse retraction, supported by a miniscrew, improved the Class II relationship and maxillary crowding. Fixed appliances were then removed, and clearaligner treatment was initiated with Class I intramaxillary elastics worn from the miniscrew to notches cut into the upper aligner trays, thus maintaining the retraction during the remaining 17 months of treatment.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., Santa Clara, CA; www.aligntech.com.
- **Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- ***Clear Collection, Hu-Friedy Manufacturing Co., Chicago, IL; www.hu-friedy.com
- †Registered trademark of Henry Schein, Melville, NY; www.henryschein.com.
- ‡Ormco Corporation, Orange, CA; www.ormco.com.
- ††American Orthodontics, Sheboygan, WI; www.americanortho.com.
- ‡‡AOA Orthodontic Appliances, Sturtevant, WI; www.aoalab.com.
REFERENCES
- 1. Boyd, R.L.; Miller, R.J.; and Vlaskalic, V.: The Invisalign system in adult orthodontics: Mild crowding and space closure cases, J. Clin. Orthod. 34:203-212, 2000.
- 2. Vlaskalic, V. and Boyd, R.: Orthodontic treatment of a mildly crowded malocclusion using Invisalign system, Austral. Orthod. J. 17:41-46, 2002
- 3. Bollen, A.M.; Huang, G.; King, G.; Hujoel, P.; and Ma, T.: Activation time and material stiffness of sequential removable orthodontic appliances, Part 1: Ability to complete treatment, Am. J. Orthod. 124:496-501, 2003.
- 4. Clements, K.M.; Bollen, A.M.; Huang, G.; King, G.; Hujoel, P.; and Ma, T.: Activation time and material stiffness of sequential removable orthodontic appliances, Part 2: Dental improvements, Am. J. Orthod. 124:502-508, 2003.
- 5. Joffe, L.: Invisalign: Early experiences, J. Orthod. 30:348-352, 2003.
- 6. Djeu, G.; Shelton, C.; and Maganzini, A.: Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system, Am. J. Orthod. 128:292-298, 2005.
- 7. Phan, X. and Ling, P.H.: Clinical limitations of Invisalign, J. Can. Dent. Assoc. 73:263-266, 2007.
- 8. Tuncay, O.: The Invisalign System, Quintessence, London, 2007.
- 9. Boyd, R.L.: Complex orthodontic treatment using a new protocol for the Invisalign appliance, J. Clin Orthod. 42:525-547, 2007
- 10. Boyd, R.L.: Esthetic orthodontic treatment using the Invisalign appliance for moderate to complex malocclusions, J. Dent. Ed. 72:948-967, 2008.
- 11. Papadopoulos, M.A.; Papageorgiou, S.N.; and Zogakis, I.P.: Clinical effectiveness of orthodontic miniscrew implants: A meta-analysis, J. Dent. Res. 90:969-976, 2011.
- 12. Kamatovic, M.: A retrospective evaluation of the effectiveness of the Invisalign appliance using the PAR and irregularity indices, doctoral dissertation, University of Toronto, Toronto, Ontario, 2004.
- 13. Tuncay, O.; Bowman, S.J.; Amy, B.; and Nicozisis, J.: Aligner treatment in the teenage patient, J. Clin. Orthod. 47:115-119, 2013.
- 14. Eckhart, J.E.: Sequential MARA-Invisalign treatment, J. Clin. Orthod. 43:439-448, 2009.
- 15. Colville, C.D.: Carrière distalizer and Invisalign combo for Class II treatment, Invisalign Insights, Sept. 2012, www.aligntechinstitute.com.
- 16. Paquette, D.: Temporary anchorage devices in combination with aligners, Nov. 2009, www.aligntechinstitute.com.
- 17. Fischer, K.: Invisalign treatment of dental Class II malocclusions without auxiliaries, J. Clin. Orthod. 44:665-672, 2010.
- 18. Schupp, W.; Haubrich, J.; and Neumann, I.: Class II correction with the Invisalign system, J. Clin. Orthod. 44:28-35, 2010.
