The Transition from Standard Edgewise to Preadjusted Appliance Systems
By the 1950s, both Begg and edgewise practitioners were beginning to consider ways to achieve high-quality results with less wire bending and simplified mechanics.1 Andrew's study of nonorthodontic normal models during the 1960s led to the development of his six keys to occlusion and average values for thickness, tip, and torque of clinical crowns.2 The Andrews Straight-Wire Appliance, introduced commercially in the early 1970s, was the result.
This preadjusted, preangulated appliance was based on the concept that in an ideal gnathological setup for a given patient, the bracket bases would accurately fit each tooth at a predetermined point, and the bracket slots would passively accept a straight wire coordinated to the patient's arch form. By 1986, preadjusted appliance systems in general were reportedly used twice as much as any other system by U.S. orthodontists.3
This article examines the most significant changes in mechanics that occurred during the transition period from standard edgewise to preadjusted appliance systems, particularly in extraction treatment. The changes are grouped under the six sequential but overlapping phases of most orthodontic treatment: anchorage control, leveling and aligning, overbite control, overjet reduction, space closure, and finishing.
Anchorage Control
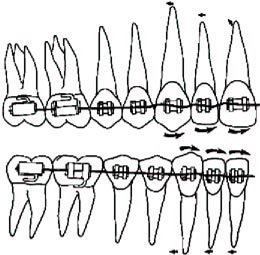
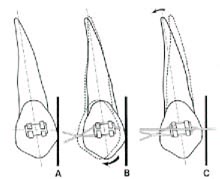
When archwires were first placed in patients with preadjusted appliances, the tip built into the anterior brackets increased the tendency for the incisors and cuspids to tip forward (Fig. 1). This tendency was greater in the upper arch than in the lower because of the greater amount of tip in the upper anterior brackets.
Many orthodontists began to complain that these appliances "burned anchorage", and some returned to the more familiar standard edgewise appliance. Andrews, however, contended that most cases were 20% undertreated compared to the nonorthodontic normal models, and that if teeth were positioned according to the six keys, the same amount of total anchorage control would be required under any fixed appliance system.4
We agree with Andrews as far as the overall treatment is concerned. Still, we found that if the greater anchorage requirements at the beginning of the case were attended to and the crowns and roots were brought into their proper positions, then anchorage needs toward the end of the case were frequently diminished.
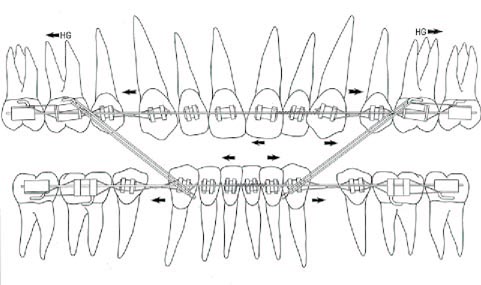
As orthodontists began to appreciate this need for early anchorage control, some incorporated the edgewise principle of omega-loop stops and molar tiebacks to control incisor and cuspid positions. Upper molars were supported with palatal bars and headgears, and lower molars with lingual arches and, indirectly, with Class III elastics. We prefer not to use omega loops to control anterior tooth positions, but instead bend back the archwires immediately behind the most distally banded molars.
Leveling and Aligning
Two significant factors became apparent after preadjusted appliances had been in use for some time. First was the result of overcompensation for the anchorage control problem. In an attempt to prevent anterior teeth from tipping forward during the initial stages, elastic forces such as chains, modules, and inter- or intra-arch elastics were often applied prematurely between the anterior and posterior teeth, so that the anterior crowns were not merely held in position, but actually tipped distally.
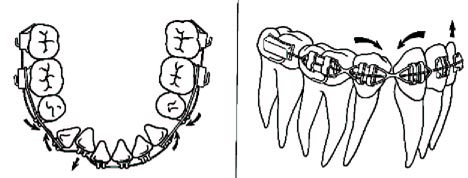
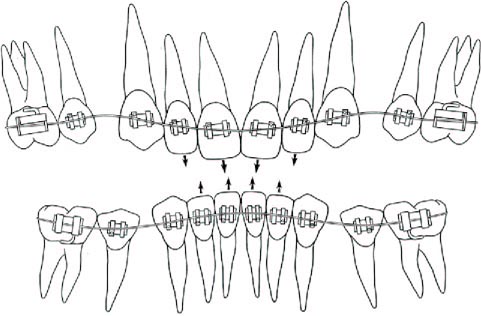
This problem was not as severe in nonextraction cases, because the amount of tipping was usually restricted by the limited space in the arch. However, in extraction cases the cuspids became the focus of attention because of the need to prevent their mesial tipping, as well as to begin retracting them into the extraction sites. The premature application of elastic tension caused the cuspids to tip distally, which in turn opened the bite in the premolar area and deepened the bite anteriorly (Fig. 2). This situation could normally be corrected, but it did result in a longer leveling stage and usually an extended total treatment.
The second factor was related to compensation for this cuspid tipping, as well as to a need for overcorrection during tooth movement and at the end of treatment. With standard edgewise mechanics--particularly the Tweed technique5--compensation and overcorrection were handled by varying the amounts of 1st-, 2nd-, and 3rd-order bends. To minimize such bends, Andrews developed two additional sets of incisor brackets with modified torque for either extraction or nonextraction cases.6 He also designed a series of extraction brackets for cuspids and posterior teeth, to be used according to the demands of the case. He provided hooks (which he called "power arms") for these extraction brackets so that forces could be applied closer to the center of rotation of each tooth.
Roth, who worked extensively with the appliance, saw a similar need for compensation and overcorrection, but wanted to overcome the inventory problem of multiple appliance prescriptions.7 He developed his own prescription, which he recommends for both extraction and nonextraction cases. A number of other angulation options are now available, and the orthodontist can essentially select an appliance of choice for any given treatment.
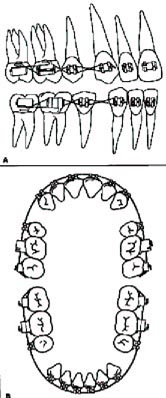
We observed that no matter which prescription was used, adverse tipping occurred in the early leveling stages if elastic forces (even very light forces) were applied to the cuspids. We instead place figure-8 .010'' ligature wires (called "lacebacks") from the most distally banded molar to the cuspid in each quadrant (Fig. 3A). The archwire is also bent back behind the most distally banded molar to minimize the forward movement of the incisors (Fig. 3B). We maintain molar anchorage as described above.
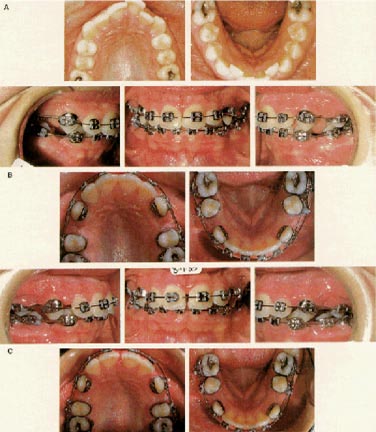
These methods, which are certainly not new to orthodontics, can be used in any case where forward tipping of cuspid crowns would be undesirable. They are most advantageous in extraction cases, in which they can provide surprisingly efficient distal cuspid movement (Fig. 4).
The figure-8 ligatures, when lightly and passively secured, initially cause a slight tipping of the cuspids with compression of the periodontal ligament in the area of the alveolar crest. However, because there is no elastic tension on the teeth, the cuspid roots have more than enough "rebound time" to upright into correct position as the main archwire takes effect (Fig. 5).
This theoretical explanation is supported by the clinical finding that when a patient returns for routine adjustments, the lacebacks are consistently loose and need minimal tightening. It is possible that the patient's tongue or food particles contacting the lacebacks could cause additional minor tipping, but these are intermittent forces that would still allow adequate rebound time.
Our technique provides 6-7mm of space opening in the anterior segments over six months, while leveling proceeds from light, multistranded wires into .020" round wires. If this space is more than desired (as in an uncrowded bimaxillary protrusion case), the lacebacks are discontinued before leveling is completed.
If the case has more than 6-7mm of crowding, the most crowded teeth are not bracketed, and light push-coil springs are inserted to provide additional space (Fig. 6). These springs are normally not used until .016" or .018" round archwires are in place; their forward tipping effect can be counteracted with the anchorage control methods listed above.
Overbite Control and Overjet Reduction
The first noticeable difference in overbite control with preadjusted appliances was again a result of the tip placed into the cuspid brackets. Cuspids frequently erupted into a more upright position than would be desirable, so the mesial aspect of the cuspid bracket slot would initially be placed more incisally than the distal aspect of the slot. The initial archwire would then have to be extended gingivally to enter the slot, creating an extrusive effect on the incisors and in turn deepening the overbite (Fig. 7).
When the cuspids are upright or even more distally inclined (fortunately not very often), the most effective way to manage this situation is to leave the incisors unbracketed, place lacebacks to the cuspids, and wait for the cuspid roots to distalize and the cuspid slots to become more parallel to the occlusal plane.