- 19. Daher, S.: Dr. Sam Daher’s techniques for Class II correction with Invisalign and elastics, Align Technology, Santa Clara, CA, 2011 [cited July 1, 2013], s3.amazonaws.com/learninvisalign/docs/06840000000GHgmAAG.pdf.
- 20. Klein, B.M.: A cephalometric study of adult mild Class II nonextraction treatment with the Invisalign System, master’s thesis, Center for Advanced Dental Education, St. Louis University, St. Louis, 2003.
- 21. Celenza, F.: Clear aligner therapy/distalizing molars, in TAD Clinical Reference Guide, version 3, ed. S. Baumgaertel, Dentaurum, Newtown, PA, 2011.
- 22. Bowman, S.J.: Thinking outside the box with miniscrews, in Microimplants as Temporary Anchorage in Orthodontics, ed. J.A. McNamara Jr. and K.A. Ribbens, Craniofacial Growth Series, University of Michigan, Ann Arbor, 45:327-390, 2008.
- 23. Carrière, L.A.: A new Class II distalizer, J. Clin. Orthod. 38:224-231, 2004.
- 24. Sandifer, C.L.; English, J.D.; Colville, C.D.; Gallerano, R.L.; and Akyalcin, S.: Treatment effects of the Carrière distalizer using lingual arch and full fixed appliances, J. World Fed. Orthod. 3:e49-e54, 2014.
- 25. Hilgers, J.J.: The Pendulum appliance for Class II non-compliance therapy, J. Clin. Orthod. 26:706-714, 1992.
- 26. Bowman, S.J.: Class II combination therapy: Molar distalization and fixed functionals, in Current Therapy in Orthodontics, ed. R. Nanda and S. Kapila, Mosby Elsevier, St. Louis, 2009, pp. 115-136.
- 27. Ludwig, B.; Baumgaertel, S.; and Bowman, S.J.: Mini-Implants in Orthodontics: Innovative Anchorage Concepts, Quintessence, Chicago, 2008.
- 28. Bowman, S.J.: Settling the score with Class IIs using miniscrews, in Temporary Skeletal Anchorage Devices: A Guide to Design and Evidence-Based Solutions, ed. K.B. Kim, Springer-Verlag, Berlin, 2014.
- 29. Bowman, S.J.: The evolution of the Horseshoe Jet, in Skeletal Anchorage in Orthodontic Treatment of Class II Malocclusion: Contemporary Applications of Orthodontic Implants, Miniscrew Implants and Miniplates, ed. M.A. Papadopoulos, Mosby Elsevier, St. Louis, 2015.
- 30. Gracco, A. and Tracey, S.: The Insignia system of customized orthodontics, J. Clin. Orthod. 45:442-451, 2011.
-
 DR. BOWMAN
DR. BOWMAN -
 DR. CELENZA
DR. CELENZA -
DR. SPARAGA
-
DR. PAPADOPOULOS
-
DR. OJIMA
-
DR. LIN
Dr. Bowman is a Contributing Editor of the Journal of Clinical Orthodontics; an Adjunct Associate Professor, St. Louis University, St. Louis; a straight-wire instructor, University of Michigan, Ann Arbor, MI; an Assistant Clinical Professor, Case Western Reserve University, Cleveland; a Visiting Clinical Lecturer, Seton Hill University, Greensburg, PA; and in the private practice of orthodontics at 1314 W. Milham Ave., Portage, MI 49024; Drs. Celenza, Sparaga, and Ojima are in the private practice of orthodontics in New York City; Anchorage, AK; and Tokyo, respectively. Dr. Papadopoulos is Professor and Program Director, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece. Dr. Lin is Clinical Assistant Professor, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, National Defense Medical University, Taipei, Taiwan, and in the private practice of orthodontics and implantology in Taipei. Dr. Bowman is inventor of the Clear Collection pliers. E-mail him at drjwyred@aol.com.