Another difficulty was a byproduct of the elastic force effect discussed in the leveling and aligning phase. When elastic forces were placed against the cuspids early in treatment, the cuspid crowns tipped distally, causing the mesial aspects of the cuspid bracket slots to move incisally (Fig. 3). This in turn caused the incisors to extrude and the overbite to deepen. The effect is not as great with the limited space available for distal tipping in a nonextraction case. As described above, the distal tipping can be ameliorated using lacebacks.
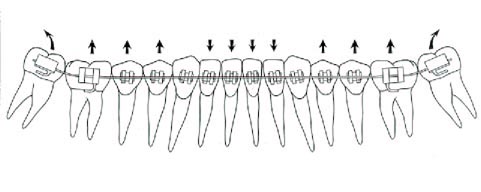
As with the standard edgewise appliance, the lower second molars must be included in the system as early as possible in the leveling and aligning stage. Complete bite opening is normally not possible until the lower second molars have been banded and leveling has proceeded to rectangular wires (Fig. 8).
Many of the principles of the standard edgewise system were likewise applicable to overjet reduction with preadjusted appliances. One difference was the tendency for upper and lower incisors to tip forward in the initial stages of preadjusted appliance treatment. In the upper arch, if not properly controlled, this creates a need for more incisor retraction and hence greater anchorage control during overjet reduction. In the lower arch, uncontrolled tipping makes it necessary to upright the incisors later with rectangular archwires, or to leave the buccal segments in a slightly Class II position after the overjet is corrected.
A second difference became apparent in the treatment of patients with severe overjets. The torque built into the incisor brackets was insufficient for such severe cases, and the upper incisors would often finish upright with inadequate torque, while the lower incisors were labially inclined and the buccal segments slightly Class II (Fig. 9). Of all the factors built into preadjusted appliances, incisor torque is the least reliable for many patients. Third-order bends are frequently required in the incisor region to compensate.
Space Closure
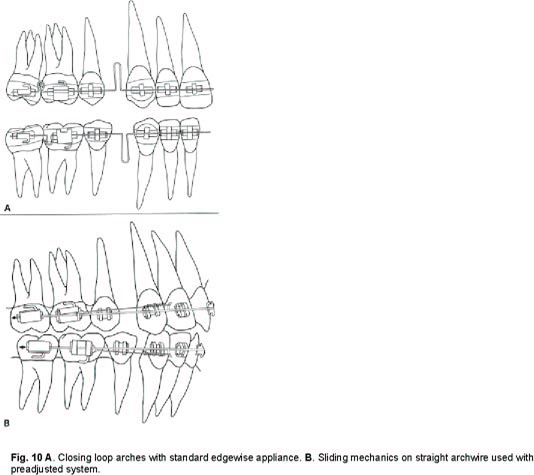
The most significant distinction between the mechanics of standard edgewise and preadjusted appliances was observed during space closure. With standard edgewise appliances, rectangular archwires did not effectively slide through the posterior bracket slots because of the 1st-, 2nd-, and 3rd-order bends. The orthodontist normally used a closing loop arch, which was activated in the office by opening the closing loop and moving the archwire through the posterior bracket slots (Fig. 10A).
The level bracket slot alignment of the new appliances allowed archwires, for the first time, to move more effectively through the posterior slots when the patient was not in the office. As a result, many orthodontists discontinued use of closing loops and began using various forms of sliding mechanics--for example, placing hooks in the anterior sections of straight archwires and tying elastics or springs to them from molar brackets (Fig. 10B).
Closing loop arches had several disadvantages:
1. Extra wire-bending time.
2. Poor sliding mechanics.
3. Tendency to run out of space for activation (after two or three activations, the omega loop contacted the molar bracket and the archwire had to be adjusted or remade).
4. High initial force levels.
They also had advantages:
1. Precise control of the amount of loop activation (often as little as 1mm), limiting the amount of initial tipping.
2. Adequate rebound time for uprighting between appointments (with minimal activations, loops closed quickly with little tipping).
Sliding mechanics had these advantages:
1. Minimal wire-bending time.
2. More efficient sliding of archwires through posterior bracket slots.
3. Sufficient space for activations.
But sliding mechanics at first also had disadvantages:
1. No established guidelines on amounts of force to be used during space closure.
2. Tendency for initial overactivation of elastic and spring forces, causing initial tipping and inadequate rebound time for uprighting.
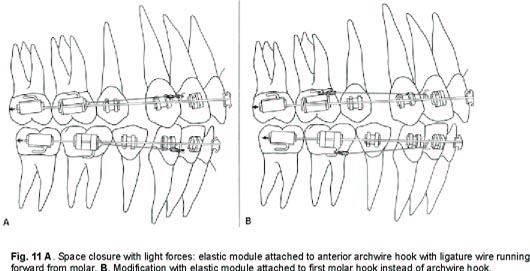
To maximize the advantages and minimize the disadvantages of sliding mechanics, we began reducing force levels during space closure. Instead of springs or overactivated elastics (which can produce 500g of force), we attach single elastic modules to anterior archwire hooks with ligature wires extended forward from the molars (Fig. 11). These "elastic tiebacks", when activated 2-3mm, generate about 100-150g of force.
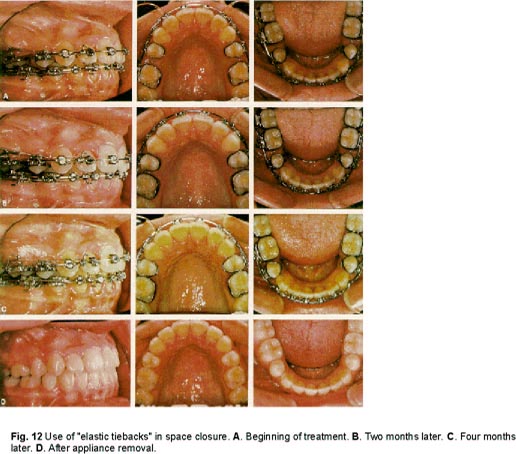
If the arches have been properly leveled, such light force allows for effective space closure; there is little tipping with subsequent binding of the archwires, and leveling is maintained (Fig. 12). We have found .019" x .025" archwires with .022" slots provide optimum rigidity, but adequate freedom for the wires to slide through the slots.
Constant attention is required to prevent any of the following inhibiting factors:
1. Inadequate leveling, resulting in archwire binding.
2. Posterior torque such that torquing and sliding cannot occur simultaneously.
3. Blockage of the distal end of the main archwire by a ligature wire.
4. Damaged or crushed brackets that bind the main archwire.
5. Soft-tissue resistance from build-up in extraction sites.
6. Cortical plate resistance from a narrowing of the alveolar bone in extraction sites.
7. Excessive force, causing tipping and binding.
8. Interferences from teeth or the opposing arch.
9. Insufficient force.
Finishing
The real value of preadjusted appliances became apparent in finishing: the more accurate the appliance, the less time and effort was required during this stage. The preangulated tip, torque, and in-out (including rotation control on the upper molars) allowed the orthodontist to spend less time treating the appliance with 1st-, 2nd-, and 3rd-order bends and more time treating the specific tooth-alignment needs of the patient.
Nevertheless, the misconception developed that no wire bending at all was required with the new preadjusted systems. Although it is true that very little bending is needed during the first five stages of treatment, finishing requires some wire bending in almost every case.
First, because the appliance prescriptions are based on averages, they cannot possibly account for all the variations of tooth size and shape. This means that detailing bends will be needed in the finishing wires of some patients.
Second, bracket placement is such an exacting requirement of preadjusted appliances that when brackets are not properly positioned, they must either be repositioned or compensating bends must be placed. It quickly became apparent that it was far more efficient to reposition brackets at strategic points in treatment (such as when including previously unerupted teeth) than to place compensating bends in all three planes of space during finishing.
Finally, wire bending is sometimes needed for overcorrection in the finishing stage as the case demands. We have found it easier to use a single appliance system with a few optional brackets than to keep on hand a wide variety of prescriptions and select one to meet the overcorrection needs of a given case. Areas of attention for overcorrection include:
1. Tip control. Most cases require little tip adjustment, but if, for example, a first molar is missing and the second molar is mesially inclined, a tipback bend will help upright the second molar.
2. Torque control. Torque adjustments of the upper and lower incisors are the most frequent compensatory bends because of the wide variations in beginning incisor positions, the distance these teeth need to be moved, and the desired finished positions. Torque adjustments can also be needed in the posterior segments, particularly for lower second molars that tend to tip lingually and for upper first and second molars that require additional buccal root torque.
3. Arch-width adjustment. Standardized archforms work well for most patients, but occasionally the form must be adjusted to compensate for disharmonies in arch width--most commonly the maxilla being narrow in relation to the mandible, requiring a widening of the upper archwire.
4. Rotation control. Most unwanted rotations can be controlled with rubber rotation wedges, Steiner rotation wedges, or lingual elastics. Upper and lower first molars are the exceptions; these teeth occasionally rotate mesiolingually because of the ligature ties to them during leveling and space closure. We correct a first molar rotation by placing an offset bend mesial to the affected molar.
5. Curve of Spee correction. If the upper and lower arches have not been completely leveled by this stage (usually a result of excessive force earlier in treatment), then bite-opening curves can be placed selectively during finishing.
ACKNOWLEDGMENT: The authors wish to express their thanks to Drs. L.F. Andrews and M.S. Berman for their help and encouragement during the development of concepts described in this article. [show_img]End.gif[/show_img]